

Abstract
BACKGROUND: Although leak compensation has been widely introduced to acute care ventilators to improve patient-ventilator synchronization in the presence of system leaks, there are no data on these ventilators' ability to prevent triggering and cycling asynchrony. The goal of this study was to evaluate the ability of leak compensation in acute care ventilators during invasive and noninvasive ventilation (NIV).
METHODS: Using a lung simulator, the impact of system leaks was compared on 7 ICU ventilators and 1 dedicated NIV ventilator during triggering and cycling at 2 respiratory mechanics (COPD and ARDS models) settings, various modes of ventilation (NIV mode [pressure support ventilation], and invasive mode [pressure support and continuous mandatory ventilation]), and 2 PEEP levels (5 and 10 cm H2O). Leak levels used were up to 35–36 L/min in NIV mode and 26–27 L/min in invasive mode.
RESULTS: Although all of the ventilators were able to synchronize with the simulator at baseline, only 4 of the 8 ventilators synchronized to all leaks in NIV mode, and 2 of the 8 ventilators in invasive mode. The number of breaths to synchronization was higher during increasing than during decreasing leak. In the COPD model, miss-triggering occurred more frequently and required a longer time to stabilize tidal volume than in the ARDS model. The PB840 required fewer breaths to synchronize in both invasive and noninvasive modes, compared with the other ventilators (P < .001).
CONCLUSIONS: Leak compensation in invasive and noninvasive modes has wide variations between ventilators. The PB840 and the V60 were the only ventilators to acclimate to all leaks, but there were differences in performance between these 2 ventilators. It is not clear if these differences have clinical importance.
Introduction
During mechanical ventilation, system leak is a major cause of patient-ventilator asynchrony.1 Leaks may be due to the endotracheal tube cuff, ventilator circuit, or chest drain during invasive ventilation. The incidence of endotracheal tube cuff leaks has been reported at ranges from 11% to 24%.2,3 With noninvasive ventilation (NIV), leaks around the face or nasal mask are a common cause of system leak.1 Patient-ventilator asynchronies have been reported to occur with a high incidence during both invasive4,5 and NIV.6,7 Thille et al reported that 24% of patients showed patient-ventilator asynchrony in > 10% of their total ventilatory rate during invasive ventilation.5 Vignaux et al demonstrated that auto-triggering was present in 13% of patients, and delayed cycling in 23% of patients during NIV.6 Patient-ventilator asynchrony can significantly increase the work of breathing,8,9 and a high incidence of patient-ventilator asynchrony is associated with a longer duration of mechanical ventilation.4,5
Although ICU ventilators were initially built to function without leaks, leak compensation has been added to ICU ventilators to improve patient-ventilator synchronization in the presence of system leaks. Ideally, leak compensation should automatically adjust during triggering and cycling to ensure that the ventilator rapidly responds to changes in leak without affecting patient-ventilator synchrony and maintains pressurization capacities. Ferreira et al evaluated the ability of 9 critical-care ventilators to function in the presence of leaks.10 The BiPAP Vision and the Servo-i were the only ventilators able to adapt to the leaks. Carteaux et al reported that dedicated NIV ventilators promoted better patient-ventilator synchronization than critical care and transport ventilators, even when the NIV mode was used.11
Technological improvements by ventilator companies are introduced rapidly. Currently there is no assessment of the performance of many ICU ventilators or the recent upgrades of ICU ventilators on their ability to prevent triggering and cycling asynchrony in both NIV and invasive ventilation. The aim of our study was to evaluate the ability of current acute care ventilators to prevent triggering and cycling asynchrony caused by increasing and decreasing leaks during both NIV and invasive ventilation.
QUICK LOOK
Current knowledge
During noninvasive ventilation leaks can cause auto-triggering and inappropriate cycling of breaths. Different ventilators demonstrate significant differences in their ability to compensate for leaks and achieve patient-synchrony.
What this paper contributes to our knowledge
Leak compensation in invasive and noninvasive modes demonstrated wide variations between ventilators, with regard to the ventilators' ability to reestablish synchrony. Ventilator performance, ventilator settings, and leak size all play an important role in determining appropriate triggering and cycling of breaths.
