

Abstract
BACKGROUND: Xbox Kinect has been proposed as an exercise intervention in cystic fibrosis (CF), but its potential has not been compared with standard training modalities.
METHODS: Using a crossover design, subjects were randomized to 2 intervention groups: Xbox Kinect and a traditional stationary cycle. Heart rate, SpO2, dyspnea, and fatigue were measured. Subject satisfaction was tested.
RESULTS: Thirty subjects with CF (11 males, mean ± SD age of 12 ± 2.5 y, mean ± SD FEV1 of 73 ± 16% of predicted) were enrolled. Xbox Kinect provided a cardiovascular demand similar to a stationary cycle, although the modality was different (interval vs continuous). Maximum heart rates were similar (P = .2). Heart rate target was achieved more frequently with a stationary cycle (P = .02). Xbox Kinect caused less dyspnea (P = .001) and fatigue (P < .001) and was more enjoyable than a stationary cycle (P < .001).
CONCLUSIONS: Subjects preferred Xbox Kinect for its interactivity. Xbox Kinect has the potential to be employed as an exercise intervention in young subjects with CF, but investigation over longer periods is needed.
Introduction
Cystic fibrosis (CF) is a multi-organ genetic disorder, but its clinical outcome involves mostly the respiratory system. Viscous mucus secretions obstruct airways, leading to recurrent and often subsequent chronic infections.1 The course of the disease is marked by periodic exacerbations, resulting in increased coughing, more dense sputum, weight decrease, and a decline in pulmonary function.1 Many subjects with CF refrain from physical activity due to fatigue and shortness of breath, which are now believed to be caused by not only poor pulmonary function but also deficits in skeletal muscle aerobic and anaerobic capacity and reduced muscle strength.2,3
This is critical, as aerobic fitness has been shown to be a key predictor of disease prognosis and mortality in subjects with CF, independent of factors such as age, sex, lung function, and nutritional status.4 Moreover, physical activity and exercise training in CF have been reported to improve or slow down the rate of decline of important prognostic indicators such as lung function and aerobic fitness.5 Reduction in exercise capacity is associated with a decline in respiratory function and survival.6
Children and adolescents with CF have a reduced ability to tolerate exercise. Nixon et al7 showed that children and adolescents with CF engaged in less vigorous physical activities compared with their healthy non-CF counterparts, despite having good lung function and nutritional status. The physical activity levels of prepubescent children with CF seem to be similar to or even higher than those of healthy controls. However, in pubescent or postpubescent subjects with moderate-to-severe CF, physical activity appears to be reduced.8
This has serious implications for their well-being and quality of life and limits the opportunities for their involvement in sports and recreational activities. Understanding the efficacy of using exercise training to promote physical fitness, well-being, and longevity is therefore critical in young patients with CF.5
Physical exercise has a potential therapeutic effect in CF, and it has therefore become a mainstay of the physiotherapy treatment for CF.9 In fact, in the last decades, aerobic exercise has been recommended for subjects with CF as an adjunctive therapy (recommendation grade of B).10 Therefore, this is an area of interest to clinicians, either as a prognostic or therapeutic tool.9 General exercise and training recommendations in children and adolescents with CF have already been defined in terms of method, frequency, duration, and intensity.11 Exercise programs should be tailored to individual needs, as there is considerable variability between subjects in terms of fitness, enthusiasm, and preference for particular types of activities.12 A recent review of physical activity levels in subjects with CF assessed the effect of an exercise program on participation in physical activity, but underscored the lack of evidence regarding strategies for promoting the commencement of and adherence to regular physical activity.13 It seems very important to consider the type of training when prescribing exercise. Children and adolescents experience greater difficulty than adults in adhering to exercise routines, and one of the most common reasons for non-adherence in young CF subjects is that traditional forms of exercise bore them.14 Strategies suggested to improve adherence should include an enjoyable, supervised, and individualized activity.
