

Abstract
BACKGROUND: The combination of high PEEP and low tidal volume (VT) decreases some risks of mechanical ventilation, including pulmonary overdistention, damage due to cyclic opening and closing of the alveoli, and inflammatory responses that can lead to multiple-organ dysfunction. We hypothesized that high VT and high PEEP induce mesenteric microcirculatory disturbances and that those disturbances would be attenuated by pentoxifylline, which is anti-inflammatory.
METHODS: We anesthetized (isoflurane 1.5%), tracheostomized, and mechanically ventilated 57 male Wistar rats with PEEP of 10 cm H2O and FIO2 of 0.21 for 2 hours. One group received low VT (7 mL/kg), another group received high VT (10 mL/kg), and a third group received high VT plus pentoxifylline (25 mg/kg). We measured mean arterial pressure, respiratory mechanics, mesenteric blood flow, and leukocyte-endothelial interactions.
RESULTS: The mean arterial pressure was similar among the groups at baseline (108 mm Hg [IQR 94–118 mm Hg]) and after 2 hours of mechanical ventilation (104 mm Hg [IQR 90–114 mm Hg]). Mesenteric blood flow was also similar between the groups: low VT 15.1 mL/min (IQR 12.4–17.7 mL/min), high VT 11.3 mL/min (IQR 8.6–13.8 mL/min), high-VT/pentoxifylline 12.4 mL/min (10.8–13.7 mL/min). Peak airway pressure after 2 hours was lower (P = .03) in the low-VT group (10.4 cm H2O [IQR 10.2–10.4 cm H2O]) than in the high-VT group (12.6 cm H2O [10.2–14.9 cm H2O]) or the high-VT/pentoxifylline group (12.8 cm H2O [10.7–16.0 cm H2O]). There were fewer adherent leukocytes (P = .005) and fewer migrated leukocytes (P = .002) in the low-VT group (5 cells/100 μm length [IQR 4–7 cells/100 μm length] and 1 cell/5,000 μm2 [IQR 1–2 cells/5,000 μm2], respectively) and the high-VT/pentoxifylline group (5 cells/100 μm length [IQR 3–10 cells/100 μm length] and 1 cell/5,000 μm2 [IQR 1–3 cells/5,000 μm2], respectively) than in the high-VT group (14 cells/100 μm length [IQR 11–16 cells/100 μm length] and 9 cells/5,000 μm2 [IQR 8–12 cells/5,000 μm2], respectively).
CONCLUSIONS: Low VT with high PEEP was lung-protective, and early pentoxifylline reduced the inflammatory response to high VT with high PEEP (and presumed lung overdistention) during mechanical ventilation.
- mechanical ventilation
- pentoxifylline
- PEEP
- leukocyte-endothelial interactions
- intravital microscopy
- ventilator-induced lung injury
- tidal volume
- mesentery
Introduction
PEEP during mechanical ventilation is believed to improve oxygenation. The combination of high PEEP and low tidal volume (VT) during mechanical ventilation is a protective strategy that decreases the risk of pulmonary overdistention, damage due to cyclic opening and closing of the alveoli, and inflammatory responses that can lead to multiple-organ dysfunction.1–3 However, PEEP increases intrathoracic pressure, which can reduce venous return and cardiac output, and redistribute blood flow away from the splanchnic vasculature.4–6 Hypoperfusion and ischemia in the gastrointestinal tract are associated with loss of tract barrier and systemic inflammation,7 which may play a pivotal role in the pathogenesis of several complications associated with mechanical ventilation,8–10 including multiple-organ failure in patients with severe sepsis and cardiac failure, a situation that usually has a very poor outcome.11–13
Therapies directed at improving microcirculation and local/systemic cellular perfusion may improve outcomes. Pentoxifylline (pentoxifylline 1-(5-oxohexyl)-3,7-dimethylxanthine) is a methylxanthine derivative and a nonspecific phosphodiesterase-inhibitor associated with increased deformability of red blood cells14 and with reduced blood viscosity,15 which are 2 factors that might improve blood flow. Pentoxifylline improved the integrity and permeability of the gut barrier, bacterial translocation, neutrophil activation, endothelial dysfunction, blood flow, lung oxygenation, and overall survival in models of acute lung injury,16,17 hemorrhagic shock/reperfusion,18,19 and sepsis.20 In humans, pentoxifylline inhibited the production of tumor necrosis factor alpha in alveolar macrophages.21 In contrast, in animal models of multiple-organ dysfunction22 and in patients with severe septic shock,23 pentoxifylline did not improve outcomes.