Methods
Seven ICU ventilators (Maquet Servo-i, Covidien PB840, Hamilton C3, Hamilton G5, GE Healthcare CareStation, Dräger V500, and CareFusion Avea) and one dedicated NIV ventilator (Respironics V60) (Table 1) were compared using a lung simulator (ASL5000, IngMar Medical, Pittsburgh, Pennsylvania)12 during increasing and decreasing system leaks.
Ventilator Specifications
Lung Model and Manikin Setup
The simulator was adjusted to simulate COPD and ARDS. In the COPD model, compliance was 60 mL/cm H2O, inspiratory resistance was 10 cm H2O/L/s, and expiratory resistance was 20 cm H2O/L/s. In the ARDS model, compliance was 20 mL/cm H2O and inspiratory and expiratory resistance were 5 cm H2O/L/s. The inspiratory time of the simulator was 0.92 s, the maximum inspiratory pressure drop was −5 cm H2O, the pressure drop generated 0.1 s after the onset of an occluded inspiratory effort was −3.6 cm H2O, and the breathing frequency was 15 breaths/min. For the profile of the negative pressure created by the respiratory muscles, 5% of the respiratory cycle time was active inspiration, 3% was an end-inspiratory hold, and 15% was for return of pressure to baseline. The ASL5000 incorporates a series of 3 user-controlled leaks with a simulator bypass and leak valve module.12
In the NIV mode, a manikin head was used to simulate the patient-mask interface (see the supplementary materials at http://www.rcjournal.com). An oronasal face mask (PerformaTrack SE, Respironics, Murrysville, Pennsylvania) was affixed to the head of the manikin with standard straps. A baseline leak of 3–4 L/min (baseline leak: B) at a mean airway pressure of 7.5 cm H2O was established. The simulator bypass and leak valve module was set to leaks of 9–10 L/min (leak level 1: L1), 26–27 L/min (L2), and 35–36 L/min (L3) at a mean airway pressure of 7.5 cm H2O. We chose these levels to represent the range of leak flows that are likely to be experienced clinically.13 All combinations of increasing (n = 6) and decreasing (n = 6) leaks were evaluated.
During invasive ventilation, the ventilators were affixed to the lung model with an 8 mm internal diameter endotracheal tube (see the supplementary materials at http://www.rcjournal.com). The simulator bypass and leak valve module was set to leaks of 3–4 L/min (L1), 9–10 L/min (L2), and 26–27 L/min (L3) at a mean airway pressure of 7.5 cm H2O. All combinations of increasing (n = 6) and decreasing (n = 6) leaks were evaluated.
Ventilator Setup
During the NIV assessment, all of the ventilators were set in NIV mode as follows: pressure support ventilation (PSV); inspiratory pressure 12 cm H2O; PEEP 5 or 10 cm H2O; breathing frequency 10 breaths/min; and leak compensation activated if available. Trigger sensitivity was set to 3 L/min if available. Inspiratory rise time, when adjustable, was set to the most rapid setting while avoiding overshooting of the set peak pressure. In the COPD model, the termination criteria, when adjustable, was set to ensure that the lung model's end of inspiration and the ventilator's end of inspiration did not differ by more than ± 5% at baseline leak. In the ARDS model the termination criteria were set at 25% of the peak flow. The maximum duration of inspiration was set to 1.5 s.
During invasive ventilation, all the ventilators were set in PSV and continuous mandatory ventilation (CMV): pressure level 12 cm H2O; PEEP 5 or 10 cm H2O; breathing frequency 10 breaths/min; and leak compensation activated if available. Trigger sensitivity and cycling criteria were set the same as during NIV. In CMV mode the inspiratory time was set at 0.90 s, approximately equal to the inspiratory time of the lung model (0.92 s).
Variables and Evaluation
For the evaluation of synchronization we recorded the number of breaths to synchronization after leak change (breaths to synchronization). The following variables were also recorded: auto-triggering, the number of cycles not triggered after a change in leak until synchronization; miss-triggering, the number of efforts not recognized by the ventilator prior to synchronization; time to settle, the number of breaths from the moment leak was increased or decreased until the tidal volume was within 2 standard deviations of the mean tidal volume for each leak level. In addition, the following variables were evaluated: time to baseline pressure, the time from the beginning of an inspiratory effort to the return of airway pressure to baseline during triggering; triggering pressure, the airway pressure change needed to trigger; delivered tidal volume, and cycling delay time, time from the end of inspiratory effort to the moment the ventilator cycled to expiration. Each specific evaluation scenario was repeated 3 times.
