

Abstract
BACKGROUND: The 2-min walk test (2MWT) has been used in several health conditions, but the interpretation of its results is limited due to a lack of reference values. The aim of this study was to establish a reference equation to predict the distance walked (DW) in the 2MWT for healthy adults and the elderly and to test its reproducibility.
METHODS: We evaluated 390 healthy subjects (195 male), 18–89 y old, with normal spirometry and no history of previous chronic diseases. Two 2MWTs were performed on the same day, 30 min apart. To test the reliability of the prediction equation, 70 subjects (35 male) were prospectively included in the study.
RESULTS: Men walked farther than women (221 [202–240] vs 199 [164–222] m, respectively; P < .0001). Significant correlations were observed between DW and age (r = −0.50), weight (r = 0.23), height (r = 0.40), and gender (r = 0.35) (P < .001 for all). Age and gender persisted in the model to predict DW (R2 = 0.51). There was no difference between the DW by the subjects (197 [182–216] m) and that estimated by the prediction equation (197 [179–222] m) (P = .68).
CONCLUSIONS: We established a prediction equation that may be used as a reference to interpret performance on the 2MWT of adults and the elderly with different health conditions.
Introduction
Walk tests have been widely used to assess functional capacity in different populations due to the simplicity of test performance and interpretability and its representation of daily life activities. The first walk test described in the literature was the 12-min walk test,1 adapted from the 12-min running test, more commonly known as Cooper's test.2
On the basis of arguments that the 12-min walk test might be time-consuming to the evaluator and exhaustive for the patient, Butland et al1 evaluated walking tests of shorter duration, describing for the first time the 2-min (2MWT) and 6-min (6MWT) walk tests. In this same study, the 2MWT was reproducible and better tolerated by patients with COPD; however, it exhibited less discriminative power for limitations or alterations arising from exercising. Thus, Butland et al1 determined that the 6MWT was more informative for assessing patients with COPD. Since then, the 6MWT has become the most common method for evaluating functional capacity in different health conditions. Then came the need to establish reference values for the 6MWT. Currently, there are > 10 prediction equations for distance walked (DW) in the 6MWT.3
Despite the limitations assigned to the 2MWT for patients with COPD, it has been incorporated again for use in this population and has proved to be valid for the assessment of exercise capacity and sensitive for detecting response to interventions in moderate-to-severe patients.4,5 The 2MWT has also been used in lower limb amputations,6,7 the elderly,8 neuromuscular diseases,9,10 and chronic heart diseases.11 However, no reference values have been established for the 2MWT, making it impossible to assess properly whether there is reduced functional capacity when performing this test.
The objective of this study was to establish a reference equation to predict DW in the 2MWT for healthy adults and the elderly and to test its reproducibility.
QUICK LOOK
Current knowledge
The six minute walk test (6MWT) is the standard test for evaluating exercise intolerance in patients with COPD. Both 12- and 2-min (2MWT) walk tests have been evaluated as a comparator to the 6MWT with both advantages and disadvantages identified.
What this paper contributes to our knowledge
A prediction equation for the 2MWT can be used as a reference to interpret performance on the 2MWT by adults with different health conditions. In certain conditions, the 2MWT may be preferred to the 6MWT.
Methods
Subjects
In a cross-sectional study, we evaluated 390 healthy subjects (195 male) from a convenience sample. They were recruited from 4 campuses of our university, located in 4 different regions of São Paulo; the community around the university; and relatives of our students and employees. We evaluated 30 men and 30 women 18–28, 29–39, 40–49, 50–59, 60–69, and 70–79 y old and 15 men and 15 women 80–89 y old. Fewer subjects were evaluated between 80 and 89 y of age because of the difficulty of finding individuals without musculoskeletal limitations at this age. For inclusion in the study, subjects had to be between 18 and 89 y of age and had to have normal spirometry, a body mass index (BMI) of ≤ 30 kg/m2, and no history of neuromuscular, musculoskeletal, or cardiorespiratory diseases. We excluded subjects who smoked or who had stopped smoking for < 2 y, those who had uncontrolled hypertension although using regular medication, those who practiced regular physical activity, and those who lacked the capacity to understand how to perform the spirometry and/or the 2MWT. The study was approved by the Research Ethics Committees of the Nove de Julho University (UNINOVE, 454934), and all subjects gave written consent before starting the evaluations.