On the basis of the high prevalence of television and video game activities, some researchers have evaluated using these devices as stimulating strategies for exercise in young people.15,16 In addition, gaming console exercises may be more attractive to children because of their pre-existing experience playing video games.17 Active video games are expected to improve self-esteem, self-efficacy, knowledge, skills, communication, and social support, all of which are mediating factors that can improve health behaviors and outcomes.18 Active video games provide instant visual and audio feedback and are goal-oriented and enjoyable; therefore, they have the potential to improve motivation and adherence to an exercise program.15–18
The burden of treatment placed on patients with CF and their families is often high, involving time-consuming and complex therapies. There are many factors that influence willingness to participate in regular activity over a period of time, including factors external to the subject (eg, social support), perception of self-competency, self-esteem, enjoyment of the activity, and factors associated with the subject's behavior (eg, motivation and choice). Support from family, instructors (coaches, teachers, and the health-care team), and peers is influential in determining activity-related self-esteem and therefore activity behavior.12
An exercise program using a gaming console may improve exercise adherence in children and adolescents with CF because the exercise is purported to be fun, which may increase motivation to exercise. Interactive gaming consoles may have the potential to replace or supplement traditional exercise programs because they result in greater enjoyment. The aims of the study were to compare both the cardiovascular demand produced and perceptions of dyspnea, fatigue, and enjoyment of pediatric subjects with CF while using Xbox Kinect versus traditional stationary cycle training.
QUICK LOOK
Current knowledge
Exercise as part of a comprehensive pulmonary rehabilitation program has been shown to reduce the decline in lung function and improve quality of life in patients with cystic fibrosis (CF). A reduced exercise capacity is associated with a decline in respiratory function and survival. Implementing a self-directed exercise program for patients with CF remains a challenge.
What this paper contributes to our knowledge
An exercise program for CF subjects using an Xbox Kinect resulted in similar changes in heart rate as traditional cycle ergometry. Subject enjoyment was greater with the Xbox, and muscle fatigue and dyspnea were lower. Use of the Xbox did not create a similar cardiovascular demand as traditional exercise.
Methods
Subjects
Pediatric CF subjects who had been admitted to a hospital for a 15-d programmed intravenous antibiotic cycle were recruited after obtaining informed consent. Inclusion criteria were: a CF diagnosis based on a positive sweat test and/or a confirmed CF genotype, age between 8 and 17 y inclusive, mild-to-moderate air-flow obstruction (FEV1 > 40% of predicted), and a stable clinical condition. Subjects started the exercise sessions within 72 h of discharge. Exclusion criteria included oxygen therapy, presence of hypercapnia defined as a carbon dioxide level of > 45 mm Hg, presence of any genomovar of Burkholderia cepacia, or skeletal muscle disease or any other disorder that impairs exercise capacity (eg, musculoskeletal pain, bone fractures, recent surgery, neurological problems). The study protocol was approved by the institutional review board (CE 78CESC).
Study Design
This randomized crossover trial was conducted at the Cystic Fibrosis Centre in Verona, Italy. Each subject received standard in-hospital care, which included intravenous antibiotics and chest physical therapy. During hospitalization, subjects were instructed to maintain their usual chest physical therapy sessions and physical activity and to perform the usual chest physical therapy sessions in the morning, at least 3 h before exercise. They consumed their usual lunch ∼3 h before all sessions. The subjects participated in 2 exercise interventions in the afternoon on separate days within 72 h of discharge: one intervention involved exercising using the gaming console (Xbox Kinect, Microsoft, Redmond, Washington), and the other involved exercising on a traditional stationary cycle. Subjects were randomly allocated to the order of exercise interventions using a computer-generated random sequence (Microsoft Excel). Allocation was concealed with the use of consecutively numbered envelopes. The statisticians who analyzed the data were blinded to the type of exercise assigned.
Sample Size Definition
The primary end point of the study was the difference in the maximum heart rate between the 2 exercise interventions. To detect a difference in the maximum heart rate of 10 beats/min, with an SD of the paired differences of 15, it was necessary to recruit 26 subjects considering a 2-sided α of 0.05 and β = 0.1. Expecting a dropout of 10%, 30 subjects were enrolled to reach the target sample size after the possible dropout.
Exercise Interventions
The gaming console used for the experimental intervention was Xbox Kinect. Kinect is a motion-sensing input device for the Xbox 360 video game console. Based on a wireless controller add-on peripheral for the Xbox 360, it enables users to control and interact with the video game in 3 dimensions without the need to touch a game controller, using only gestures and spoken commands. The Kinect Adventures program (composed of 5 mini-games) was used. River Rush was chosen as the most challenging. The control intervention consisted of high-intensity, constant, aerobic stationary cycle exercise to reach the heart rate target for this population: 80% of the maximum heart rate for age.11 Specific indications were provided to subjects for both activities.