Data Collection and Analysis
After each change in leak level we waited up to 1 min for the ventilator to synchronize with the simulator. If synchronization was not achieved, the ventilator was considered unable to compensate at that specific leak setting, and data were not collected. If synchronization was achieved within 1 min, a total of 2 min of data after each change in leak level was collected and analyzed. Offline analysis of each breath was performed by the lung model's software (Labview, National Instruments, Austin, Texas). A P < .05 was considered significant. Data are presented as mean ± SD or median (IQR), depending on the parametric or non-parametric nature of the data distribution. Regarding the time to baseline pressure, triggering pressure, delayed cycling time, and delivered tidal volume, we report only differences that were both statistically significant (P < .05) and clinically important (> 10%).
Results
Synchronization
In NIV mode the Servo-i, PB840, C3, and V60 synchronized to all increasing and decreasing leaks in both the COPD model and the ARDS model (Tables 2 and 3). In invasive mode only the PB840 and the V60 synchronized to all increasing and decreasing leaks in both PSV and CMV.
Synchronization Capability Under Leak Scenarios During Noninvasive Ventilation Modes
Synchronization Capability Under Leak Scenarios During Invasive Ventilation Modes
Increasing Leak Versus Decreasing Leak
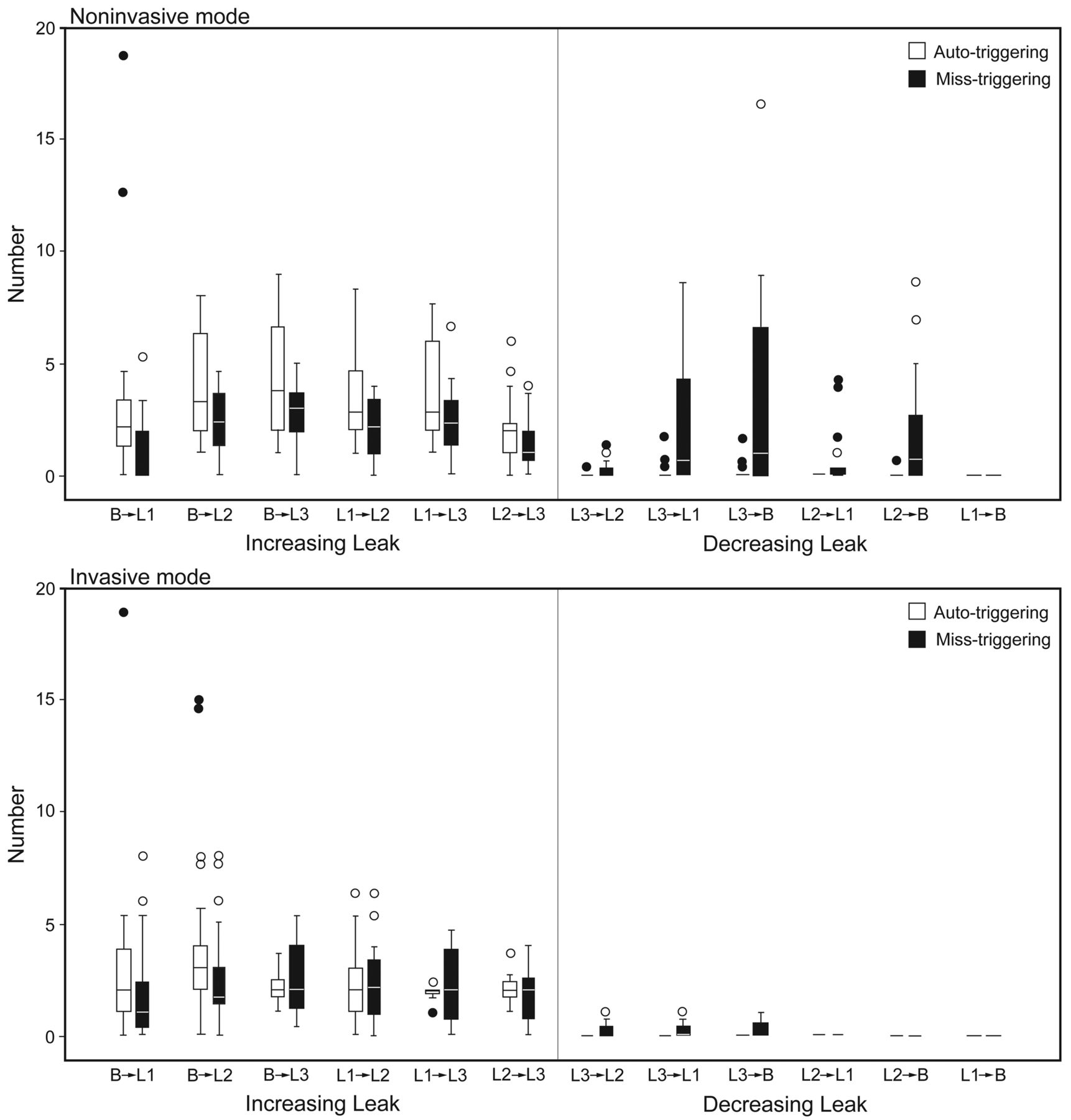
Breaths to synchronization, miss-triggering, auto-triggering and time to settle were higher for increasing than for decreasing leaks (Fig. 1, and see the supplementary materials at http://www.rcjournal.com). During increasing leak, auto-triggering occurred more frequently than miss-triggering, and during decreasing leak, miss-triggering occurred more frequently than auto-triggering, in both NIV and invasive ventilation (see Fig. 1). As the magnitude of the change in leak increased, breaths to synchronization and miss-triggering increased, but not auto-triggering (P < .001).

