
Introduction
Giant lung bullae have a large impact on respiratory mechanics1,2 and make ventilator management difficult in patients undergoing mechanical ventilation. The pathogenesis of lung bullae is varied. COPD-related emphysematous bullae are the most common type of lung bullae, whereas ventilator-associated lung bullae are rare. Treatment considerations include therapy for underlying disease, ventilation strategies to prevent progression of the bullous lung disease, and indications for surgical or bronchoscopic intervention. Although there are some treatment recommendations for COPD-related lung bullae,3,4 the role and timing of bullectomy for new-onset lung bullae during mechanical ventilation remain unclear. We describe our experience of treating a patient with severe bullous lung disease that developed during mechanical ventilation. We used ventilator management alone, without surgical intervention, to successfully treat the patient.
Case Summary
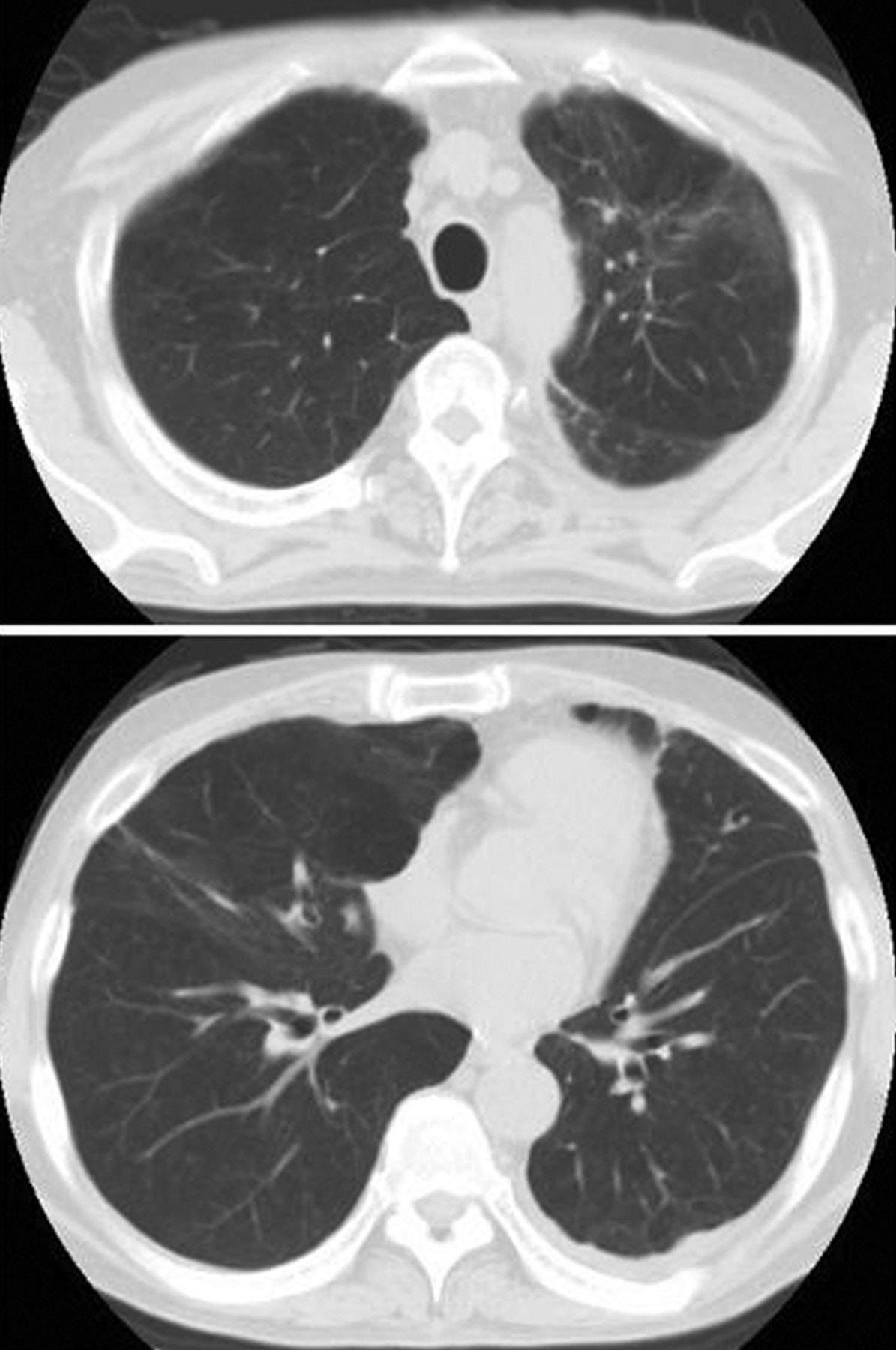
A 46-year-old man, who was a smoker and alcoholic, was admitted to the hospital because of severe community-acquired pneumonia. Computed tomogram on admission showed consolidation of the right lung (Fig. 1). He was intubated on the second hospital day, for hypoxic respiratory failure. Pressure controlled continuous mandatory ventilation was initially used, with an inspiratory pressure of 14 cm H2O, PEEP of 10 cm H2O, and FIO2 of 0.4. Arterial blood analysis showed PaO2 of 115 mm Hg. Both the sputum and blood cultures yielded Klebsiella pneumoniae, and he was treated with ceftriaxone. During ventilator weaning, he developed left-side pneumonia with complicated parapneumonic effusion, which was treated with tube thoracostomy and combination antibiotics.