For the experimental intervention, subjects were told that Xbox Kinect works with a body scanner (Kinect) that analyses and reproduces their body movements. The game chosen was River Rush, in which subjects stand in a virtual raft and control it by stepping left or right to steer and by jumping. Subjects were requested to move within the body-scan space for the proper interaction with the video game. The aim of the game is to collect a certain number of pins along the river. There are 3 levels (easy, intermediate, and difficult) with a corresponding incremental effort. Each level lasts ∼6 min with a 1-min rest time while the next level loads.
During the control intervention, subjects performed continuous aerobic cycle training with a gradual increase in the intensity level to maintain heart rate within a set level. The cycling speed was kept constant despite the changes in resistance. Subjects cycled slowly at a lower intensity at the beginning (2-min warmup) and end (2-min cooldown) of the exercise session. Each exercise intervention lasted 20 min.19
During the exercise sessions, the children wore a portable heart rate monitor (Pulsox-300i, Konica Minolta, Osaka, Japan) via a finger probe to monitor SpO2 and heart rate. These parameters were measured continuously, and the respiratory physiotherapist recorded values at baseline and every 5 min for the stationary cycle or at the end of each level for Xbox Kinect. All sessions were monitored by a respiratory physiotherapist. The exercise interventions were stopped if the subjects exhibited any signs of intolerance: severe dyspnea (visual analog scale score of ≥ 9), oxygen desaturation (SpO2 during exercise of ≤ 88%), or excessively high heart rate (≥ 200 beats/min).
Outcome Measures
The primary outcome measures were heart rate and subject enjoyment. The secondary outcome measures were SpO2, level of dyspnea using the visual analog scale with a happy-face pain-rating scale, and perception of fatigue using the Children's OMNI-Step Scale.
To evaluate dyspnea, we used a vertical scale quantified from 0 to 10 (visual analog scale score of 0–10), in which 0 represents no dyspnea and 10 represents maximum dyspnea. We associated the pictorial descriptors (5 faces) of the visual happy-face pain-rating scale to facilitate the evaluation of this symptom. We explained to subjects that each face is for a person who feels happy because he has no shortness of breath or who feels sad because he has some or a lot of shortness of breath. The subject chose the number from 0 to 10 with the aid of the face images.
To evaluate perception of fatigue, we used the Children's OMNI-Step Scale.20 The term OMNI is a contraction of the word omnibus and refers to a numerical category scale that employs interchangeable sets of mode-specific pictorial descriptors positioned along a visually discernible exertional intensity gradient. The pictorials for the Children's OMNI-Step Scale depicted either a girl or boy performing various step exercise intensities with the corresponding numbers from 0 to 10. Heart rate, SpO2, and visual analog scale scores for dyspnea and muscle fatigue were recorded at rest and every 5 min for the stationary cycle or at the end of each level of Xbox Kinect. Subjects were asked to rate their level of enjoyment after each experimental condition using a 5-point Likert-type scale, where 1 = disagreement and 5 = strong agreement.
Statistical Analysis
All measurements were subjects to an intention-to-treat analysis. Descriptive statistics were reported as percentages for categorical variables and as median, range, and mean ± SD for continuous variables according to the normal distribution of data. Box-and-whisker plots were used to represent continuous variables: the bottom and top of the box represent the first and third quartiles, the band inside the box represents the median, and the dot corresponds to the mean. The ends of the whiskers represent the minimum and maximum.
Continuous variables were compared using the paired t test: the maximum value over the period was considered (heart rate, SpO2, and visual analog scale scores for dyspnea and muscle fatigue). To compare the target (reached vs not reached) and the enjoyment (much/very much vs none/little/quite) between the 2 exercise modes, the McNemar test was applied. Statistical significance was set at P < .05. All analyses were performed using SAS 9.2 (SAS Institute, Cary, North Carolina).
Results
Thirty subjects (11 males, 36.7%) were enrolled and completed the study. Subjects were children and adolescents (mean ± SD age of 12 ± 2.5 y, range of 7.7–16.6) and showed mild-to-moderate lung function (mean ± SD FEV1 of 73 ± 16% of predicted, range of 45–101) at the end of the intravenous antibiotic cycle. All exercise sessions were tolerated by subjects, and no sessions were prematurely stopped. Heart rate, SpO2, and dyspnea and fatigue measurements during rest and each intervention are presented in Table 1.
