
Abstract
BACKGROUND: Recent studies have demonstrated a greater prevalence in exercise-induced bronchospasm (EIB) in obese adolescents. However, the role of pro-/anti-inflammatory adipokines and the repercussions of obesity treatment on EIB need to be explored further. Therefore, the objective of this study was to evaluate the role of pro-/anti-inflammatory adipokines on EIB in obese adolescents evaluated after long-term interdisciplinary therapy.
METHODS: Thirty-five post-pubertal obese adolescents, including 20 non-EIB (body mass index [BMI] 36 ± 5 kg/m2) and 15 EIB (BMI 36 ± 5 kg/m2), were enrolled in this study. Body composition was measured by plethysmography, using the BOD POD body composition system, and visceral fat was analyzed by ultrasound. Serum levels of adiponectin and leptin were analyzed. EIB and lung function were evaluated according to the American Thoracic Society criteria. Patients were recruited to a 1-year interdisciplinary intervention of weight loss, consisting of medical, nutritional, exercise, and psychological components.
RESULTS: Anthropometrics and lung function variables improved significantly after the therapy in both groups. Furthermore we observed a reduction in EIB occurrence in obese adolescents after treatment. There was an increase in adiponectin levels and a reduction in leptin levels after the therapy. In addition, a low FEV1 value was a risk factor associated with EIB occurrence at baseline, and was correlated after treatment with changes in anthropometric and maximal O2 consumption values as well as the adipokines profile.
CONCLUSIONS: In the present study it was demonstrated that 1 year of interdisciplinary therapy decreased EIB frequency in obese adolescents, paralleled by an increase in lung function and improvement in pro-/anti-inflammatory adipokines.
- obesity
- adolescents
- adipokines
- bronchospasm
- exercise-induced
- treatment
- interdisciplinary studies
Introduction
Obesity is a multi-factorial condition that leads to social, psycho-social, and health problems.1 In 1997, the World Health Organization declared obesity to be a global epidemic condition.2 According to the last survey, approximately 49% of the adult Brazilian population is currently obese or overweight. In addition, the prevalence of obesity in adolescents has more than doubled in the last 20 years.3 The health risks associated with obesity include effects on the respiratory system.4 The increase in fat deposits has been associated with a reduction in lung volume4,5 and exercise-induced bronchospasm (EIB).6–8
EIB is defined as a 15% reduction in FEV1 due to the airway obstruction that occurs in association with exercise, without regard to the presence of chronic asthma.9 Recent studies have observed that the prevalence of EIB is greater in obese non-asthmatics, compared to non-obese individuals.6,7,10 Another study did not find any difference in EIB prevalence between non-asthmatic obese and non-obese boys.11
Collectively, these reports indicate that exercise tolerance may be lower, lung function may be compromised, and inflammation was up-regulated in obese, compared to lean, individuals.6–8,12 In this sense, previous studies observed a positive association between leptin levels and airway hyper-responsiveness.13,14 On the other hand, the adiponectin level has been shown to be a protective factor for asthma.15 However, obese subjects present hyperleptinemia and/or leptin resistance, as well as hypoadiponectinemia.16,17 These physiological changes may also be the mechanism linking increased fat deposits with reported EIB.4 Moreover, the adiponectin/leptin ratio has been used a biomarker for the inflammatory process related to obesity; however, the role of these interactions with EIB frequency has not been well explored.
There are multiple treatments for EIB, which can be divided into pharmacologic and non-pharmacologic categories. Pharmacologic agents include short- and long-acting β2 adrenoceptor agonists, anti-cholinergics, mast cell stabilizing agents, inhaled corticosteroids, and leukotriene receptor antagonists.18,19 Previous studies have demonstrated the effectiveness of these medications for reducing the occurrence of EIB.20,21 However, other studies have demonstrated that there are some limitations of pharmacologic therapy, such as potential side effects, the effectiveness of each medication, the frequency of administration, the duration of action, bad taste, and tolerance level.21–24
Non-pharmacologic management includes physical conditioning, incorporating a warm-up before and a cool-down period after exercise, nasal breathing, avoidance of cold weather or environmental allergens, and using a face mask or other aid to warm and humidify inhaled air.19 Dietary modifications may also play a role in EIB. In this manner, Mickleborough et al25 demonstrated that dietary supplementation with fish oil for 3 weeks reduced symptoms of EIB in asthmatics, with less than a 10% fall in post-exercise FEV1. Despite many studies being conducted to date, there is no single agent that has been consistently shown to prevent EIB; moreover, the majority of the studies were with asthmatic patients.25–27 The goal of therapy is to allow patients with EIB to participate in vigorous activity without symptoms and difficulty.18 Although the level of evidence is not high for several of the non-pharmacologic therapies, most have little or no adverse effects.26,27
Therefore, non-pharmacologic treatment for EIB is an area with many questions for continued research.18,19 In fact, to our knowledge, no study has evaluated the obesity-related inflammatory biomarkers and their influence on EIB in obese adolescents. Thus, considering the relevance of EIB in obesity and the importance of clinical strategies, in this study we have explored the EIB frequency and the associated risk factors in obese adolescents submitted to long-term interdisciplinary therapy.