Admission chest computed tomogram shows consolidation of the right lung, but no lung bullae.
Weaning was delayed because of this event. He underwent mechanical ventilation for 1 month, and chest radiograph revealed progressive hyperlucency of the right lung. He had respiratory distress, a respiratory rate of 25–30 breaths/min, sinus tachycardia, PaO2 of 79 mm Hg on FIO2 of 0.5, and PaCO2 was around 55 mm Hg, with mild acidemia, even with larger minute ventilation (14 L/min or 0.28 L/min/kg).
Computed tomogram revealed multiple bullae in the right upper and middle lobes and compression of adjacent lung tissue and the mediastinum (Fig. 2). Since the bullae markedly affected gas exchange, bullectomy was strongly advised to decrease the dead space and facilitate ventilator weaning. However, the patient's family refused surgical bullectomy and tracheostomy, so the treatment strategy focused on ventilator management and antibiotic therapy.
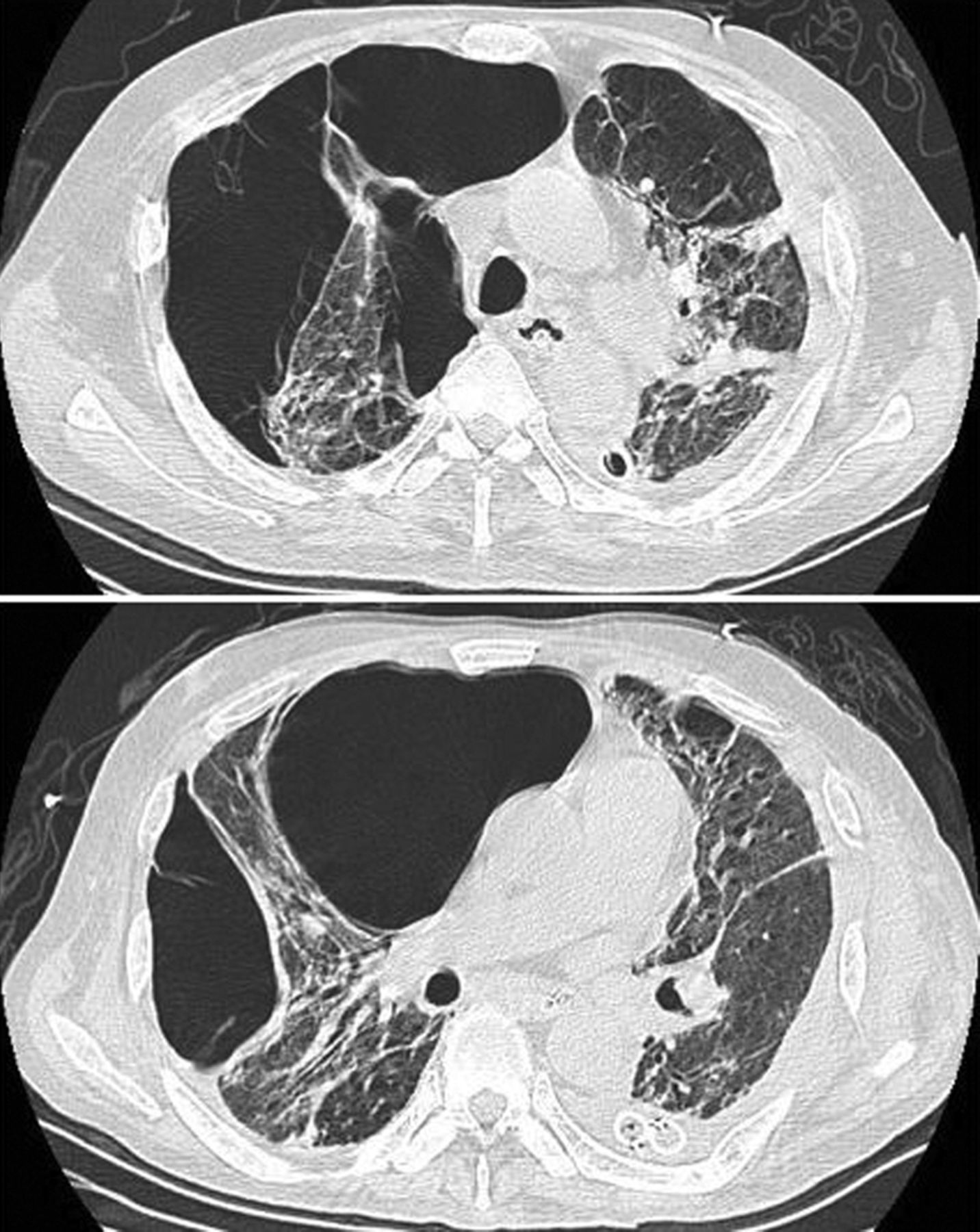
Computed tomogram after one month of mechanical ventilation shows multiple right-lung bullae and compression of the adjacent lung and heart.
We decreased PEEP from 5 cm H2O to 3 cm H2O, and drastically decreased the pressure support level if the respiratory rate was less than 35 breaths/min. To test for extubation readiness and to temporarily release the airway pressure, once or twice a day we conducted T-piece