

Abstract
BACKGROUND: Heat and moisture exchangers (HMEs) are commonly used in chronically tracheostomized spontaneously breathing patients, to condition inhaled air, maintain lower airway function, and minimize the viscosity of secretions. Supplemental oxygen (O2) can be added to most HMEs designed for spontaneously breathing tracheostomized patients. We tested the efficiency of 7 HMEs designed for spontaneously breathing tracheostomized patients, in a normothermic model, at different minute ventilations (V̇E) and supplemental O2 flows.
METHODS: HME efficiency was evaluated using an in vitro lung model at 2 V̇E (5 and 15 L/min) and 4 supplemental O2 flows (0, 3, 6, and 12 L/min). Wet and dry temperatures of the inspiratory flow were measured, and absolute humidity was calculated. In addition, HME efficiency at 0, 12, and 24 h use was evaluated, as well as resistance to flow at 0 and 24 h.
RESULTS: The progressive increase in O2 flow from 0 to 12 L/min was associated with a reduction in temperature and absolute humidity. Under the same conditions, this effect was greater at lower V̇E. The HME with the best performance provided an absolute humidity of 26 mg H2O/L and a temperature of 27.8°C. No significant changes in efficiency or resistance were detected during the 24 h evaluation.
CONCLUSIONS: The efficiency of HMEs in terms of temperature and absolute humidity is significantly affected by O2 supplementation and V̇E.
- tracheostomized patients
- absolute humidity
- inspiratory air temperature
- air conditioning
- heat and moisture exchangers
Introduction
The main functions of the upper airways are warming, humidifying, and filtering the inspired gas. In patients with tracheostomies the upper airway is bypassed, thus losing conditioning and filtering function. Breathing non-conditioned air for a prolonged time may damage the mucociliary function, resulting in a decrease in secretion clearance.1,2 Moreover, breathing cold and dry air results in heat loss and water loss by evaporation.1,2 Several animal and human studies have attempted to determine the “optimal” temperature and absolute humidity of inspired air when the upper respiratory tract is bypassed by an endotracheal tube or a tracheostomy.3–6 Since 1992 the American Association for Respiratory Care (AARC) clinical practice guidelines7 have recommended that inspired gases be warmed to 30°C and humidified to 30–33 mg H2O/L. Heat and moisture exchangers (HMEs) conserve a portion of the heat and humidity from the exhaled gas, conditioning the subsequently inspired gas.8–10 The use of HMEs in chronically tracheostomized spontaneously breathing patients can reduce retained secretions and improve quality of life.11,12 HMEs can also provide supplemental oxygen (O2) flow through a direct connection to an O2 delivery system. However, a dry and cold gas flow directly on the HME's membrane might reduce the amount of water and heat retained and transferred by the HME. In addition, a loss of HME efficiency during mechanical ventilation has been reported at high minute ventilation (V̇E).13,14 Our hypothesis was that additional O2 flow and different V̇E will affect the efficiency of HMEs designed for tracheostomized spontaneously breathing patients.
The aims of this study were to evaluate the effects of O2 flow at 3, 6, and 12 L/min and V̇E of 5 and 15 L/min on the performance (temperature and absolute humidity) of 7 commercially available HMEs, and to test their efficiency change over a 24 h period.
QUICK LOOK
Current knowledge
Heat and moisture exchangers (HMEs) are commonly used in chronically tracheostomized spontaneously breathing patients. Supplemental oxygen (O2) can affect the HME's performance.
What this paper contributes to our knowledge
The efficiency of HMEs used for spontaneously breathing patients with tracheostomy was decreased by increased O2 flow and increased minute ventilation. O2 flow of > 3 L/min was associated with important decreases in HME performance.
Methods
Experimental Protocol and Hygrometry
The experimental lung model consisted of a piston pump that was connected to one end of a breathing circuit, to simulate a spontaneously breathing patient (Fig. 1). The expiratory gas flow was heated and humidified (DAR HC 2000 HWH, Mallinckrodt/Covidien, Mansfield, Massachusetts) to mimic normothermic conditions (34°C).13,15 The HME was connected to the opposite end of the circuit and to O2 flow. A breathing circuit with 4 unidirectional valves to separate inspiratory and expiratory flows was inserted between the HME and the lung model. Two temperature probes, one dry and one wet (coated with cotton soaked with sterile water), were placed at both the inspiratory and expiratory sides of the circuit. The dry probe measured the actual gas temperature, while the wet one measured the temperature as lowered by evaporation. Since the wet probe measured a temperature proportional to gas dryness, the absolute humidity of the inspired and expired gases can be calculated from the temperature difference between the probes, with a formula previously reported.16,17 Temperatures were measured electronically, displayed on a screen and printed on a chart recorder (436004 uR 1000, Yokogawa, Tokyo, Japan). This psychrometric method is commonly used by clinicians and researchers interested in valuation of humidity.15,16 The system was considered stabilized after 1 h of ventilation without HME. The expiratory gas was maintained saturated at a temperature of 34°C. Once the lung model was stabilized, the HMEs were tested in a random order. Temperature and humidity output of the lung model were checked before each measurement.