QUICK LOOK
Current knowledge
Evidence suggests there is a greater prevalence of exercise-induced bronchospasm in obese adolescents. However, the role of pro-/anti-inflammatory adipokines and the repercussions of obesity treatment on exercise-induced bronchospasm are not well described.
What this paper contributes to our knowledge
A 1-year interdisciplinary weight loss therapy combining exercise training with medical, nutritional, and psychological therapies decreased exercise-induced bronchospasm frequency in obese adolescents, increased lung function, and improved pro-/anti-inflammatory adipokines.
Methods
Population
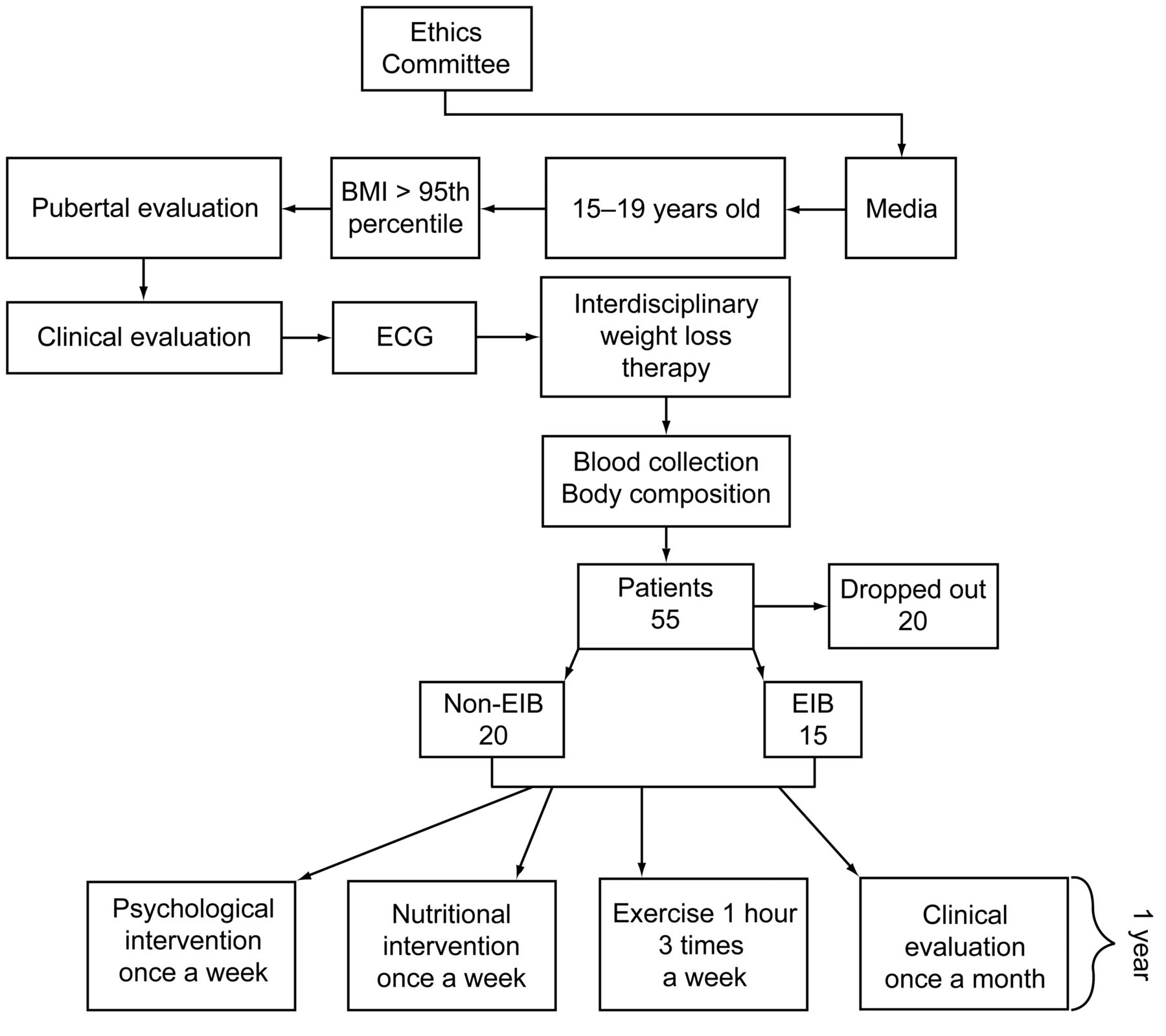
After a sample size power calculation, a total of 55 (15–19 years old) obese adolescents were enrolled to participate in the Interdisciplinary Obesity Program of the Universidade Federal de São Paulo Escola Paulista de Medicina (UNIFESP-EPM) (Fig. 1). The study occurred at the Sleep Institute in the Centro de Estudos em Psicobiologia e Exercício - Grupo de Estudos da Obesidade (CEPE-GEO) obesity interdisciplinary program, São Paulo, Brazil. The data were obtained in 2008 and 2009, when lung function was initially evaluated. The mean ± SD age was 16 ± 1.5 years. The mean ± SD body mass index (BMI) was 36 ± 5 kg/m2. All participants were confirmed as meeting the inclusion criteria of post-pubertal stage V (based on the Tanner stages)28 and of obesity (BMI > 95th percentile of the Centers for Disease Control reference growth charts).29 Non-inclusion criteria were as follows: metabolic, endocrine, or identified genetic diseases; viral diseases; previous drug use; cardiac or pulmonary diseases; and smoking.6

Study protocol diagram. BMI = body mass index. ECG = electrocardiogram. EIB = exercise-induced bronchospasm.