Assessment
Body weight was assessed with a beam scale to the nearest 0.1 kg, with subjects standing barefoot in light clothing. BMI was calculated as weight/height (kg/m2).
Spirometry (Ultima CPX, Medical Graphics Corporation, St. Paul, Minnesota) was performed according to recommendations of the American Thoracic Society/European Respiratory Society.12 FVC and FEV1 were compared with those predicted for the Brazilian population.13
The 2MWT was performed in a 30-m corridor. Two tests were performed, with a rest interval of 30 min between them. The subjects were instructed to walk as fast as possible, without running. Based on the recommendations for the 6MWT,14 encouragement was given after the first minute with the following standardized phrases: “You're doing well” and “One minute left.” Blood pressure was measured at rest in the standing position and immediately after the test by sphygmomanometer (DS44 DuraShock, Welch Allyn, Arden, North Carolina). Subjects were instructed to stop the test if they experienced chest pain, dizziness, malaise, or any other symptoms of discomfort. Pulse oxygen saturation was continuously measured (Biox 3740, Ohmeda, Boulder, Colorado), as was heart rate (S810 frequency meter, Polar, São Paulo, Brazil). The values recorded were those shown on the display of the equipment at rest, at the end of the first minute, and at the end of the second minute. The variation of heart rate and SpO2 were considered as the values at the peak of the exercise minus the value at rest. The predicted maximum heart rate was calculated as 220 − age in years. The peak heart rate was expressed in absolute and predicted (peak heart rate/maximum predicted) values. The modified Borg scale was used for evaluation of dyspnea and leg fatigue.15
Statistical Analysis
The normality of the data was analyzed by the Shapiro-Wilk test. The data showed nonparametric distribution and were expressed as median (interquartile range 25–75%). Differences in DW between men and women were analyzed using the Mann-Whitney test. The test with the farthest DW was selected for the next analysis. Spearman's correlation coefficient was used to correlate the independent variables (age, weight, and height) with the dependent variable (DW). For multiple regression analysis (stepwise), gender was added to the independent