breathing via a 7.5-mm inner-diameter endotracheal tube, without PEEP or ventilatory assistance, with the patient in semi-recumbent position. The duration of T-piece breathing depended on the patient's tolerance. Subsequent chest radiographs showed a gradual resolution of the bullae. Three weeks after the appearance of the bullae, the patient was successfully weaned from the ventilator and discharged from the hospital. Computed tomogram at 2-month follow-up showed total resolution of the bullae (Fig. 3).

{kind=link}
{kind=link}
{kind=link}
Computed tomogram 2 months after discharge shows complete resolution of the bullae.
Discussion
A lung bulla is an air-space more than 1 cm in diameter, regardless of its pathogenesis.4–6 A pneumatocele is a type of lung bulla caused by check-valve phenomenon, and is classically considered to be related to localized bronchiolar necrosis due to acute pneumonia.7 In our patient several factors did not favor the diagnosis of pneumatocele. First, the bullae developed mainly in the right upper and middle lobes, but the pneumonia affected mainly the right lower lobe. Second, the bullae developed after the pneumonia had resolved, which is different from the usual course of pneumatoceles. Third, positive-pressure ventilation alone can contribute to the formation of bullae without check-valve mechanism. Positive-pressure ventilation could lead to distention of these air spaces, regardless of their pathogenesis. Reducing the impact of positive-pressure ventilation on the lung bullae is one of the major concerns in ventilator management.