This study was performed in accordance with the principles of the Declaration of Helsinki, and was formally approved by the institutional ethics committee UNIFESP-EPM (0135/04). Informed consent was obtained from all subjects and/or their parents, and participation of the adolescents and their families was voluntary.
Study Protocol and Medical Screening
The subjects were medically screened, and their pubertal stage and anthropometric measures were evaluated. For all subjects, the procedures were scheduled for the same time of day, to remove any influence of diurnal variation. An endocrinologist recorded their health and clinical parameters monthly (see Fig. 1).
Anthropometric Measurements and Body Composition
The subjects were weighed while wearing light clothing and no shoes, on a Filizola scale, to the nearest 0.1 kg. Height was measured to the nearest 0.5 cm, with a wall-mounted stadiometer (Sanny ES 2030, American Medical do Brazil, São Bernardo do Campo, Brazil). BMI was calculated as body weight divided by height squared (wt/ht2).
Body composition was measured by plethysmography in a BOD POD body composition system (version 1.69, Life Measurement Instruments, Concord, California).30 Visceral and subcutaneous fat were assessed by ultrasonography, as previously described.31,32
Serum Analysis
Blood samples were collected at the out-patient clinic, around 8:00 am, after an overnight fast, by a skilled and qualified technician. After collection, the blood was centrifuged for 10 min at 5,000 revolutions/min and stored at −70°C. The materials used for collection were disposable, adequately labeled, and of recognized quality. Adiponectin (Phoenix Pharmaceuticals, Belmont, California) and leptin (Chemicon International, Millipore, Billerica, Massachusetts) levels were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits, according to the manufacturers' instructions.
Evaluation of Lung Function
Lung function was measured with a spirometer (EasyOne model 2001, ndd Medizintechnik, Zürich, Switzerland), according to American Thoracic Society criteria.33 The highest of 3 technically appropriate measurements was recorded. While the subjects were performing the maneuver, volume-time and flow-volume curves were followed on the screen. FVC (L), FEV1 (L), FEV1/FVC (%), and peak expiratory flow (L/s) were measured, and predicted values were obtained.34
The diagnosis of asthma was made according to American Thoracic Society guidelines.33 Specifically, the patients who presented a 6-month or longer history of recurrent chest symptoms, such as coughing, dyspnea, and wheezing, that were relieved by bronchodilator treatment, and whose spirometry demonstrated reversible air-flow limitation were not included in the study. The International Study of Asthma and Allergy in Childhood (ISAAC) questionnaire was used to assess asthma-related symptoms.35
Exercise Challenge Test
A standardized exercise challenge test consisted of 8 min on a treadmill, and was initiated at a speed of 1 km/h and a 0% inclination, increasing 1.5 km/h and a 2.5% inclination after each 30-second period for 2 minutes, until the subject achieved 6 km/h and a 10% level of inclination. The challenge was conducted by having subjects run for 8 min while inhaling air through their mouths, at a work load that increased the heart rate to 80% of the age-predicted maximum.36 During the days of testing, mean temperature and relative humidity were 25 ± 5°C and 41 ± 10%, respectively. The study was conducted in the afternoon (1:00–5:00 pm).
Spirometric measurements were made immediately before and at 2, 5, 10, 15, 20, 25, and 30 min after exercise. To measure EIB, the maximal change in FEV1 was calculated as:
EIB diagnosis was defined as a 15% or greater reduction in FEV1 after exercise, compared to FEV1 at baseline. As previously mentioned, the prior history of EIB was evaluated by the ISSAC questionnaire.37
Research Design
A 1-year interdisciplinary weight loss therapy combined exercise training with medical, nutritional, and psychological therapies. The use of an interdisciplinary approach as a criterion has been suggested by the World Health Organization.38 All measurements were performed at baseline and after 6 months (short-term) and 1 year (long-term) of therapy.