variables for definition of the predictive equation. The lower limit of the normal range was calculated as predicted value − (1.64 × residual SD). The intraclass correlation coefficient (ICC) and Bland-Altman analysis16 were used to assess the reproducibility of the two 2MWTs. Comparisons of DW among the age groups were performed using the Kruskal-Wallis and Mann-Whitney tests on each pair of groups, with the P value adjusted by the Bonferroni method. The reliability of the prediction equation was tested by comparing the DW performed by the subjects (DWactual) with that estimated by the equation (DWpredicted) using the Mann-Whitney test and Bland-Altman analysis.
Results
The baseline characteristics are shown in Table 1.
Characteristics of the Subjects
The comorbidities more prevalent among the subjects were systemic hypertension (18%), diabetes mellitus (3%), and thyroid disorders (3%).
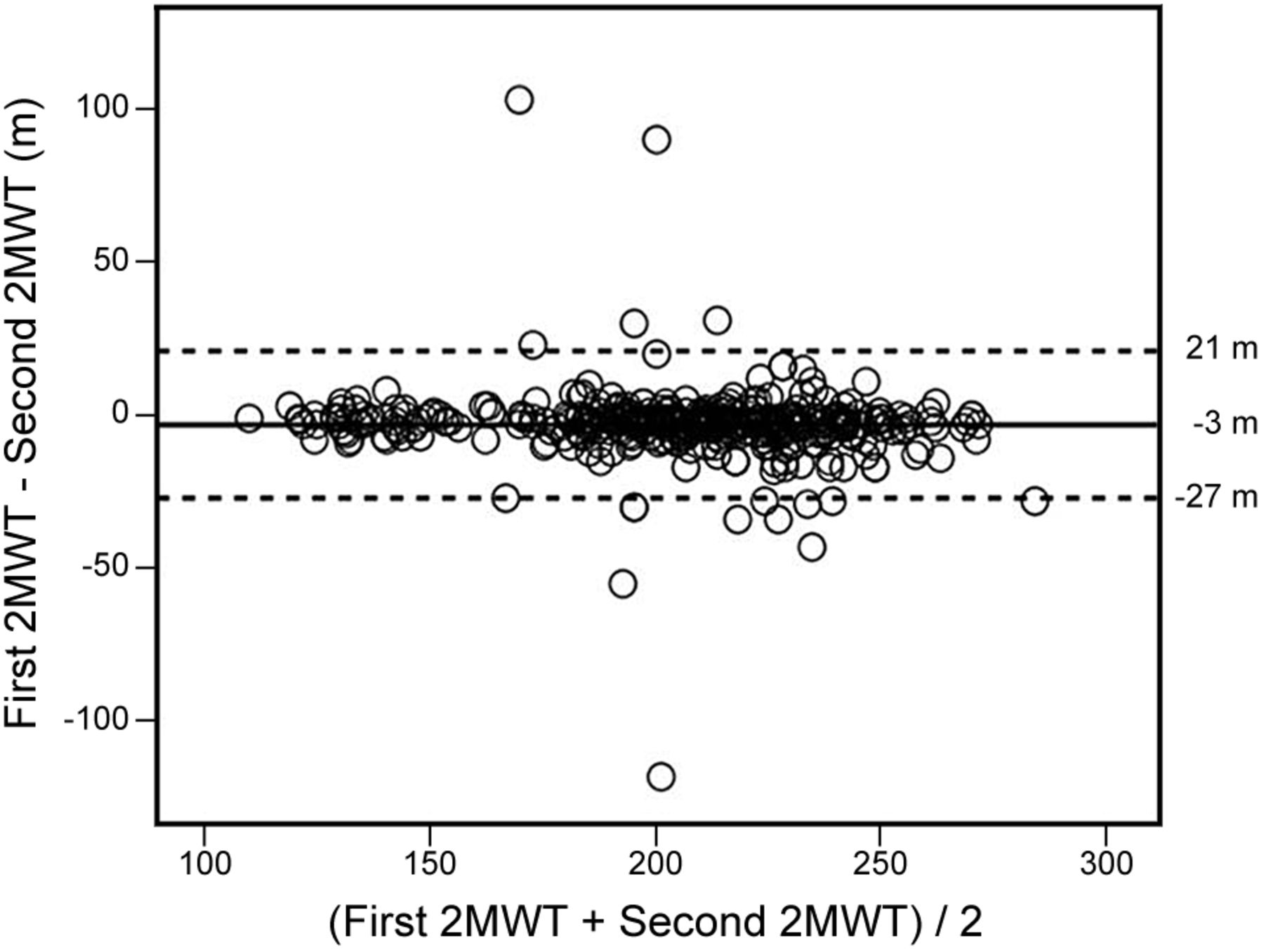
The majority of the subjects (n = 295) presented the best performance (ie, a greater DW) in the second 2MWT, 73 subjects walked farther in the first test, and 22 walked the same distance in both tests. There were no significant differences in the outcomes measured at rest and at the peak of the two 2MWTs (Table 2). The mean difference between the first and second 2MWTs was narrow (Fig. 1).
Data at the Peak of the 2-Min Walk Test

Distance walked in first and second 2-minute walk tests (2MWT).
The male subjects walked farther than the female subjects (221 [202–240] vs 199 [164–222] m, respectively; P < .001). The difference did not persist when correcting the DW/height (127 [104–140] vs 128 [118–139], respectively; P = .054). Significant correlations were observed between DW and age (r = −0.50), weight (r = 0.23), height (r = 0.40), and gender (r = 0.35) (P < .001 for all), but not BMI (r = −0.08, P = .14). There was a reduction in DW in the 2MWT with advancement of age (Fig. 2). The reduction in DW was 11.5 m (−4.9%) from 18–28 to 29–39 y of age, 10.5 m (−4.7%) from 29–39 to 40–49 y, 6 m (−2.8%) from 40–49 to 50–59 y, 11.5 m (−5.5%) from 50–59 to 60–69 y, 9 m (−4.6%) from 60–69 to 70–79 y, and 13 m (−6.9%) from 70–79 to 80–89 y. The average decline over the ages was 10 m (−4%). Between the extreme ages (18–28 and 80–89 y), the reduction in DW was 61.5 m (−26%).