Intravital microscopy is a live-imaging technique used in animal models of hemorrhagic shock/reperfusion and sepsis.19,23–25 We recently found that injurious mechanical ventilation with a high VT (10 mL/kg) and a PEEP of 10 cm H2O markedly increased leukocyte-endothelial interactions in rat mesentery.26 Lung-protective ventilation is the only treatment that has been shown to decrease mortality in patients with ARDS. Because of the severity of the underlying disease, in many patients it is not possible to provide a ventilation strategy that will protect all lung units, so a pharmacologic therapy that modulates the inflammatory response would be beneficial. We investigated the effects of early pentoxifylline in mechanically ventilated rats.
Methods
This study was approved by and under the license of the Institutional Animal Care and Use Committee of the Heart Institute, Faculdade de Medicina da Universidade de São Paulo, and was performed according to the United States National Institutes of Health guidelines for the use of experimental animals.
Animals
Fifty-seven adult male Wistar rats (mean ± SD weight 253 ± 27 g) were housed for 3–5 d before the experiment, with unrestricted access to food and water. In the experiment the animals were first anesthetized with sodium pentobarbital (50 mg/kg, intraperitoneal), then we cannulated the right carotid artery and jugular vein with PE50 tubing, and tracheotomized with PE45 tubing for spontaneous breathing. We then randomly assigned the animals to 3 groups: low VT (VT = 7 mL/kg) (no. = 19), high VT (VT = 10 mL/kg) (no. = 19), and high VT plus pentoxifylline (25 mg/kg) at the beginning of mechanical ventilation (no. = 19). We continued anesthesia with isoflurane (1.5%)26 during the 2 hours of mechanical ventilation, with a PEEP of 10 cm H2O on room air. The respiratory rate was set at 70 breaths/min in the high-VT and high-VT/pentoxifylline groups, and at 80 breaths/min in the low-VT group, to maintain normocapnia. All the animals received an infusion of saline (100 μL/100 g body weight).
Hemodynamics Measurements
At baseline and after 2 hours of mechanical ventilation we recorded blood pressure (MK-III-S, Narco Bio-Systems, Austin, Texas). Via laparotomy we gently dissected the superior mesenteric artery from the surrounding tissue and measured mesenteric artery blood flow with an ultrasound transit-time flow probe (2SB545, Transonic Systems, Ithaca, New York) placed around the artery.
Respiratory Mechanics Measurements
We collected data as previously reported,27 at the beginning of mechanical ventilation and after 2 hours of mechanical ventilation. We measured peak airway pressure (Paw) with a differential pressure transducer (142PC05D, Honeywell, Freeport, Illinois) connected to a side tap in the tracheal cannula. We measured air flow (V̇) with a pneumotachograph (Fleish 4–0, OEM Medical, Richmont, Virginia) connected to the tracheal cannula and to a differential pressure transducer (163PC01D36, Honeywell, Freeport, Illinois). We measured lung-volume changes (V) via electronic integration of the V̇ signal. We averaged 10 respiratory cycles for each data point. Wecalculated respiratory system elastance (ERS) and resistance (RRS) with the linear equation of motion:
Blood Gas Analysis
We conducted arterial blood gas analysis (ABL 555, Radiometer Medical, Copenhagen, Denmark) 5 min after beginning mechanical ventilation (baseline), and 2 hours after beginning mechanical ventilation.