Psychological Therapy
During 1 year of interdisciplinary therapy, the adolescents received psychological orientation for one hour in a weekly group session. A psychologist discussed body image and eating disorders, as well as binge eating disorders, and their signs, symptoms, and health consequences. The psychologist also discussed the relationship between emotions and food, as well as familial problems, in a group setting. Individualized psychological therapy was recommended when behavioral alterations were found, including depression, anxiety symptoms, or poor dietary habits such as bulimia, anorexia nervosa, and binge eating.39
Nutritional Therapy
Once a week for 1 year, the adolescents had nutritional lessons regarding topics such as the food pyramid, food record, weight loss diets, diet and light concepts, fat and cholesterol, and eating disorders. Energy intake was set at the levels recommended by the dietary reference for subjects with low levels of physical activity of the same age and sex.40 A 3-day dietary record was made for each adolescent to help his/her parents. Portions were measured in terms of familiar volumes and sizes. The nutritionist explained to the parents and the adolescents how to record food consumption. These dietary data were transferred to a computer by the same nutritionist, allowing for nutrient composition analysis by a software program developed at UNIFESP-EPM (Nutwin for Windows, version 1.5) based on Western and local food tables.
Physical Therapy
An aerobic and resistance training regimen was performed 3 times a week for 1 year. Each session included 30 min of aerobic training plus 30 min of resistance training. The volunteers were instructed to invert the order of the exercises at each training session; in one session, the adolescent started the training session with aerobic exercises, and in the subsequent session, the same adolescent started with resistance training. Aerobic training consisted of running on a motor-driven treadmill (model TR 9700HR, Life Fitness, Schiller Park, Illinois) at the cardiac frequency intensity of ventilatory threshold I (± 4 beats/min), which was determined by the results of an initial oxygen uptake test for aerobic exercise (cycle-ergometer and treadmill). In addition, the maximal O2 consumption (V̇O2max) values were obtained from the oxygen uptake tests.
The physiologists controlled the cardiac frequency, which was measured with a cardiometer at 5 min intervals during all training sessions (FS1, Polar Electro, Kempele, Finland). The exercise program was based on the American College of Sports Medicine recommendations.41 We used exercises for the main muscle groups (bench press, leg press, sit-ups, lat pull-down, hamstring curls, lower back, military press, calf raises, arm curls, and triceps pushdown), and the order of the exercises was strictly followed by the group.
The first 2 weeks of resistance training were for adaptation to training and learning other movements (3 sets of 15–20 maximal repetitions). Following this adaptation period, the training load was adjusted by increasing the weight and intensity, and by decreasing the number of repetitions to between 6–20 for each of the 3 sets. The following rest intervals were allowed between series and exercises: 15–20 maximal repetitions = 45 seconds, 10–12 maximal repetitions = 1 min, and 6–8 maximal repetitions = 1.5 min. The training loads were adjusted in each training session and evaluated according to the increase in the strength of the participants. Therefore, training was conducted with maximal repetitions. During exercise therapy, the EIB subjects were accompanied by a physical therapist who controlled their symptoms.
Statistical Analysis
Statistical analyses were performed using software (Statistica, version 7.0 for Windows, StatSoft, Tulsa, Oklahoma), and a sample size calculation was performed with alpha equal to .05. The Gaussian distribution of variables was verified with the Shapiro-Wilk W test, and variables with normal distribution were expressed as the mean ± SD, whereas variables without normal distribution were expressed as median (minimum and maximum) in a descriptive table. The variables that did not present a normal distribution were leptin and adiponectin concentrations and the adiponectin/leptin ratio; for these variables, non-parametric methods were used.
The comparisons between the measurements of the parametric variables before intervention and 6 months and 1 year after intervention were determined by repeated measures analysis of variance. The Wilcoxon signed-rank test and Mann-Whitney U test were used to analyze the non-parametric variables.
Logistic regression analysis was used to ascertain the risk factors to EIB occurrence at baseline. The analysis was performed with all the subjects. The EIB diagnosis was set as a dependent variable in different models. First, the data were evaluated with a simple regression of the independent variables (body mass, V̇O2max, FEV1, adiponectin levels, leptin levels, or adiponectin/leptin ratio), whereas the EIB diagnosis was the dependent variable. Then a multiple regression was performed, considering the same variables as independent and the EIB diagnosis as dependent, but this analysis was adjusted for age and sex.
Furthermore, a simple linear regression was used, considering FEV1 as the dependent variable and leptin levels or BMI as independent variables to investigate if the FEV1 values had underlying associations with leptin levels and BMI values at baseline.
We assessed the correlation between delta values of EIB associated risk factors and lung function (Δ = the difference of values between 6 months or 1 year and baseline). The Pearson correlation coefficients were calculated to assess possible relationships between normally distributed variables, and Spearman correlation coefficients were used for non-parametric variables.