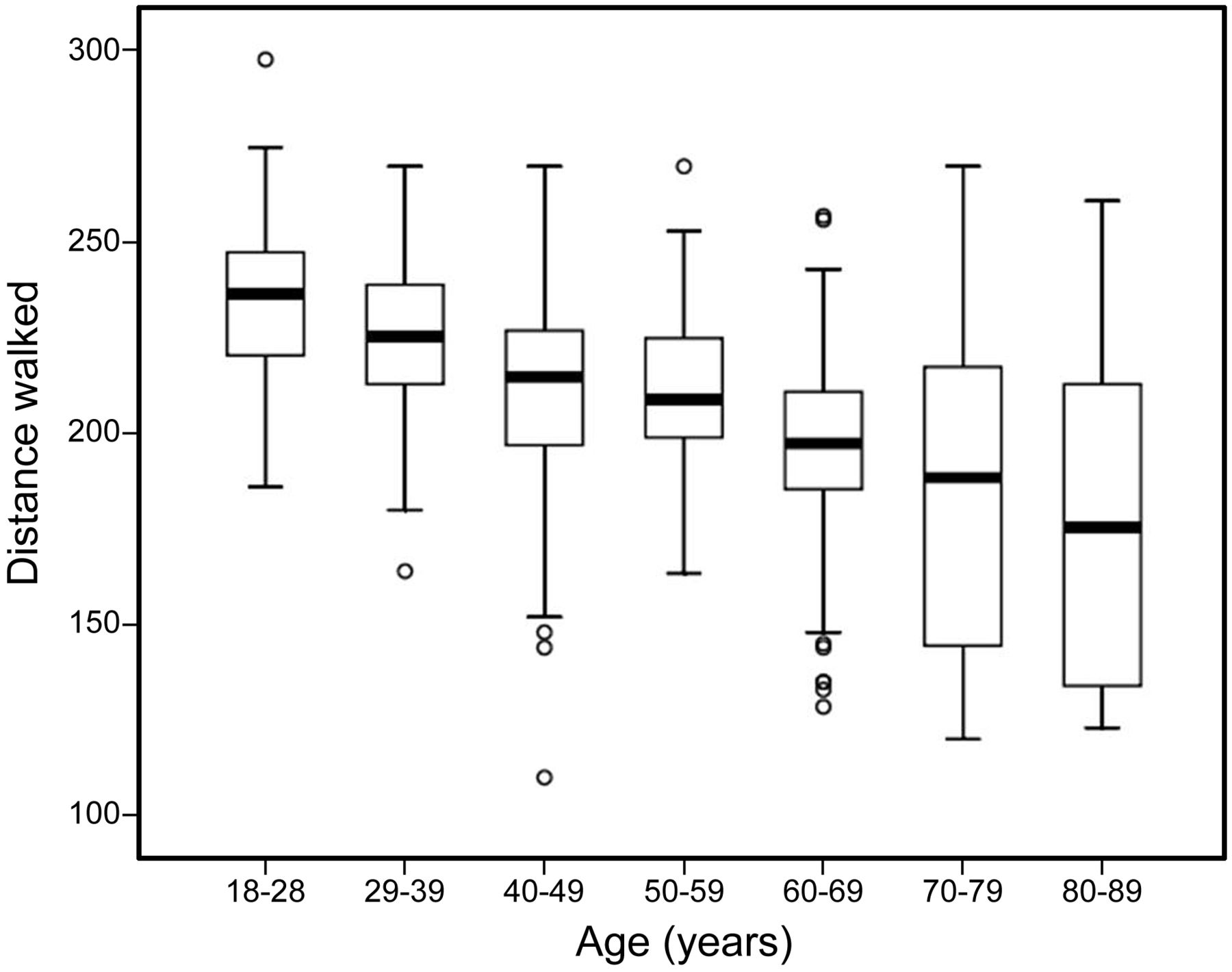
Influence of age on distance walked in the 2-minute walk test. For the 18-28-y age group, P = .02 compared to the 29-39-y age group, and P < .001 compared to the older age groups. For the 29-39-y age group, P = .03 compared to the 40-49-y age group, P = .007 compared to the 50-59-y age group, and P × .001 compared to the older age groups. For the 40-49-y age group, P = .83 compared to the 50-59-y age group, P = .03 compared to the 60-69-y age group, and P = 0.001 compared to the older age groups. For the 50-59-y age group, P = .03 compared to the 60-69-y age group, and P < 0.001 compared to the older age groups. For the 60-69-y age group, P = .10 compared to the 70-79-y age group, and P = .005 compared to the 80-89-y age group. P = .21 for the 70-79-y age group compared to the 80-89-y age group. The horizontal line in the middle of each box represents the median. The top and bottom borders of the box mark the 75th and 25th percentiles, respectively, and the whiskers above and below the box mark the 90th and 10th percentiles, respectively. Circles beyond the whiskers represent outliers.
