

We read with great interest the article by Guérin and colleagues, in the November 2010 issue of Respiratory Care,1 describing analysis of acid-base disorders with the Stewart method versus the conventional approach in patients with chronic respiratory failure in stable or unstable respiratory condition. Unfortunately, we find several aspects of the analysis to be rather misleading.
First, according to the Stewart concept2 and as Guérin et al clearly explained, the blood pH depends on 3 independent variables: PCO2, the strong ion difference (which represents the net balance between strong positive ions and strong negative ions), and the total concentration of nonvolatile weak acids (Atot). As we know,3 weak acids, as opposed to strong ions, can exist at physiologic pH as dissociated (A–) or associated with a proton (AH):
Guérin et al calculated [Atot] with the formula:
Unfortunately, that formula is for [A–], not [Atot].4 The correct formula5 is:
Second, the techniques Guérin et al used for calcium (Ca2+) and magnesium (Mg2+) measurements give total concentrations. Hence, the ionized portions of Ca2+ and Mg2+ were not used to calculate the apparent strong ion difference, as is recommended.6 Thus, the apparent strong ion difference values, and therefore those of the strong ion gap, provided by Guérin et al are not quite correct. Consequently, the correction of these values could influence the study results. On the other hand, it is confusing that they used 2 variables (“unidentified strong anions” [XA] and strong ion gap) that belong to the same approach to quantify the unmeasured anions. Indeed, as Guérin et al provided the lactate concentration values, the determination of XA ([XA] = [strong ion gap] + [lactate]) had a little interest. Note also that lactate is not considered “unmeasured,” and the strong ion gap not only detects the presence of unmeasured strong ions but also unmeasured weak ions.3,7