Intravital Microscopy of the Mesentery
All the animals were kept under mechanical ventilation during intravital microscopy, as previously described.24–26 After midline abdominal incision, the distal ileum and its accompanying mesentery is exposed for examination of the microcirculation. The animal is placed in the right lateral decubitus on a warmed (37°C) stage, and the mesentery is transilluminated and kept moist with continuous applications of warm (37°C) Krebs solution. Care is taken during handling to prevent physical damage. Mesenteric microcirculation is assessed after 10 min of stabilization, then 3–5 post-capillary venules are selected by their diameters (approximately 20 μm) and examined once. A charge-coupled device (CCD) color camera (TK-C1380U, JVC, Tokyo, Japan) is incorporated with a triple-ocular microscope (Axioplan 2, Zeiss, München, Germany), which sends the signal (magnification 1,960) to a computer monitor (SyncMaster 753DFX, Samsung, Manaus, Brazil). Analyses of leukocyte-endothelial interactions were performed with image acquisition and analysis software (Axiovision 4.1, Zeiss, München, Germany). We counted the number of rolling leukocytes as the number of white cells that passed a designated line perpendicular to the venular axis during a 10-min period.24–26,28 We counted the number of adherent cells as the number of cells that remained stationary for > 30 seconds on a 100-μm segment of the venular endothelium during a 10-min period.24–26,28 We counted the number of migrated leukocytes as the number of cells accumulated at the connective tissue, adjacent to the chosen postcapillary venule, in a standard area of 5,000 μm.24–26
Lung Histology
At the end of the experiment, the animal was exsanguinated by cutting the abdominal aorta. The lungs were then gently inflated (10 mL/kg), removed, and fixed with 10% formalin solution in sodium phosphate buffer (0.2 mol/L, pH 7.2) for 24 hours. The lungs were ethanol dehydrated and embedded in paraffin. Three lung sections (5 μm) were cut from the apex to the base and stained with hematoxylin and eosin. Examination, as previously reported,24,26 was performed by 2 observers. We attached a 104 μm2, 100-point grid to the ocular lens of the microscope (magnification 1,000), and randomly chose 12–20 fields in each section (3–5 per animal), then quantified the edema volume index (volume fraction of perivascular and interstitial edema divided by total perivascular tissue), the polymorphonuclear cell density (cells/104 μm2) in the perivascular and interstitial tissue, and the polymorphonuclear cell density (cells/104 μm2) in the alveolar septa.
Statistical Analysis
We chose the sample size for this study based on our previous experiments on mesenteric leukocyte-endothelial interactions.19,24–26 We report the data as median and interquartile range (IQR). We compared the groups with the Kruskal-Wallis test, and tested differences between groups with the Dunn Test. We tested differences between periods with the Wilcoxon signed rank test. P values < .05 were considered significant.
Results
Hemodynamics
Mean arterial blood pressure was similar at baseline and after 2 hours and also between groups: low VT 98.5 mm Hg (IQR 94.0–108.3 mm Hg) and 98.0 mm Hg (IQR 78.0–123.3 mm Hg), respectively; high VT 117.0 mm Hg (IQR 94.3–131.5 mm Hg) and 107.5 mm Hg (IQR 86.3–128.0 mm Hg), respectively; and high-VT/pentoxifylline 111.5 mm Hg (IQR 92.3–119.5 mm Hg) and 106.0 mm Hg (IQR 92.5–113.5 mm Hg), respectively. There were no significant differences in mesenteric blood flow between groups: low VT 15.1 mL/s (IQR 12.4–17.7 mL/s); high VT 11.3 mL/s (IQR 8.6–13.8 mL/s); and high-VT/pentoxifylline 12.4 mL/s (IQR 10.8–13.7 mL/s), respectively.
Arterial Blood Gases and Lactate
At baseline there were no significant differences between the groups in pH, PaCO2, or lactate (Table 1). PaO2 was within normal range in all 3 groups, but was higher in the high-VT/pentoxifylline group than in the low-VT group. After 2 hours of mechanical ventilation, oxygenation increased in the low-VT group and high-VT group, and remained higher in the high-VT/pentoxifylline group. PaCO2 and pH were similar in all groups at baseline and at 2 hours. Lactate improved in the low-VT group and the high-VT/pentoxifylline group, compared to the high-VT group.
Arterial Blood Gas and Lactate Values*
Respiratory Mechanics
Peak airway pressure was lower in the low-VT group than in the high-VT group or the high-VT/pentoxifylline group (Table 2). Respiratory system elastance increased and respiratory system resistance decreased in all 3 groups.