Test setup. HME = heat and moisture exchanger.
Evaluation of Effects of O2 Flow and V̇E
Each HME was tested at 2 different V̇E (5 and 15 L/min, tidal volume 500 mL, and breathing frequencies of 10 and 30 breaths/min) and 4 O2 flows (0, 3, 6, and 12 L/min). For each combination of V̇E and O2 flow, 15 min after stabilization, 3 consecutive temperature measurements were taken and averaged. Room temperature and relative humidity were measured before each experiment and maintained constant throughout the experiment. Each pair of probes was calibrated by measuring room temperature, and the differences were always < 0.3°C. This value was used to correct all the measurements. All HMEs were tested on 4 different study days (a different HME was used each day) for assessment of reproducibility.
Evaluation After 24 Hours of Use
Each HME was studied for 24 consecutive hours with a V̇E of 10 L/min. A V̇E of 10 L/min was chosen, because it was midway between the 2 V̇E tested short-term, and represents a typical V̇E in critically ill patients. Temperature measurements were recorded at 0, 6, 12, and 24 h; resistance and weight of the HME were recorded at 0 and 24 h. Flow resistance was estimated from the pressure drop across the HME at 60 L/min flow. HME weight was measured by a precision balance, and the absolute change for each HME was determined.
The following commercially available HMEs were tested: HCH-6V (Mediflux, Croissy Beaubourg, France), HCH-6F (Mediflux, Croissy Beaubourg, France), Hydro-Trach T (Intersurgical, Woingham, Berkshire, United Kingdom), Edith Trach (GE Healthcare, Madison, Wisconsin), Tracheolife II (Mallinckrodt/Covidien, Mansfield, Massachusetts), Tracheal HME 9500/01S (Air Safety Limited, Lancashire, United Kingdom), and HME-D6 (DEAS, Castel Bolognese, Italy). Their main characteristics, according to the manufacturers, are described in Table 1.
Characteristics of the Heat and Moisture Exchangers as Described by the Manufacturers
Statistical Analysis
Descriptive statistics are expressed as mean ± SD, median, minimum/maximum, 95% CI, and/or percentages. The coefficient of variation was calculated for the temperature and absolute humidity measurements. Normal distribution was evaluated with the Shapiro-Wilk normality test. Pearson correlation was performed to determine the degree of correlation between continuous variables. The values were compared as means of repeated measures by 2-way analysis of variance with the Tukey honest significant difference post hoc test. Homogeneity of variance was evaluated with the Fligner-Killeen test. Statistical significance was assumed by a 2-sided P value < .05. Statistical analysis was performed with statistics software (R 2.15.2, R Foundation, Vienna, Austria).
Results
Effects of O2 Flow and V̇E
Mean and median data for temperature and absolute humidity with each HME are presented, respectively, in Table 2 and Table 3. In all HMEs the progressive increase in O2 flow from 0 to 12 L/min was associated with a reduction in the temperature (P < .001) and absolute humidity (P < .001). Under the same conditions, this effect was greater at lower V̇E (5 vs 15 L/min) (P < .001) (Fig. 2). Comparing the average performance of all HMEs across all experimental settings, the minimum performance was a temperature of 24.6°C and an absolute humidity of 18.2 mg/L at V̇E 5 L/min and O2 flow 12 L/min, while the best performance was a temperature of 26.6°C and an absolute humidity of 23.4 mg/L at V̇E 15 L/min and O2 flow 0 L/min.