Auto-triggering and miss-triggering under increasing and decreasing leak during invasive and noninvasive ventilation. The B and L codes are explained in the text. In the data bars the horizontal lines represent the median values, the tops and bottoms of the bars represents the IQR, and the whisker bars represent the maximum and minimum values except for outliers. The circles represent outliers > 1.5 times the data-bar length. The dots represent outliers > 3.0 times the data-bar length. In noninvasive mode, for miss-triggering, P < .01 for B→L3 > B→L1, P < .01 for B→L3 > L2→L3, P < .001 for L3→L1 > L1→B, P < .001 for L3→B > L1→B, P < .01 for L2→B > L1→B, P = .002 for L3→B > L3→L2. There were no significant differences between the leak scenarios.
COPD Versus ARDS Model
In NIV mode, miss-triggering and time to settle were higher with the COPD model than with the ARDS model. Auto-triggering was higher in the ARDS model than in the COPD model (see the supplementary materials at http://www.rcjournal.com).
In invasive mode, miss-triggering (PSV) and time to settle (PSV and CMV) were higher in the COPD model than in the ARDS model. Auto-triggering was higher in the ARDS model than in the COPD model in both PSV and CMV (see the supplementary materials at http://www.rcjournal.com).
PEEP 5 Versus 10 cm H2O
Breaths to synchronization, miss-triggering, auto-triggering, and time to settle were higher with PEEP 10 than 5 cm H2O in both NIV and invasive ventilation (see the supplementary materials at http://www.rcjournal.com).
Comparison Among Ventilators
We compared synchronization only among ventilators that could synchronize to all leak scenarios. In NIV the PB840 significantly outperformed the other 3 ventilators (Servo-i, C3, and V60) in 3 categories (breaths to synchronization, miss-triggering, and time to settle) (see the supplementary materials at http://www.rcjournal.com).
In invasive mode, the PB840 significantly outperformed the V60 in breaths to synchronization, miss-triggering, and time to settle in both PSV and CMV (see the supplementary materials at http://www.rcjournal.com).
PSV Versus CMV
There were significant differences in breaths to synchronization, miss-triggering, and time to settle between PSV and CMV, with CMV outperforming PSV in all 3 categories (see the supplementary materials at http://www.rcjournal.com).