Among the independent variables selected from the simple regression analysis (age, weight, height, and gender), age and gender persisted to predict DW in the model, explaining 51% of its variance. The data from the multiple linear regression analysis are shown in Table 3. The reference equation for DW in the 2MWT was 2MWTpredicted = 252.583 − (1.165 × age) + (19.987 × gender*), where * is male = 1 and female = 0. The lower limit of the normal range is DWpredicted − 44 m.
Predictor Variables for Distance Walked in the 2-Minute Walk Test Obtained From Multiple Linear Regression Analysis
To test the reliability of the prediction equation, 70 subjects (35 male) were prospectively included in the study (age: 53 [34–71] y; weight: 68 [59–77] kg; height: 1.64 [1.59–1.70] m; BMI: 25 [22–28] kg/m2; FVC (% predicted): 96 [85–103]; and FEV1 (% predicted): 99 [89–104]). There was no difference between DW by the subjects (DWactual = 197 [182–216] m) and that estimated by the prediction equation (DWpredicted = 197 [179–222] m) (P = .68). The DW for the prospective sample corresponded to 99% (96–105) of that predicted.
Discussion
The present study provides an equation to predict DW in the 2MWT. Age and gender explained 51% of the variance in DW. Moreover, men presented better performances compared with women, and the 2MWT is highly reproducible in healthy subjects.
There are currently several equations to predict DW in the 6MWT,3 and there are two for the incremental shuttle walk test (ISWT),17,18 but there has been no reference equation for the 2MWT. Age and gender are variables commonly present in prediction equations for walking tests. Age and gender were also the only predictor variables of DW in two previous studies of the 6MWT, and the coefficients of determination were lower than those observed in the present study (R2 = 0.41 and 0.30).19,20 The strength of association between age and DW in the 2MWT found in our study (r = −0.50) is consistent with that (from r = −0.36 to r = −0.75) observed in studies that have established prediction equations for the 6MWT.19–25 The inverse relationship between age and exercise capacity is well known because normal aging is characterized by reduced functional reserve capacities of the heart, lung, and skeletal muscles, as well as decreased levels of physical activity.26–28 Our data showed a substantial reduction in DW (−61.5 m) when comparing the youngest (18–29 y) and oldest (80–89 y) ages. In a previous study of the 6MWT, DW decreased by 16% from 40–49 y (611 ± 85 m) to 70–80 y (514 ± 71 m).29 Considering the similar ages in our study (40–49 and 70–79 y), the reduction observed was ∼12%. This confirms that, even in short-duration tests, such as the 2MWT, it is possible to observe the impact of aging on the ability to walk. However, future studies evaluating longitudinal decline in DW per decade would confirm whether the cross-sectional decline was equivalent.
On average, in the present study, men walked 12% more than women, which is a percentage similar to that found in previous studies on the 6MWT.19,23,30,31 The influence of gender on DW has been demonstrated previously in the 6MWT by either of these conditions: prediction equation specific for gender30 or gender as a predictor variable in the prediction equation.19,20,22,32–34 Aerobic capacity, represented by maximum oxygen uptake, is ∼30% lower in women compared with men.35,36 Consequently, women exhibit lower performances in tests of physical capacity, including the 2MWT.