Descriptive Statistics of Temperature for the Tested Heat and Moisture Exchangers
Descriptive Statistics of Absolute Humidity for the Tested Heat and Moisture Exchangers
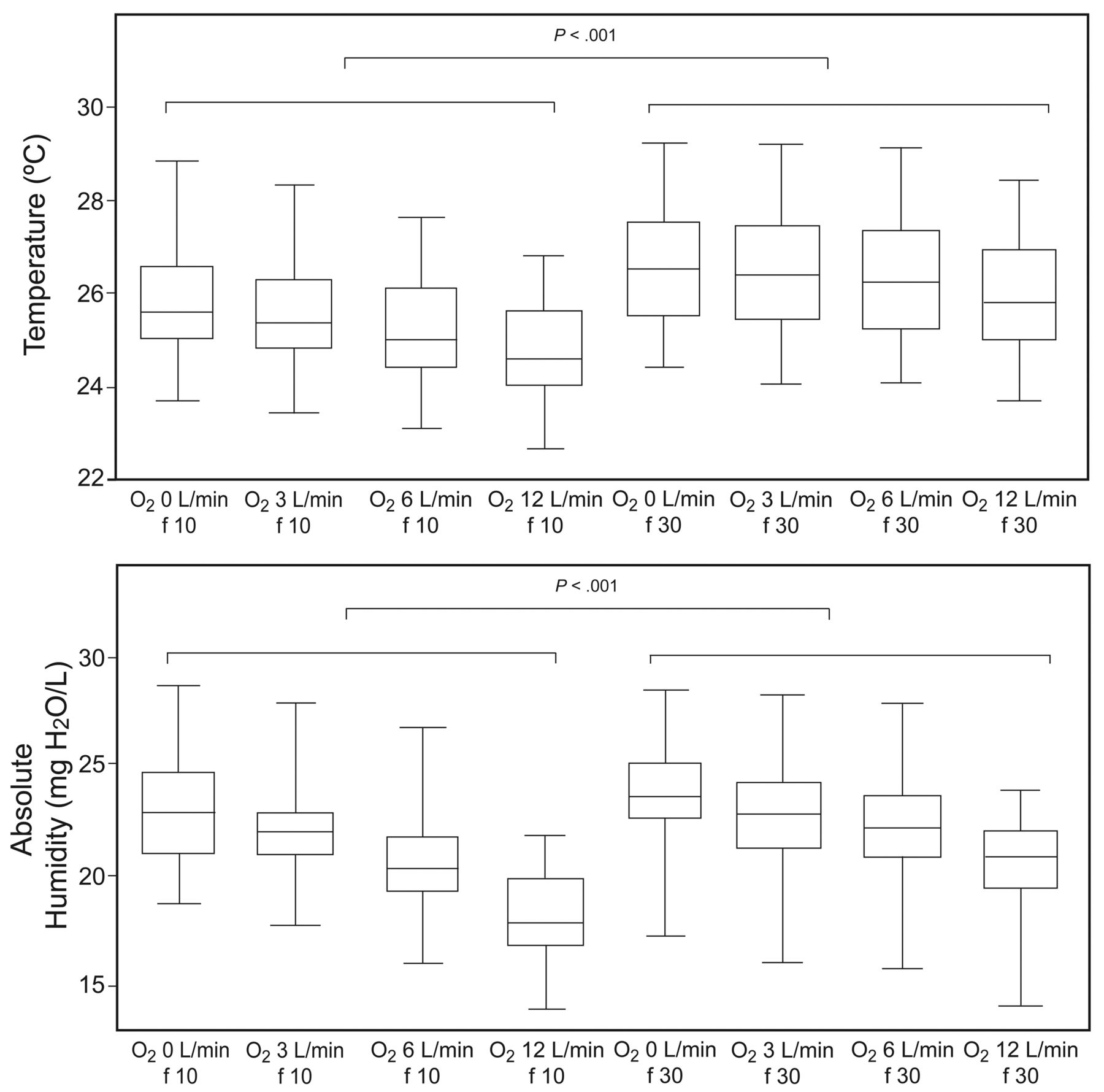
Temperature and absolute humidity versus O2 flow and breathing frequency (f). The horizontal lines within the data bars represent the medians. The tops and bottoms of the data bars represent the interquartile ranges. The whisker bars represent the minimum and maximum values.
Effects of Different HMEs on Temperature and Absolute Humidity
All the HMEs showed a variable degree of O2 flow-dependence, with increasing differences between measured and expected performance in terms of temperature and absolute humidity as O2 flow increased and V̇E decreased (P < .001). The overall performance of all HMEs tested is presented in Table 4 and 5 and Figure 3. The Tracheolife II showed the best performance: absolute humidity 26 mg H2O/L and temperature 27.8°C.