In addition, the Grubb test was used to detect outliers in the data, using software (GraphPad Prism, version 5.0 for Windows, GraphPad, San Diego, California). The results were considered statistically significant at the level of P < .05.
Results
At the beginning of the therapy, 55 obese adolescents were enrolled in the program. However, 35 subjects completed 1 year of therapy with more than 75% of treatment sessions. It is important to note that there were no differences for all variables between those who completed the therapy and the last known data from those who did not. The main reasons for dropping out in our study were financial and family problems, followed by school and job opportunities (see Fig. 1).
At baseline we did not find significant differences in age and BMI between the groups, after the studied population was paired by these variables according to sex. Furthermore, there were no statistically significant differences between sexes in both groups for all variables (data not shown).
One of the most important findings of the present study was that a reduction in EIB prevalence from 43% (no. = 15) to 13% (no. = 2) and 0% was shown, respectively, for short- and long-term therapy in all analyzed obese subjects.
According to EIB diagnosis at baseline, the volunteers were divided into 2 groups: non-EIB group (no. = 20) and EIB group (no. = 15) (Table 1). When the groups were compared, statistical differences between analyzed variables in all the times of evaluation were not observed. In both groups a significant reduction in all anthropometric variables was observed.
Anthropometric Variables, Body Composition, Visceral and Subcutaneous Fat, and Lung Function Variables Measured at Baseline and After Interdisciplinary Therapy in Obese Adolescents Classified by Diagnosis (n = 35)
Furthermore, after therapy, lung function improved (see Table 1) and was paralleled by a reduction in the percentage of fall in FEV1 and FEV1/FVC values after the exercise bronchoprovocation test in the EIB group (Fig. 2). Moreover, the volunteers of the EIB group did not present previous history of EIB evaluated by the ISAAC questionnaire, and did not receive medication to control symptoms of EIB (data not shown).
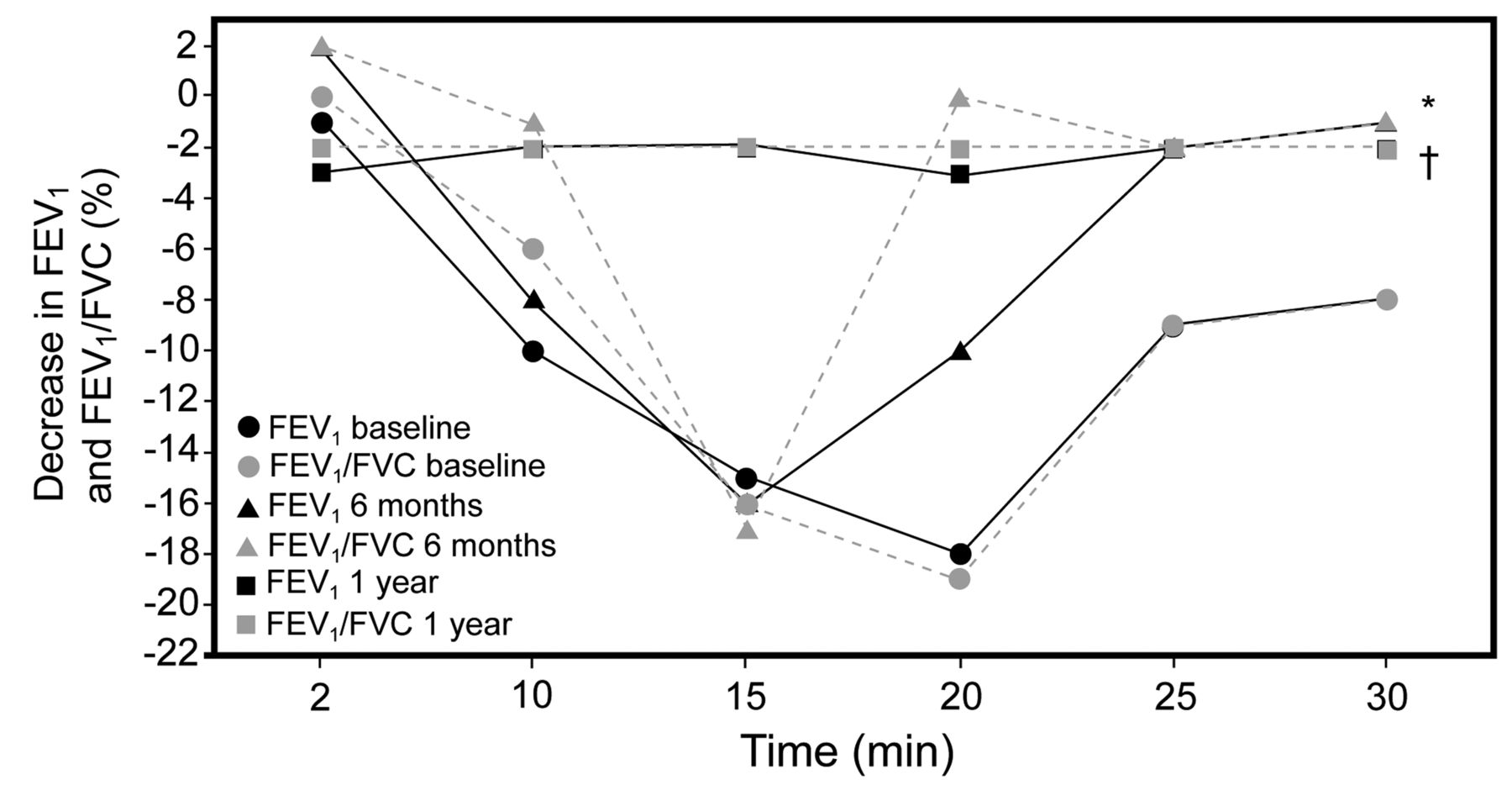
Percentage of decrease in FEV1 and FEV1/FVC values after bronchoprovocation test in the exercise-induced bronchospasm group. * P = .02 between baseline and short-term therapy. † P = .01 between baseline and long-term therapy.