Triggering Delay
In NIV mode the time to baseline pressure was longer in the COPD model (148 ± 22 ms) than in the ARDS model (128 ± 26 ms) (P < .001) (Fig. 2). The time to baseline pressure was longer in the C3 and the V60 than in the Servo-i (P < .001). All ventilators except for the G5 showed a time to baseline pressure < 150 ms at baseline leak. However, the C3 and the V60 showed time to baseline pressures over 150 ms in L2 and L3 (see Fig. 2).
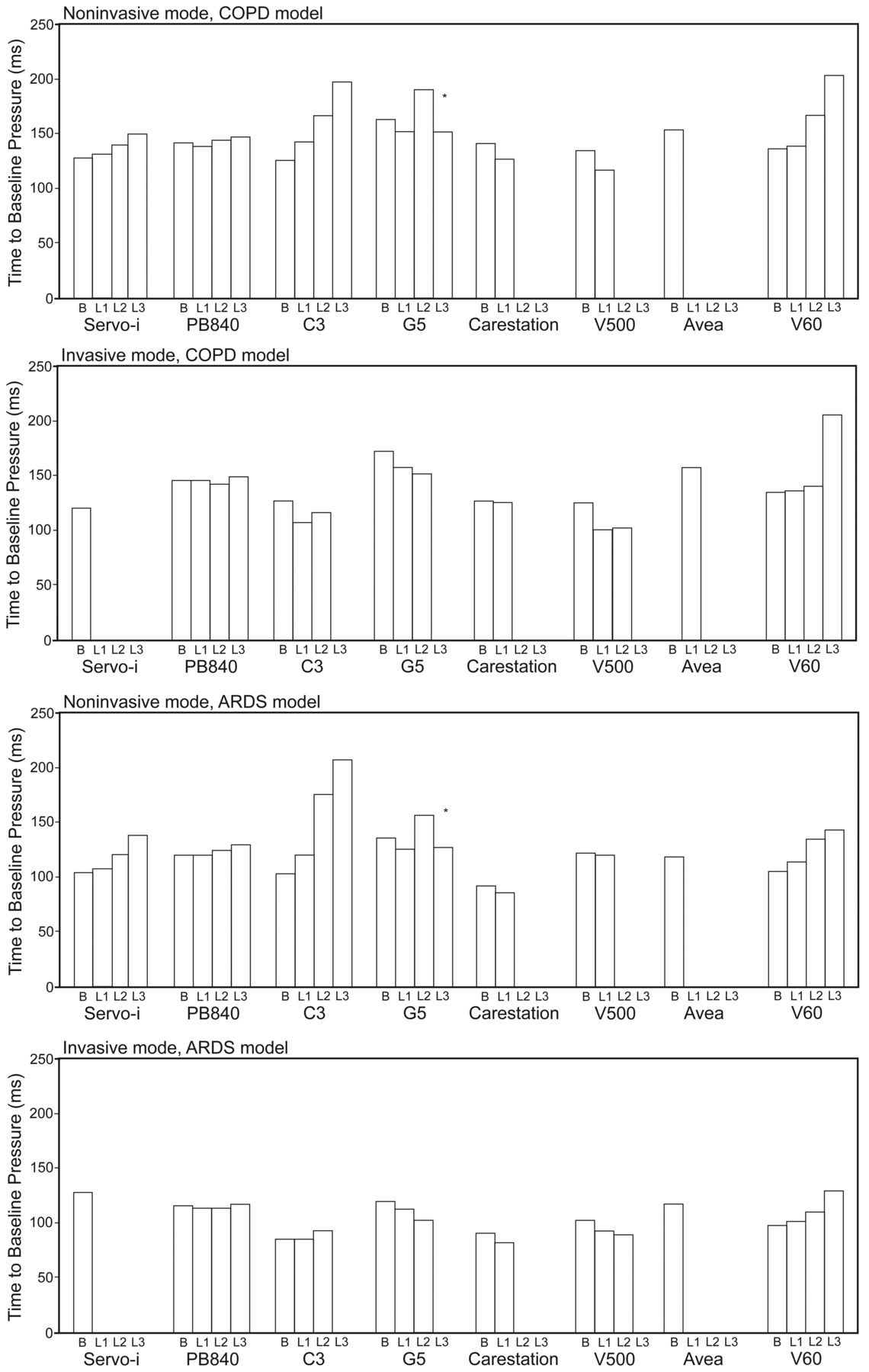
Mean time to baseline pressure under leak scenarios in COPD and ARDS models. The B and L codes are explained in the text. All data include the PEEP values 5 cm H2O and 10 cm H2O. Absence of a data bar indicates failure to synchronize during that leak scenario. * The data bars for the G5 ventilator show only PEEP of 5 cm H2O in conditions L2 and L3 because the G5 did not synchronize at PEEP of 10 cm H2O under conditions L2 and L3.