Temperature Comparisons
Absolute Humidity Comparisons

Median temperature and absolute humidity with the tested heat and moisture exchangers (HMEs). The horizontal lines within the data bars represent the medians. The tops and bottoms of the data bars represent the interquartile ranges. The whisker bars represent the minimum and maximum values.
Effects of 24 Hours of Use on Performance, Air Flow Resistance, and Weight
No significant drop in absolute humidity was detected over the 24 h evaluation of any HME (P = .99). No changes in flow resistance or pressure drop were observed between baseline and 24 h for any HME, except for Tracheolife II, which showed a pressure drop at 60 L/min, from 0.2 cm H2O to 0.8 cm H2O, which was not statistically significant or clinically important. The increases in weight at 24 h were 1.46 g for HCH-6V, 0.39 g for HCH-6F, 0.22 g for Hydro-Trach T, 2.05 g for Edith Trach, 0.47 g for Tracheolife II, 0.37 g for Tracheal HME 9500/01S, and 0.47 g for HME-D6, without any significant correlation with flow resistance at 60 L/min (r2 = 0.33, P = .46).
Between the 4 study days, room temperature was 24°C ± 0.5, whereas relative humidity was 13% ± 11. The dynamics of daily room temperature and relative humidity did not significantly affect the results (P = .58).
Discussion
The main results of the present study are:
The addition of O2 to an HME inversely affected HME efficiency.
The efficiency of all the HMEs was better at higher V̇E.
The Tracheolife II was best able to maintain temperature and absolute humidity of inspired gases.
To the best of our knowledge this is the first study evaluating the effects of the addition of O2, various V̇E, and 24 h use on the efficiency of HMEs for tracheostomized spontaneously breathing patients. It is important to stress that none of the HMEs tested met the AARC clinical practice guideline standards for humidification: 30–33 mg/L and 30°C.7
Effect of O2 Flow and V̇E
The absolute humidity and temperature of inspired gases were significantly, inversely affected by the addition of O2 flow. The drop in efficiency from 0 to 12 L/min of O2 flow was higher for absolute humidity than for temperature, and these results were consistent for all HMEs. We found that Tracheolife II maintained an acceptable performance up to 6 L/min O2 flow, then demonstrated a fall at 12 L/min, while the other HMEs presented a more gradual reduction in efficiency as O2 flow increased.
Most HMEs commercially available have the capability of adding supplemental O2 flow to increase FIO2. However, to our knowledge there is no information in the manufacturers' literature discussing the effect of adding O2 on the efficiency of the HME. The decrease in efficiency of HMEs at increasing O2 flow should be considered by physicians trying to optimize the clinical condition of their patients. The interdependence of HME performance and supplemental O2 flow should be expected, since HMEs are characterized by a hygroscopic membrane that retains water and heat from the exhaled air and then returns it to inspired air. The addition of supplemental O2 dries and lowers the temperature of the hygroscopic material, thus negatively affecting HME performance. The method of O2 delivery may be one of the reasons for the different behavior of each HME to increasing O2 flows, since some HMEs allow O2 to travel to the patient without traversing the hygroscopic membrane, while others direct the added O2 flow through the hygroscopic membrane.
In general, considering all HMEs tested at the 2 different V̇E conditions, they provided better temperature and humidity output at higher V̇E. Previous studies, reported contradictory results on the effects of V̇E on HME performance during mechanical ventilation.13–15 In fact, Unal et al14 found better performance at lower V̇E, while Pelosi et al15 demonstrated better performance at higher V̇E, and Chiumello et al13 found the best performance at 10 L/min, with a decrease in performance both at higher and lower V̇E. However, contrary to our study, those authors did not test HMEs designed for tracheostomized patients during spontaneous breathing. Our results can be explained by the fact that at lower V̇E the hygroscopic membrane receives less conditioned exhaled air per minute, allowing more time to cool down, thus losing more water molecules and being less efficient in the subsequent inspiration. Moreover, the HMEs were tested at 2 different V̇E (5 vs 15 L/min) by modifying only the respiratory frequency (10 vs 30 breaths/min). The differences in efficiency may be a direct result of the fact that with a higher respiratory frequency there is less time for the hygroscopic membrane to cool down. This finding may be minimized by increasing tidal volume to increase V̇E instead of rate.