Respiratory Mechanics Data*
Mesenteric Leukocyte-Endothelial Interactions
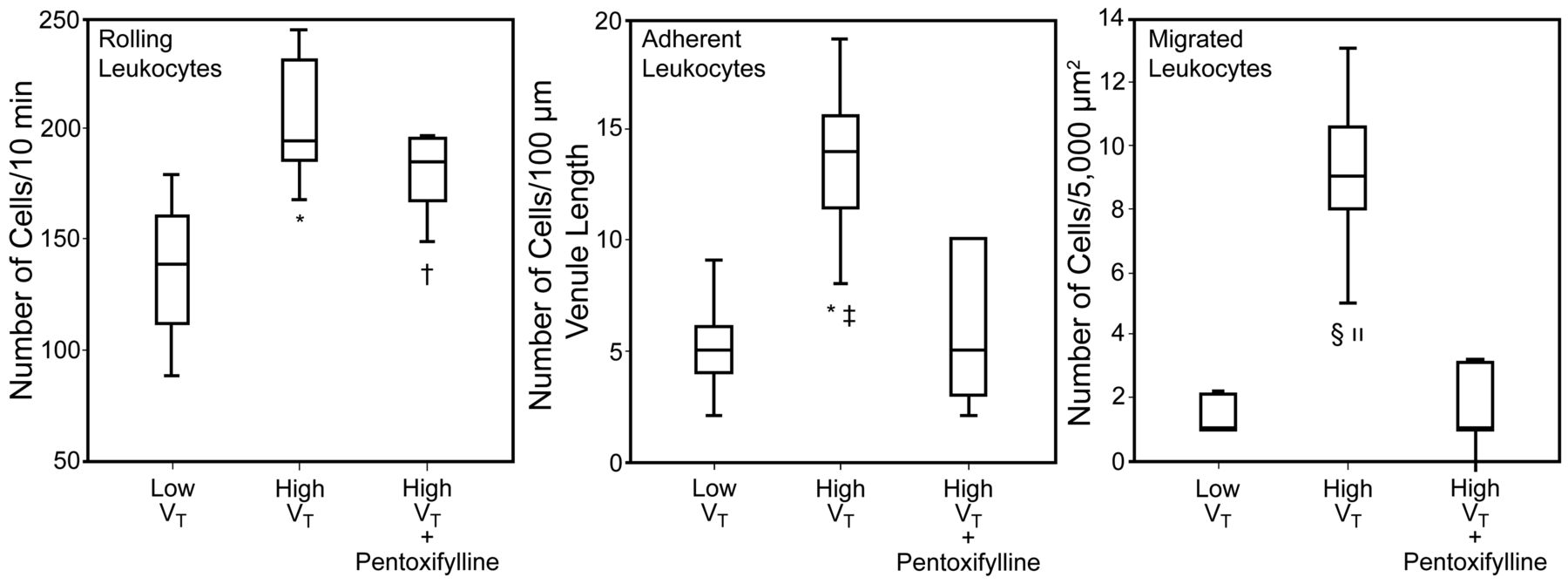
Table 3 shows the microvessel diameter and leukocyte data. Figure 1 also shows the leukocyte data.
Microvessel Diameters and Leukocyte Data*

Rolling leukocytes, adherent leukocytes, and migrated leukocytes in postcapillary venules in the mesentery of rats, after 2 hours of mechanical ventilation with either low tidal volume (VT) (n = 6), high VT (n = 7), or high VT plus early pentoxifylline (n = 5). * P = .002 versus low VT. † P = .03 versus high-VT/pentoxifylline. ‡ P = .01 versus high-VT/pentoxifylline. § P = .001 versus low VT. ‖ P = .003 versus high-VT/pentoxifylline.
Lung Neutrophil Infiltration and Edema
There was no intra-alveolar hemorrhage or hyaline membrane in any of the groups. Table 4 shows the neutrophil infiltration in the alveolar septa and perivascular tissue, and edema in the perivascular tissue. Neutrophil infiltration in the perivascular and interstitial tissue was significantly higher in the high-VT group than in the low-VT group (P < .001). Compared to the low-VT group and the high-VT/pentoxifylline group, the high-VT group had more neutrophil infiltration in the alveolar septa, which was associated with more interstitial and perivascular tissue edema (Fig. 2).