In invasive mode the time to baseline pressure was longer in the COPD model (139 ± 25 ms and 139 ± 23 ms) than in the ARDS model (112 ± 15 ms and 113 ± 15 ms) in both PSV and CMV (P < .001) (Fig. 3). There were no differences in mean triggering delay time between PSV and CMV in both the COPD model and the ARDS model (COPD model PSV vs CMV: 139 ms vs 139 ms, P = .89) (ARDS model PSV vs CMV: 112 ms vs 113 ms, P = .23). Comparing the PB840 and the V60, there was no significant difference between the 2 ventilators.

Mean cycling delay time under leak scenarios in COPD and ARDS models. The B and L codes are explained in the text. Positive values represent delayed cycling and negative values represent premature cycling. All data include the PEEP values 5 cm H2O and 10 cm H2O. Absence of a data bar indicates failure to synchronize during that leak scenario. * The data bars for the G5 ventilator show only PEEP of 5 cm H2O in conditions L2 and L3 because the G5 did not synchronize at PEEP of 10 cm H2O under conditions L2 and L3.
Cycling Delay
In NIV mode all the ventilators except for the G5 showed delayed cycling time within 50 ms in the COPD model. In the ARDS model all the ventilators except the C3 and the G5 showed a delivered inspiratory time > 100 ms shorter than the lung simulator inspiratory time in all leak scenarios (see Fig. 3). The C3 and the G5 showed prolonged cycling time in the ARDS model (> 2 times the lung simulator inspiratory time) during L2 and L3. In CMV all the ventilators showed a cycling delay time of approximately 50–100 ms in both the COPD and the ARDS models (see the supplementary materials at http://www.rcjournal.com).
Triggering Pressure and Tidal Volume
Triggering pressure and delivered tidal volume are described in the supplementary materials at http://www.rcjournal.com.
Discussion
The main findings of this study are as follows:
At baseline all the ventilators were able to synchronize without miss-triggering or auto-triggering, but there were wide variations in synchronization capability.
The ventilators performed better during decreasing than increasing leak.
The ventilators performed better with lower than with higher PEEP.
Miss-triggering occurred more frequently and longer times were required to stabilize tidal volumes in the COPD model than in the ARDS model.
Auto-triggering occurred more frequently in the ARDS model than in the COPD model.
The ventilators were better able to avoid miss-triggering and achieve synchronization and stabilization of tidal volume in CMV than in PSV.
The PB840 and the V60 were the only ventilators to maintain synchrony in all leak scenarios without adjustment of sensitivity or inspiratory termination criteria, but there were differences in performance between these 2 ventilators.
While previous studies have evaluated leak compensation in NIV alone,10,11 to the best of our knowledge this is the first assessment of leak compensation during invasive ventilation and NIV.
The ventilators performed better during decreasing than increasing leak scenarios. These findings were consistent with a previous report.14 As system leak increases, ventilators misinterpret the resulting changes in flow as inspiratory efforts, leading to frequent auto-triggering. If leak flow reaches the trigger threshold, auto-triggering occurs. Because of this, the frequency of auto-triggering does not depend on the magnitude of the increase in leak.6 On the other hand, if the leak is large enough, the ventilator may not detect respiratory efforts, leading to miss-triggering. Auto-triggering also may induce miss-triggering if inspiratory time is prolonged, due to auto-triggering overlapping the patient's next inspiratory effort. In other words, cycle asynchrony can produce trigger asynchrony. Thus, in order for a ventilator to maintain synchrony in the presence of leak, the ventilator has to automatically adjust the trigger sensitivity and/or cycling time.