Logistic regression analysis showed that low values of FEV1 were a risk factor associated with the EIB diagnosis at baseline. The adjustments for age and sex did not change this association substantially (Table 2). Furthermore, a simple linear regression was performed considering FEV1 as the dependent variable and leptin levels or BMI as independent variables to investigate if the lower FEV1 had underlying associations with leptin levels and BMI values at baseline; however, these variables were not predictors of FEV1 values (data not shown).
Logistic Regression Analysis of the Relationship Between EIB and Its Possible Associated Risk Factors at Baseline
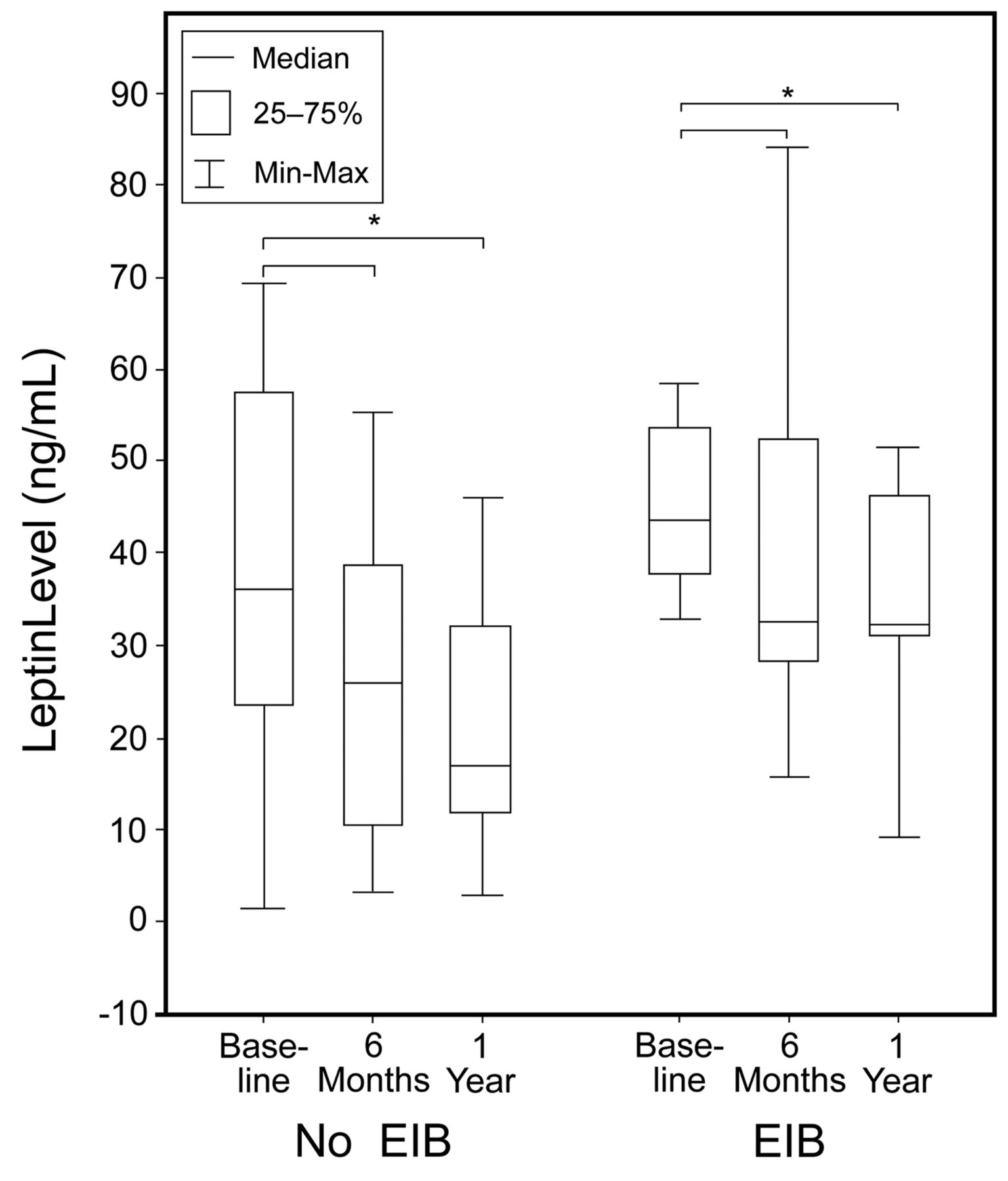
Another finding from the present investigation was that the adiponectin/leptin ratio (see Table 1) and the adiponectin concentration increased significantly (Fig. 3), while the leptin levels decreased significantly after therapy, in both groups (Fig. 4), although the state of hyperleptinemia was maintained in the EIB group.