Effect of Different HMEs on Temperature and Absolute Humidity
The present study has shown significant differences in efficiency among the 7 HMEs evaluated. Comparing the temperature output and absolute humidity of the HMEs at 15 L/min V̇E and 0 L/min O2 flow, the best performance was by Tracheolife II, with 28.4 mg H2O/L and 29.2°C, respectively, while the worst performance was by HME-D6, with 18.4 mg H2O/L and 25.3°C, respectively. The optimal level of inspired air conditioning in tracheostomized patients is still debatable. To the best of our knowledge there are no specific guidelines on the levels of absolute humidity and temperature in spontaneously breathing tracheostomized patients. Some studies on tracheostomized dogs have defined the optimal range of humidity to be 100% saturation at 25–30°C (ie, absolute humidity 23.1–30.5 mg H2O/L).18,19 In addition, excessive heating and humidification are recognized as harmful to the airway mucosa.20–22 In normal conditions the temperature range of expired gases is 28–32°C, with an absolute humidity of 27–33 mg H2O/L, and thus an inspired-gas temperature range of 29–33°C and an absolute humidity of 28–35 mg H2O/L should be adequate.23 These guidelines7 might also apply to tracheostomized patients, even if the portion of the artificial airway above the carina is shorter than with an endotracheal tube. We found that only the Tracheolife II reached the levels recommended in all conditions except for low V̇E with 6 or 12 L/min O2 flow and high V̇E with 12 L/min. The structure of Tracheolife II is very different from that of the other HMEs. Tracheolife II does not contain a spongy material like the others, but instead has an embossed and pleated membrane, which allows substantially more hygroscopic surface and consequently a greater entrapment of water.
We found that the performance of HMEs designed for tracheostomized patients during spontaneous breathing was poorer than that reported for HMEs for mechanically ventilated patients under similar experimental conditions.13,15,24 HMEs for spontaneously breathing patients are inserted into an open breathing circuit, drawing air from the room, whereas HMEs for mechanically ventilated patients are used in a closed ventilatory circuit, so the heat and moisture are kept within the system. Furthermore, HMEs for spontaneously breathing patients, except for Tracheolife II, are hollow in the middle, and the membrane is displaced to the periphery, allowing the collection of secretions and minimizing the increase of airway resistance, while all HMEs for mechanically ventilated patients have the membrane throughout the device, promoting efficiency but increasing resistance.
Effects of 24 Hours of Use on Performance, Air Flow Resistance, and Weight
Absolute humidity and temperature output were not affected during the 24 h study period. Several investigations of HMEs for mechanical ventilation demonstrated that changing HMEs after 48 h25–27 or even 96 h28 did not influence efficiency nor the incidence of nosocomial pneumonia. HMEs for spontaneously breathing patients have not been tested for longer than 24 h use, and are marketed with directions to replace them every 24 h. They do not have an antibacterial filter and are hollow in the middle, avoiding an increase of airway resistance. Our in vitro data suggest that HMEs could be used for longer periods, but the safety of this procedure should be demonstrated in a large clinical trial.
The efficiency of the HMEs evaluated was independent of room temperature and relative humidity, at least within the conditions during the present study. Room temperatures were similar throughout the 4 study days (24 ± 0.5°C); however, room relative humidity was quite different, depending on outside temperature (13 ± 11%). Room dryness may play an important role in absolute humidity output at different V̇E.
Our study has some limitations that need to be addressed. First, the model we used only partially reproduced clinical conditions. Thus, our results cannot be directly extrapolated to the clinical scenario. However, since all the devices were evaluated under the same conditions, the comparative efficiency of the devices is accurate. Second, all of the HMEs commercially available worldwide were not evaluated. Thus, other devices may demonstrate different performances. Third, the performance at different O2 flows and V̇E was not evaluated during the entire 24-hour period. Fourth, V̇E variations were only obtained by changing breathing frequency. Differences in performance between lower and higher V̇E may be a direct result of altering breathing frequency.
Conclusions
The performance of different commercially available HMEs used in tracheostomized patients during spontaneous breathing is significantly affected by O2 flow and V̇E. The minimal O2 flow required according to the patient's clinical condition should always be administered. Especially if a tracheostomized patient needs O2 flows higher than 3 L/min, the clinician should be aware of the negative effect O2 flow has on HME performance. Most importantly, the performance differences among the evaluated devices should be considered when making the choice of HME in tracheostomized spontaneous breathing patients. Finally, none of the HMEs tested met the AARC clinical practice guideline standards for humidification: 30–33 mg/L and 30°C.7
Footnotes
- Correspondence: Claudia Brusasco MD, Dipartimento di Scienze Chirurgiche e Diagnostiche Integrate, Università Degli Studi di Genova, Largo Rosanna Benzi 8, 16132, Genova, Italy. E-mail: claudia.brusasco{at}gmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}