Lung bullae can be idiopathic or associated with COPD, pulmonary infection, and/or mechanical ventilation. The most well studied bullous lung disease is COPD-related emphysematous bullae. The natural history and treatment outcome of lung bullae of other origin are unclear. Physiological analysis shows that giant bullae compress the adjacent lung parenchyma, increase dead space, and decrease the elastic recoil pressure of lung, thereby impairing gas exchange and increasing the work of breathing.1,2 Decompression of large bullae can improve lung function.1,8 Treatment options include surgical bullectomy and several transbronchial bronchoscopic methods.3,9–11
The indications of surgical bullectomy of COPD-related bullae are severe functional limitation despite maximal medical therapy, the bulla's occupying more than one third of the hemithorax (more ideal if the bulla occupies more than 50% of the hemithorax), no advanced emphysema in the non-bullous adjacent lung, and no important comorbidities.3,4,12 Although bullectomy and lung-volume-reduction surgery have been suggested for treating selected patients with COPD-related lung bullae,3,12 these cannot be used in all cases, particularly those of new-onset lung bullae during mechanical ventilation.
The variable pathogenesis of lung bullae affects the disease course and outcome. There is no well established treatment algorithm for lung bullae in mechanically ventilated patients. Few case reports have mentioned the ventilator strategies used.13,14 This case suggests that non-surgical management, including aggressive ventilator weaning, may successfully treat new-onset lung bullae, even severe, giant bullae that markedly impair gas exchange. However, risks in such non-surgical, ventilation-control management include patient-ventilator asynchrony, progression of bullae or emphysema, and life-threatening tension pneumothorax.
Airway pressure should be decreased as soon as possible in a patient with severe bullae. A practical difficulty associated with decreasing the airway pressure is determining the appropriate ventilation variable with which to adjust the inspiratory pressure, and the rate of decrease. Tidal volume is not the ideal variable to adjust, because the lung compliance is pseudo-high with a bullous lung. We think that respiratory rate is the better and practical variable to adjust and monitor the progress of reducing the inspiratory pressure. We allowed our patient a higher respiratory rate (up to 35 breaths/min) to decrease the inspiratory pressure. PaCO2 should be checked periodically. In our patient we used intermittent T-piece breathing to temporarily release the airway pressure and thus facilitate resolution of the bullae. The response to ventilator management can be assessed by monitoring the arterial blood gases, patient-tolerance duration of T-piece breathing, and chest radiographs.
The present case highlights that new-onset lung bullae during mechanical ventilation may be reversible if positive-pressure ventilation is discontinued as soon as possible. Drastically decreasing the airway pressure is the key strategy. Surgical bullectomy should be reserved for patients who fail repeated weaning attempts.
Teaching Points
The pathogenesis of lung bullae is variable, and the pathogenesis affects disease course and outcome. New-onset bullae during mechanical ventilation are potentially reversible if positive-pressure ventilation is discontinued.
Drastically decreasing the airway pressure is the key management strategy. Respiratory rate is a better variable than tidal volume to guide the progress of reducing the inspiratory pressure.
For new-onset lung bullae during mechanical ventilation, even giant bullae causing severe gas-exchange impairment do not suggest inevitable failure of non-surgical management.
Footnotes
- Correspondence: Sheng-Yuan Ruan MD, Department of Internal Medicine, National Taiwan University Hospital, No. 7 Chung-Shan South Road, Taipei 100, Taiwan. E-mail: syruan{at}ntu.edu.tw.
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.