The adiponectin levels measured at baseline and after 6 months and 1 year of interdisciplinary therapy in both groups. * Baseline versus 1 year of therapy P = < .05.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The leptin levels measured at baseline and after 6 months and 1 year of interdisciplinary therapy in both groups. * Baseline versus 1 year of therapy P = < .05.
Another important result was that changes in lung function were negatively correlated with changes in anthropometric variables and leptin levels in both groups. On the other hand, positive correlations were observed among changes in lung function and adiponectin levels and V̇O2max in both groups (Table 3). Nevertheless, the EIB group did not have a significant increase in V̇O2max (see Table 1).
Correlation Coefficients of the Factors Potentially Associated With EIB in Obese Adolescents at Short and Long Term After Therapy
Discussion
In the present study, interdisciplinary therapy promoted a great control of the EIB occurrence in all subjects, paralleled by an increase in lung function and improvement in pro-/anti-inflammatory adipokines profile. Furthermore, we observed that low FEV1 values were a risk factor associated with EIB diagnosis at baseline.
In this context, pharmacologic and non-pharmacologic methods can be used in the management of EIB.19 Proposed options for non-pharmacologic management include physical conditioning, nasal breathing, incorporating a warm-up before and a cool-down period after exercise, avoidance of cold weather or environmental allergens, and using a face mask or other aid to warm and humidify inhaled air.18,19 Recent results also suggests that dietary modifications may play a role in controlling EIB in asthmatics.25 However, to our knowledge, this is the first study that has evaluated the effect of an interdisciplinary therapy of 1 year on EIB frequency and possible mechanisms involved in this change, such as inflammatory factors (leptin, adiponectin and adiponectin/leptin ratio) in non-asthmatic obese adolescents.
Obesity negatively affects the respiratory and other systems in many ways, and previous studies have demonstrated that increased body weight has been associated with bronchial hyper-responsiveness in obese patients,42 confirming the importance of attenuating the inflammatory process related to obesity and respiratory conditions. Nevertheless, studies assessing EIB frequency in non-asthmatic obese children and adolescents have found conflicting results.6,7,10,11
In the present investigation, we observed that 1 year of interdisciplinary therapy decreased EIB frequency; this fact was evidenced by the proportional change in FEV1 and FEV1/FVC after exercise in the EIB group (see Fig. 2). This is a relevant finding, considering that some studies have demonstrated that non-asthmatic obese individuals have a greater EIB frequency, compared to lean individuals.6,7 Furthermore, this condition can be a restriction to the practice of physical exercise and consequently contributes to sedentarism,43 as well to a vicious cycle between causes and consequences linking obesity and respiratory diseases.44
The sedentary state of obese individuals further complicates matters by putting an added strain on the respiratory system: their decreased V̇O2max causes this system to work much harder for an equivalent level of physical activity, even at low levels.43 It should also be considered that the ventilatory reserves in the obese are limited by their ability to support the increased muscle oxygen requirements during exercise, because the lungs do not increase in size commensurate with the subject's added weight.45
In our study, differences in the V̇O2max values were not found between the groups. However, after therapy, the improvement in FEV1 was correlated with the change in V̇O2max. This result was expected because there was an improvement in lung function after therapy, and consequently in the ventilatory reserve, with an increase in V̇O2max values (Table 4).45 Furthermore, exercise programs involving aerobic activity have demonstrated a benefit in cardiorespiratory fitness, and consequently in the exercise tolerance and EIB frequency in asthmatics.26,27
The decrease in EIB frequency was followed by improvements in lung function (see Table 1), in agreement with previous studies.46,47 This increase in FEV1 and FEV1/FVC may reflect the enhancement in lung volumes, a well-known effect of weight loss in obese patients,46–48 suggesting an important role of an integrated clinical approach to control of chronic diseases.38
Moreover, one of the most important findings in this study was that a low FEV1 value was a risk factor associated with EIB at baseline, when adjusted for age and sex. There are some disagreements on the role of the pre-challenge FEV1 in the association between obesity and airway hyper-responsiveness. Whereas in some studies FEV1 remained unchanged or increased in obese individuals,49,50 others demonstrated that increased body fat or fat distribution impaired mechanical ventilation, with reduced ventilatory function and small tidal volumes, with low smooth airway stretch.50,51 Reduced smooth muscle stretch results in a “latch phase” with less actin-myosin cycling increasing airway hyper-responsiveness.13
In addition, the lung volume is a major determinant of the bronchoconstrictor response. Thus, changes in lung volume act to alter the forces of interdependence between airways and parenchyma that oppose airway smooth muscle contraction.52 Therefore, we suppose that this is the main mechanism for EIB occurrence in our study.