Third, the standard base excess formula used to diagnose acid-base status according to what Guérin et al called “the conventional approach” (see their Equation 4) is the corrected standard base excess equation that updates the base excess to allow for change in Atot.6 Therefore, that standard base excess, as used in the study, does not belong to the conventional approach. Actually, the study did not compare the Stewart method to the conventional approach, but to more traditional ones, improved by the use of corrected standard base excess. Kellum6 called this a semi-quantitative approach in the reunification of acid-base physiology. We also think that the data presented cannot be used to assess the value of the Stewart method, since the calculations of Atot, apparent strong ion difference, and strong ion gap are in error.
Footnotes
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.
References
The author responds:
We thank Drs Mallat and Thevenin for their comments. Their points are well taken and correct, and we would like to address each of them.
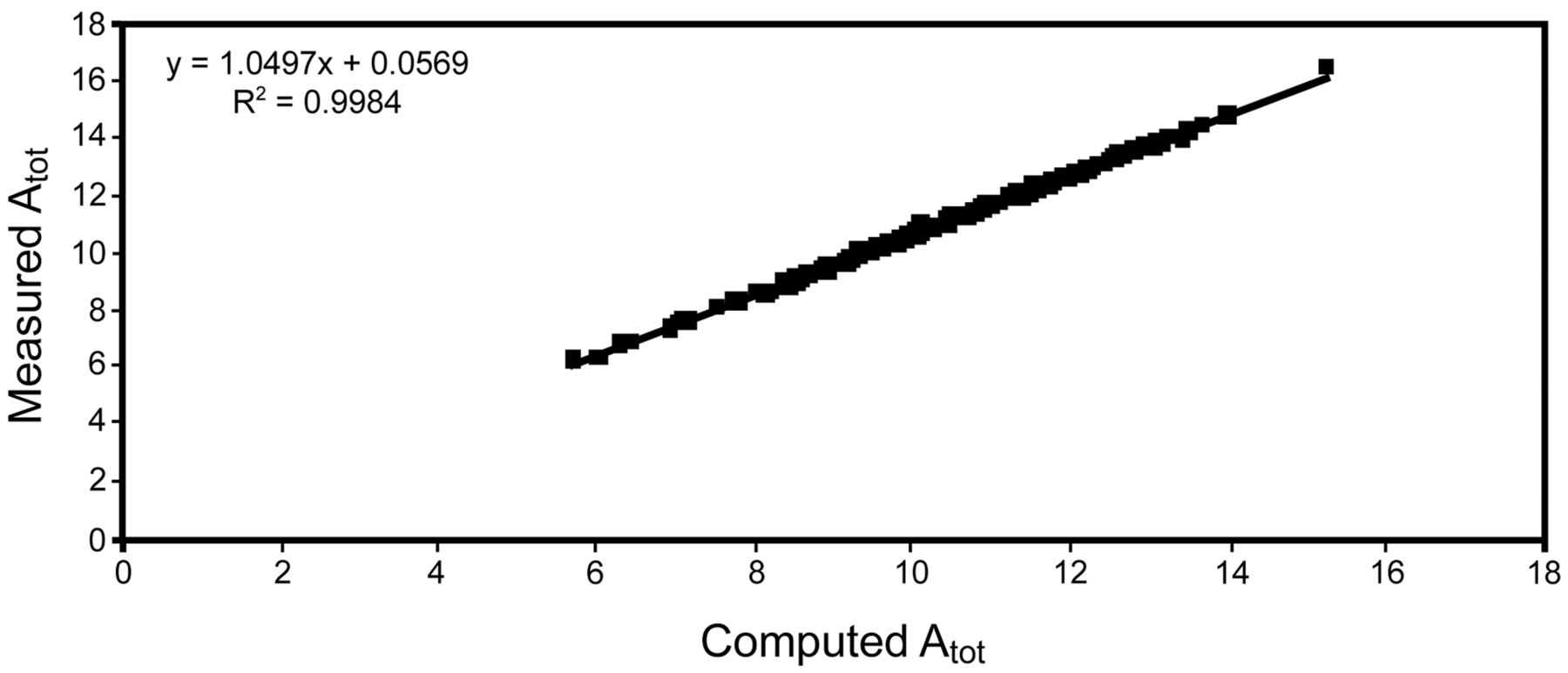
First, it is true that the way we used Atot applies for A– and not Atot. However, computing Atot as [A–] [1 + 10 (pKa – pH)] in our data1 by taking the value of 6.12 for pHa2 resulted in a minor difference (Fig. 1). The bias amounted to 0.57 mmol/L.
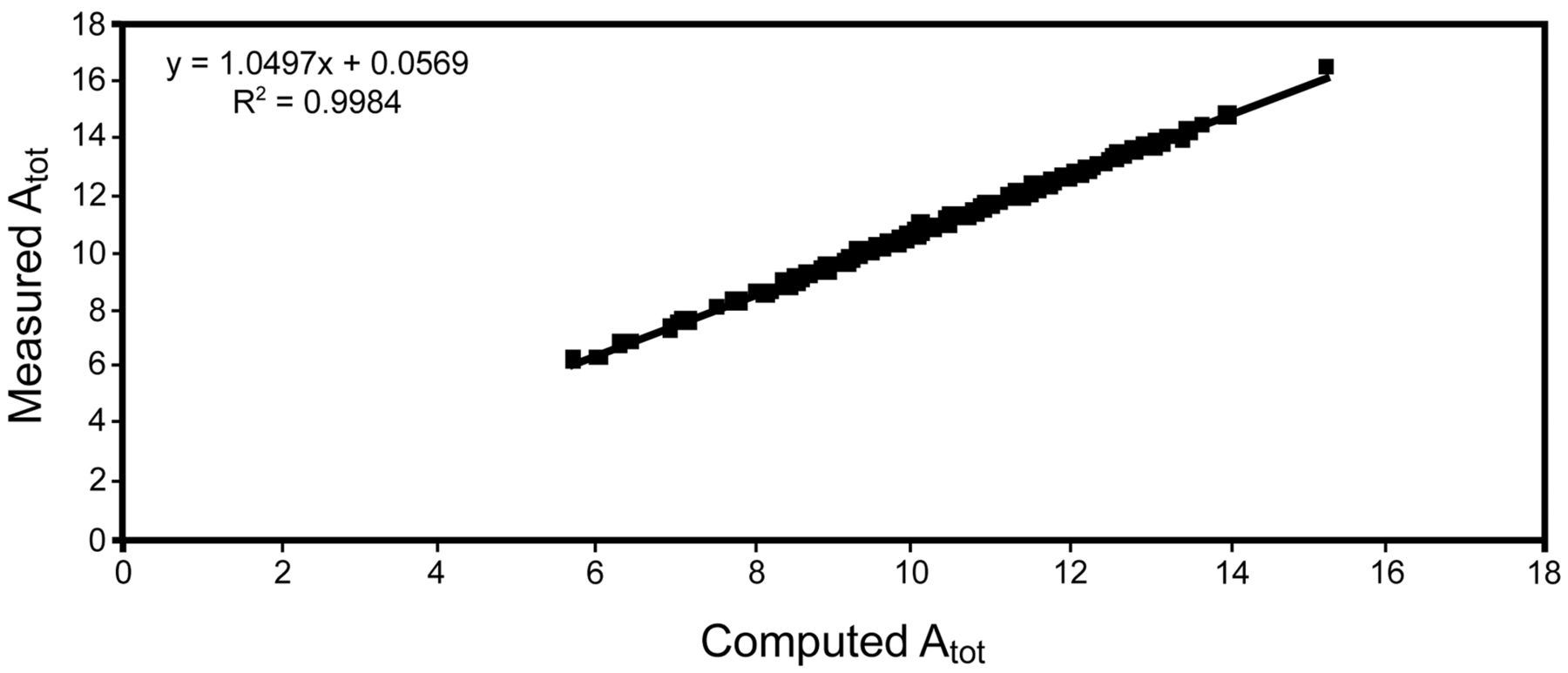
Relationships between the original values of total concentration of nonvolatile weak acids (Atot) and the Atot values computed from the equation Atot = [A–] [1 + 10 (pKa – pH)].