The ventilators may automatically decrease trigger sensitivity according to the level of leak to avoid auto-triggering, but as the leak decreases the trigger sensitivity increases. This can lead to miss-triggering, particularly if the change is larger than the inspiratory effort. If the change in leak is smaller than the inspiratory effort, miss-triggering is unlikely, though higher patient effort is required to reach this threshold. Because all the ventilators measure one or several cycles and adjust trigger/cycling for the subsequent cycles following a leak level change, it is not possible to synchronize on the exact breath that the leak changes. Due to this technical constraint, leak compensation on current acute care ventilators is limited in its ability to provide synchrony.
The ventilators performed better at PEEP 5 cm H2O than at 10 cm H2O. Leak was created at the airway opening of the lung simulator, and the extent of the gas leak was nonlinearly related to pressure and flow. At higher PEEP the leak is increased due to the higher baseline pressure, and this may lead to an inability to distinguish the trigger signal from the leak.
In the COPD model miss-triggering was more frequent and required a longer time to stabilize tidal volumes than in the ARDS model. These results are consistent with those of previous reports.4,5 Compared to the ARDS model, the COPD model had increased time to baseline, triggering pressure, and delayed cycling time. This may be explained by the presence of higher airway resistance and lung compliance in the COPD model, which impede the transmission of respiratory effort to the ventilator and require larger efforts to reach the trigger threshold. On the other hand, auto-triggering was more frequent in the ARDS model than in the COPD model. Expiratory leaks can mimic an inspiratory effort, leading to auto-triggering. Premature cycling in the ARDS model prolongs expiratory time and may facilitate this expiratory leak effect. Another possible reason is that pressure signal noise induced by the low compliance of the simulated lung may also facilitate auto-triggering.15 In the clinical setting, low respiratory drive, respiratory frequency, and absence of hyperinflation are associated with auto-triggering.16–18
In this study, all the ventilators except for the G5 showed acceptable cycling off capability (approximately ± 50 ms), even in the presence of system leak in the COPD model. However, Ferreira et al reported that the Servo-i and the BiPAP Vision showed cycling delay times of approximately 200 ms and 800 ms respectively under similar lung mechanics and leak conditions.10 One possible reason is that we set the termination criteria to ensure that the end of inspiration of the lung model and the ventilator did not differ by more than ± 5% at baseline leak in the COPD model. In this study we set the cycling termination criteria at around 40–45% of peak inspiratory flow. In the ARDS model most of the ventilators showed premature cycling at 25% of peak inspiratory flow, due to the low compliance. In general, setting the expiratory trigger at a low percentage of the peak inspiratory flow may attenuate premature cycling. However, in the preliminary evaluation, all ventilators could not adjust the ending of inspiration to be within ± 5% of the lung model ending of inspiration at baseline leak, even when the termination criteria were set to the lowest possible values in the ARDS model; therefore we adjusted the expiratory trigger sensitivity to 25% of peak inspiratory flow. The C3 showed a prolonged inspiratory time (> 600 ms) at L2 and L3 in the ARDS model (termination criteria was set at 25% of peak inspiratory flow) but not in the COPD model (the termination criteria was set at 45% of peak inspiratory flow). In these cases we believe that system leak may prevent air flow from reaching the preset expiratory flow, leading to a prolonged inspiratory time at lower values of peak inspiratory flow. Tokioka et al reported that delayed termination with a duty cycle of > 0.5 sometimes occurred with the lowest values of termination criteria (1% of peak inspiratory flow) in 2 of 8 patients with ARDS or acute lung injury.9 In CMV, miss-triggering occurred less frequently and the ventilators required fewer breaths to synchronization than in PSV. As shown in the supplementary materials at http://www.rcjournal.com, just after the system leak was increased, cycling delay due to inspiratory system leak induced miss-triggering, resulting in a longer time to synchronization during PSV. However, in CMV, inspiratory time was fixed and cycling delay did not induce miss-triggering. This is one reason why CMV provided better synchronization than PSV. Calderini et al reported that in the presence of leaks, CMV provided better synchrony and patient comfort than PSV during NIV.19