To better explore the other mechanisms involved in EIB occurrence in obese adolescents, a regression analysis was performed to investigate the role of leptin concentrations and adiposity measures on FEV1 values; however, these variables were not predictors of low FEV1 values at baseline (data not shown). This aspect needs to be investigated in future research with a larger cohort.
Moreover, after treatment, we showed that FEV1 values were negatively correlated with changes in leptin concentration. Nevertheless, after 1 year of therapy, the EIB group did not normalize the leptin values, remaining in a state of hyperleptinemia. Altogether, these findings suggest the difficulty in controlling both the neuroendocrine regulation of energy balance and the inflammatory process linking obesity and respiratory alterations.
Since its discovery, leptin has been known to play an important role in energy balance control.53 In addition, studies have observed an important function: up-regulation of inflammatory immune responses. This finding may provide a common pathogenesis mechanism, which contributes to the majority of complications of obesity.54 Leptin's action on inflammation leads to an inflammatory state in obese subjects.55
A previous study demonstrated that leptin was negatively correlated with lung function variables.14 Furthermore, leptin infusion in mice was associated with airway hyper-responsiveness.13 Human studies have demonstrated that high leptin concentration was associated with increased prevalence of asthma and a trend for wheezing in asthmatics.56,57 A recent study showed that the pro-inflammatory effects of obesity on the airway are probably not due to a direct effect of leptin on airway smooth muscle. In this sense, another mechanism proposed is that the leptin effects are a result of proliferation inhibition on human airway smooth muscle.14 Therefore, the main effects of leptin in this process are on airway inflammation and lung development.13,14,56,57
The reports are scarcer on the link between obesity-associated EIB and adiponectin, which is an obesity-related biomarker. Studies associating adipokines and asthma have documented a protective effect of high adiponectin concentration, although only in asthmatics patients.15,58
Thus, one finding from this study is that the improvement in FEV1values was positively correlated with changes in adiponectin concentration in non-asthmatic obese adolescents. The primary metabolic effects of adiponectin are on glucose regulation and fatty acid metabolism, but it also has an anti-inflammatory effect.59,60 Thus, the decreased adiponectin concentrations commonly observed in the obese, including adolescents, could contribute to the development of airway hyper-responsiveness.17 The significant increment in adiponectin and in adiponectin/leptin ratio after treatment can suggest a better control of subclinical inflammation related to obesity in these patients.
Taken together, this study demonstrated that interdisciplinary therapy promoted an improvement in lung function and anti-inflammatory profile, as well as a reduction in adiposity measures; however, the EIB group remained with higher leptin levels and did not improve their V̇O2max values. These findings reinforce the importance of the practice of non-pharmacologic therapy for the treatment of the common conditions related to obesity and respiratory alterations in non-asthmatic obese adolescents.
The lack of a control group represents a limitation of the present study. However, it should be mentioned that the original objective was to assess the effects of long-term interdisciplinary therapy on EIB frequency and inflammatory risk factors associated in obese adolescents. Further investigation including a control group and long-term follow-up are needed.
Conclusions
This study demonstrated a decrease in EIB frequency, paralleled by an increase in lung function and an improvement in the pro-/anti-inflammatory profile among obese adolescents. Additionally, this kind of treatment effectively ameliorates the hormonal profile and obesity in adolescents.
Footnotes
- Correspondence: Patrícia Leão da Silva MSc, Postgraduate Program of Nutrition, Universidade Federal de São Paulo, São Paulo, Brazil, Rua Marselhesa, 535 Vila Clementino, São Paulo, Brazil 04020–060. E-mail: patricialeao{at}cepebr.org.
This research was partly supported by Associação Fundo de Incentivo à Pesquisa (AFIP), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP 2008/53069–0, FAPESP 2006/00684–3, FAPESP 98/14303–3), Centro de Excelência Esportiva (CENESP), Fundo de Auxilio ao Docente e ao Aluna (FADA), Centros de Pesquisa, Inovação e Difusão (CEPID) Sleep no. 98/14303–3 ST), and Universidade Federal de São Paulo, São Paulo, Brazil.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.