Neutrophil Infiltration in the Alveolar Septa and Perivascular Tissue, and Edema in the Perivascular Tissue
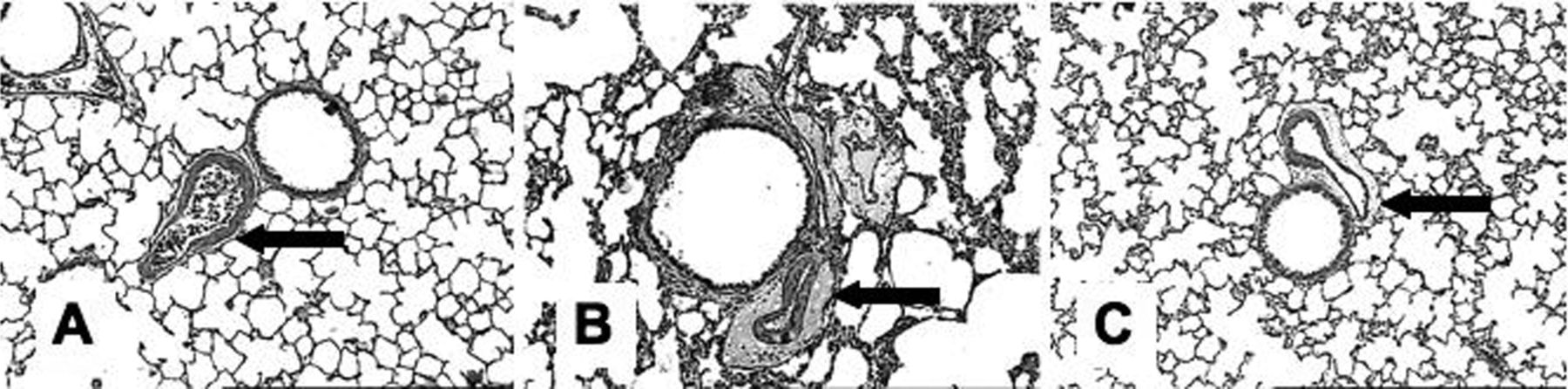
Representative photomicrographs of rat lung. The vessels are branches of the pulmonary artery at the terminal bronchiolar level, and are of the same magnitude. The arrows point to edema in the perivascular and interstitial tissue. A: Low tidal volume (VT). B: High VT. C: High VT plus early pentoxifylline. There is more edema in the perivascular and interstitial tissue in the high-VT group than in the low-VT or high-VT/pentoxifylline groups. Magnification 100, hematoxylin and eosin stain.
Discussion
Baseline oxygenation was higher in the high-VT group and the high-VT/pentoxifylline group than in the low-VT group. It appears that high-VT ventilation transiently increased oxygenation and caused inflammatory response at 2 hours, compared to low-VT ventilation. Early pentoxifylline helped maintain oxygenation, perhaps because pentoxifylline's mild vasodilation properties improved gas exchange by the capillaries.
Early pentoxifylline appeared to reduce the inflammatory response from ventilator-induced lung injury. Most patients with acute lung injury require mechanical ventilation, which can cause lung injury, and high ventilator settings are associated with a mortality rate of 35–65% in acute respiratory distress syndrome, usually from progressive dysfunction of vital organs.29,30 Several studies have shown an association between mechanical ventilation and exacerbated pulmonary inflammatory response and increased alveolar capillary permeability.1–3,31 Other studies have found protective effects from PEEP and low VT in patients with injured lungs1,3,32–34 and non-injured lungs.35 Recently, Dos Santos et al32 reported a 20–40% deterioration of pulmonary compliance in rats ventilated with a high VT (12 mL/kg), versus low VT (6 mL/kg), after 2–4 hours of mechanical ventilation. They demonstrated that acute ventilator-induced lung injury can be biochemically and biophysically distinguished early in the progression of the injury, with microarray and bioinformatic techniques. In the present study, the rats had an increase in peak airway pressure (approximately 15%), a decrease in resistance (approximately 10%), and a substantial increase in elastance (approximately 22%). Lung injury was marked in the high-VT group, as indicated by more edema and neutrophils in the parenchyma and perivascular tissue. In contrast, low VT induced only small amounts of neutrophil infiltration and edema. Similarly, early pentoxifylline attenuated ventilator-induced lung injury. Our results are consistent with those from Lessa et al,36 that pentoxifylline decreases inflammatory lung injury in rats mechanically ventilated with VT of 20 mL/kg, and from Yada-Langui et al,19 who found that pentoxifylline attenuated lung inflammatory response in a hemorrhagic shock/reperfusion rat model.
Microcirculatory integrity has a key role in adequate tissue oxygenation and organ function, which may be crucial in the prognosis of critically ill patients.11–13 Leukocytes circulate in the bloodstream and migrate into the tissues in response to signals released in the microenvironment of infection and tissue injury. Leukocyte-endothelial interactions are essential for effective defense from bacterial invasion. However, leukocyte over-activation and increased leukocyte accumulation in the perivascular tissue can be associated with an exaggerated pro-inflammatory immune response that can contribute to widespread microvascular injury and consequent endothelial damage.7,24–26 Hypoperfusion of the gastrointestinal vascular bed has been suggested as a potential mechanism for the development of several complications from mechanical ventilation in critically ill patients.8–10 We recently found that high intrathoracic pressure generated by high VT (10 mL/kg) and high PEEP (10 cm H2O) increased leukocyte-endothelial interactions in rat mesentery, as compared to PEEP values of 0 and 5 cm H2O, with no significant differences in mean arterial blood pressure between the groups.26 In the present study we used that same rat model and found that high VT and high PEEP had similar deleterious effects on mesenteric leukocyte-endothelial interactions.