The regression equation of the present study, applied prospectively, was demonstrated to be reliable for estimating DW in the 2MWT. To illustrate the use of our prediction equation, we expressed the absolute values of DW in the 2MWT for people with lower limb and transtibial amputations6,7 and subjects with COPD4,5 as a percentage of the predicted value from our prediction equation. Considering that 95% of the total sample of amputees was made up of male subjects,6 we calculated the predicted DW for the male gender only, which resulted in 196 m. The best DW for these subjects was 121 m (second 2MWT), which corresponded to 62% of the predicted value. In another study of amputees,7 the best DW of in-patient transtibial amputees (57.5 m) corresponded to 29% and 32% of the predicted value in males and females, respectively; for out-patient transtibial amputees, the best DW was 140.7 m, corresponding to 67% for males and 74% for females. In the study performed by Leung et al4 (n = 45; 37 males; 71.8 y old; FEV1 = 42 ± 13% of predicted) with COPD patients, we also calculated the predicted values for males, as 82% of the subjects were male. On average, patients walked 130.8 m, representing 69% of the predicted values from our prediction equation. Cardiac surgery patients11 walked 68% of the predicted distance preoperatively and 42% postoperatively. Therefore, subjects presented with reduced functional capacity not only because of the low values in relation to the percentage of predicted but also because the DW was lower than the lower limit of the normal range (121 vs 152 m for amputees, 140.7 vs 165 m for out-patient transtibial amputees, 130.8 vs 145 m for COPD patients, and 136 vs 155 m for cardiac surgery patients). Considering the responsiveness of the 2MWT, a study5 has shown that patients with COPD (n = 57; 30 males; 69 y old; FEV1 = 35 ± 12% of predicted) walked 153 and 162 m in the 2MWT before and after use of a bronchodilator, respectively, corresponding to 79.7% and 84.4% of the predicted values obtained from our prediction equation, considering male subjects. In addition to the improvement in terms of absolute values (9 m), DW reached values > 80% of the predicted values after use of a bronchodilator. After pulmonary rehabilitation, it is an interesting highlight that the improvement in DW in the 2MWT, expressed as a percentage of our predicted values, was 11.5%, quite similar to that observed in the 6MWT (14%), taking into consideration the predicted values of Enright and Sherrill.30
In the present study, on average, subjects achieved 70% of the predicted maximum heart rate, which is similar to what was observed at the peak of the 6MWT by healthy subjects (64%) with a mean DW of 587 m.20 As both the 2MWT and 6MWT are self-paced tests, it is possible that the heart rate achieved during the second minute corresponds to the rest-exercise transition. From this point until the sixth minute, it could remain constant, which would correspond to the steady state. We could not find studies about the behavior of blood pressure during the 2MWT. Higher values of systolic blood pressure were found at the peak of ISWT17 in comparison with that observed in the present study (160 vs 140 mm Hg). This result was expected, as speed is gradually increased in the ISWT, and the test is not time-limited.
The reproducibility of any method must be tested to ensure that its result is reliable so as to ensure that the differences found are due to interventions or to the patient's evolution and not a result of oscillations because of variability of the method itself. Reproducibility is therefore an indication of the consistency of a measure and is usually evaluated by ICC; coefficients above 0.80 indicate high reliability.35 The reproducibility of DW in the 2MWT has been tested in patients with COPD,1,5 congestive heart failure,36 or poliomyelitis9; in the elderly8; and in amputees.7 DW in the 2MWT in these previous studies showed evidence of reliability, with ICCs ranging from 0.828 to 0.99,7 which is compatible with that observed in our study (0.96 [0.95–0.97]).
Another analysis we used to assess the reproducibility of DW in the 2MWT was the Bland-Altman graphical distribution, which is based on a dispersion diagram, facilitating the interpretation of the magnitude of the disagreement between two measures (ie, DW in two 2MWTs). In the present study, the limits of agreement in the Bland-Altman analysis ranged from −27 to 21 m, which can be considered similar to those found in subjects with poliomyelitis (−21 to 23 m)9 and the elderly (−21 to 21 m).8 This means that, independent of the health condition, the subject is able to walk a similar distance in two 2MWTs performed on the same day.
Conclusions
We established a prediction equation for the 2MWT that may be used as a reference to interpret performance on the 2MWT by adults and the elderly with different health conditions.
Footnotes
- Correspondence: Simone Dal Corso PhD, Postgraduate Program in Rehabilitation Sciences, Universidade Nove de Julho (UNINOVE), Rua Vergueiro 235/249, 2° subsolo, 01504-001 São Paulo, Brazil. E-mail: simonedc{at}uninove.br.
Ms Selman was supported by São Paulo Research Foundation grant FAPESP-2012/13314-0. Mr de Camargo received a master fellowship grant from the Programa de Suporte à Pós-Graduação de Instituições de Ensino Particulares (PROSUP)/Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). Dr Dal Corso is an Established Investigator of the Conselho Nacional de Desenvolvimento Tecnológico (CNPq). This study was supported by São Paulo Research Foundation grant FAPESP-2010/09732-6. The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}