According to our study, the leak compensation in acute care ventilators can correct partially or completely for system leak interferences, but there was wide variation among ventilators. Vignaux et al performed a bench study of 8 ICU ventilators featuring an NIV mode.20 For most of the tested ventilators, leaks led to an increase in trigger delay and a decrease in ability to reach the pressure target and delayed cycling. Similar to our findings, they found that NIV mode partially or completely corrected triggering and cycling delay, and there were marked variations between ventilators. Contrary to our study, some investigators have reported that dedicated NIV ventilators could produce better performance and synchronization than ICU ventilators in the presence of leak.7,8,21 Miyoshi et al evaluated the effects of gas leak on triggering function during NIV with dedicated NIV and ICU ventilators using a lung simulator.21 They found that the dedicated NIV ventilators triggered properly at several levels of leak (up to 44.2 L/min at 5 cm H2O) and triggering was more effective than with the ICU ventilators. However, the NIV mode was not tested in the ICU ventilators. Carteaux et al compared the operation of 8 ICU ventilators, 5 transport ventilators, and 6 NIV ventilators in NIV mode in a lung model and clinical study.11 In the lung model study they found that, even though there were wide variations in synchronization capabilities among ICU and transport ventilators, the Servo-i, PB840, and V500 could avoid auto-triggering completely when using NIV mode. In the clinical study they found that the NIV ventilators allowed better patient-ventilator synchrony than the ICU ventilators, but they did not test the Servo-i, PB840, or V500 in the clinical study. Ferreira et al evaluated the ability of 9 ICU ventilators and 1 NIV ventilator to function in the presence of leaks in a COPD model.10 As leak increased, all the ventilators except for the Servo-i and BiPAP Vision needed adjustments of triggering or cycling criteria to synchronize appropriately with the lung simulator. They concluded that the Vision had slightly better synchrony with triggering and the Servo-i with cycling. However, some ICU ventilators tested had not incorporated leak compensation. Since the manufacturers have not revealed the exact triggering and cycling algorithms used during system leak, it is difficult to explain the discrepancies among the different studies. However, considering the rapid growth of technology, it is critical to regularly repeat evaluations of ventilators to determine their ability to prevent triggering and cycling asynchrony caused by system leaks.
There were some limitations in this study. First, this study was not conducted on human subjects, raising the question of clinical relevance. However, lung simulator studies assure that the experimental conditions are the same for each ventilator evaluated. It is impossible to control the level of the leak or maintain stable baseline conditions in a clinical setting.
Another limitation is that we tested only a limited range of leaks and ventilator settings. However, we chose these to represent the range of leak flows that are likely to be encountered in clinical settings. In addition, we were interested in evaluating the maximum capabilities of the ventilators tested. Third, in some patients with acute respiratory failure, ventilatory efforts may be higher than that of our simulated respiratory efforts, and these higher efforts may affect our results.
Conclusions
All the ventilators synchronized at baseline leak, and some synchronized at low-level leak, but there were wide variations of ventilator performance. The PB840 and the V60 were the only ventilators to synchronize with simulated respiratory efforts in all leak scenarios both in NIV and invasive ventilation modes. Ventilator performance is strongly influenced by leak, lung mechanics, and PEEP setting. In clinical practice the ventilator is applied to patients with different lung mechanics, different ventilator settings, and rapid leak variations. Considering the above, the performance of a leak compensation algorithm is a crucial issue. Although it is unclear how different ventilators may affect clinical outcome, clinicians should be aware of these differences when applying leak compensation during invasive ventilation and NIV. Further studies are needed to determine the impact of different ventilators on outcome during NIV and invasive ventilation.
Footnotes
- Correspondence: Robert M Kacmarek PhD RRT FAARC, Respiratory Care Services, Massachusetts General Hospital, 55 Fruit Street, Boston MA 02114. E-mail: rkacmarek{at}partners.org.
Supplementary material related to this paper is available at http://www.rcjournal.com.
Dr Kacmarek presented a version of this paper at the AARC Congress 2012, held November 10–13, 2012, in New Orleans, Louisiana.
Deputy Editor Richard Branson guided this paper through peer review.
This research was partly supported by Covidien. Dr Kacmarek has disclosed relationships with Maquet and Covidien. The other authors have disclosed no other conflicts of interest.
See the Related Editorial on Page 2194
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}