We choose PEEP of 10 cm H2O, because in a separate study (unpublished data) with surfactant-depleted rats we found that both maximum lung compliance and oxygenation were achieved at a PEEP of 12 cm H2O, whereas the rats in the present study had healthy lungs. In healthy anesthetized piglets, PEEP of 16 cm H2O resulted in hyperinflation that decreased when PEEP was progressively reduced to around 10 cm H2O.37 Because of the severity of the underlying disease, in many patients it is not possible to provide a ventilation strategy that will protect all lung units, so a pharmacologic therapy that modulates the inflammatory response would be beneficial.
A novel finding of the present study is that, compared to high VT, low VT attenuates over-activation and leukocyte accumulation in the mesenteric perivascular tissue, without affecting lung elastance. This suggests that lung injury and acute inflammatory response start early in mechanical ventilation, prior to alteration of lung mechanics. In addition, pentoxifylline attenuates leukocyte-endothelial interactions at the mesentery after 2 hours of mechanical ventilation with high VT and high PEEP. Taken together, these results show systemic inflammation induced by alveolar overdistention during high VT and suggest that low VT prevents mesenteric microcirculatory derangements, and that pentoxifylline during high VT modulates adherence and migration at the mesentery and improves blood lactate. These pentoxifylline benefits were probably related to reduced lactate production, antithrombotic activity,38 increase red-blood-cell deformability,13 and attenuation of the inflammatory response.18,39,40
Limitations
To access the mesenteric microcirculation we performed a midline abdominal incision to expose the mesentery for intravital microscopy and the mesenteric artery for flow measurements. This could, in principle, interfere with the microcirculation. However, the abdomen was kept closed during the study period and during all the other measurements. One could argue that PEEP decreases intestinal blood flow in proportion to the applied PEEP level, as previously reported.5,6 We did not measure intrapulmonary pressure. However, we set PEEP at 10 cm H2O in all the animals, and despite differences between the groups in respiratory rate (80 breaths/min in the low-VT group vs 70 breaths/min in the high-VT and high-VT/pentoxifylline groups) and VT (7 mL/kg in the low-VT group vs 10 mL/kg in the high VT and high-VT/pentoxifylline groups), the mean arterial blood pressure and mesenteric blood flow were not different between the groups, which suggests a blood-flow-independent inflammatory response as a result of biotrauma during mechanical ventilation. A likely explanation is inflammatory mediator translocation from pulmonary to systemic circulation following mechanical ventilation.
Another limitation is that we did not measure adhesion molecules. However, we previously found positive correlations between the expression of P-selectin and intercellular molecules with leukocyte-endothelial interactions at the mesentery and lungs after hemorrhagic shock/reperfusion and sepsis.7,19,24 And in the present study we found significant differences in leukocyte-endothelial interactions between the groups, which were not associated with hemodynamics. The increased leukocyte adhesion and migration to the perivascular tissue at the mesentery (distant locale) may have been induced by systemic inflammation biotrauma, which was prevented by low VT and attenuated by pentoxifylline. Moreover, our findings were obtained in rats with normal lungs submitted to 2 hours of mechanical ventilation, and we must be very cautious in interpreting the data relative to mechanically ventilated patients.
Conclusions
Two hours of mechanical ventilation with high VT and high PEEP were harmful to mesenteric microcirculation and the lungs of rats, whereas low VT with high PEEP protected the lungs and mesenteric microcirculation, and early pentoxifylline attenuated lung and mesenteric inflammation during high VT and high PEEP. These findings suggest that early pentoxifylline might decrease the risk of ventilator-induced microcirculatory derangements and lung injury.
Acknowledgments
We thank Julia Fukushima for help with statistical analysis. The platform for intravital microscopic study of the rat mesentery was developed by Naomi Kondo Nakagawa, Simão Bacht, and Idágene Cestari.
Footnotes
- Correspondence: Naomi Kondo Nakagawa PT MSc PhD, Department of Physiotherapy, Communication Science and Disorders, and Occupational Therapy, Faculdade de Medicina da Universidade de São Paulo, LIM 34, Avenue Dr Arnaldo, 455 Room 1150, Cerqueira Cesar CEP, 01246-903 São Paulo, Brazil. E-mail: naomi.kondo{at}usp.br.
This study was partly supported by grant FAPESP 07/51605-9 from Fundação de Amparo à Pesquisa do Estado de São Paulo, São Paulo, Brazil.
The authors have disclosed no other conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}