Second, it is true that we measured total plasma calcium and magnesium instead of their ionized counterparts. We agree that it is not correct to use the total concentration (free + protein-bound) of some ions in the apparent-strong-ion-difference equation. It is, however, unlikely that this would markedly change the value of the apparent strong ion difference. The weight of calcium and magnesium in the apparent strong ion difference is low, and some authors simplified the computation of apparent strong ion difference toward the difference between Na+ and Cl–.3 Constable and Stämpfli2 stressed that accurate measurement of apparent strong ion difference in human plasma may be difficult, and computed it via 3 formulae:
The corresponding mean ± SD values of the apparent strong ion difference in the venous blood of 8 humans (see Table 2 in reference 2) were 40.9 ± 2.9 mEq/L, 40.0 ± 2.9 mEq/L, and 43.0 ± 2.9 mEq/L, respectively. The measurements were on normal plasma and did not pertain to patients. Furthermore, the amount of calcium electrostatically bound to plasma protein is 0.8 mmol, as compared to 36 mmol for Na+.2
We presented unidentified strong anions (XA) and strong ion gap not to confuse the reader but because we found it interesting to describe these 2 ways to bridge the gap between the various measured ions.
Third, you are correct in that the standard base excess is an update of the conventional approach, and it would have been more appropriate to read it as such.
Finally, we stress that, even though our computations of Atot, apparent strong ion difference, and strong ion gap were not accurate (strong ion gap was not correct because apparent strong ion difference was not), it remains that the values of the effective strong ion difference were correct in our study. Therefore, in our study the comparisons between the 4 chronic-respiratory-failure groups were correct on that basis, as was the distinction between the acid-base disorders categories from the Stewart approach.
Footnotes
-
The author has disclosed no conflicts of interest.









{kind=link}