Heart Rate, SpO2, and Visual Analog Scale Scores for Dyspnea and Muscle Fatigue at Rest and During Each Exercise Intervention
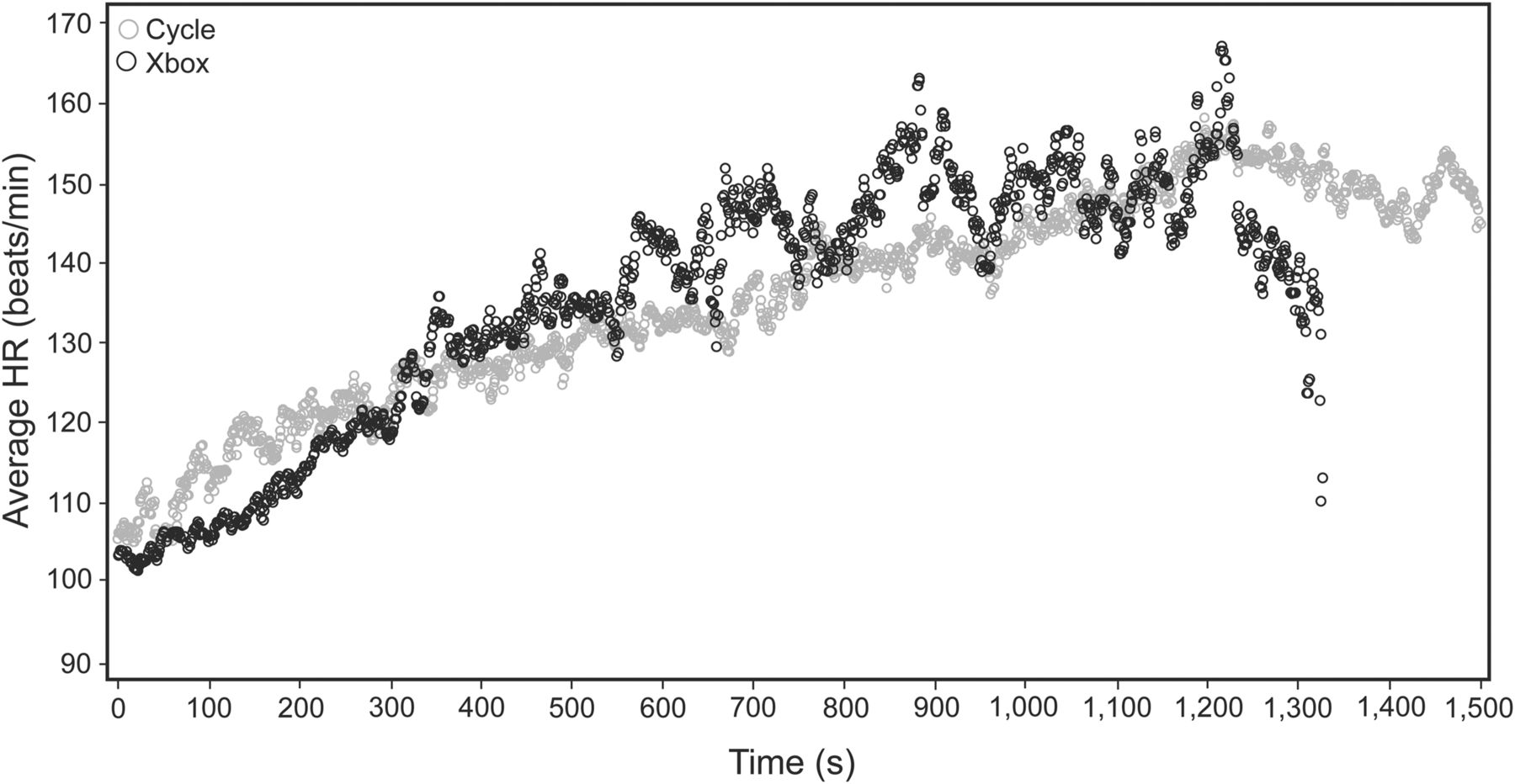
Figure 1 presents the cardiorespiratory responses to exercise with Xbox Kinect and a stationary cycle. Maximum heart rate was determined according to the equation 220 − age in years,21 which leads to a range of 203–212 beats/min in our population. The target was computed considering 80% of the maximum heart rate.11 A mean value of 166 beats/min (range of 162.4–169.6) was obtained. During the 20-min exercise session, there was no significant difference in the maximum heart rate reached over time between the Xbox Kinect (mean ± SD beats/min of 165.0 ± 23.6) and stationary cycle (170.8 ± 13.2, P = .2) groups, but the heart rate target was reached more often with the stationary cycle (20 of 30 subjects) compared with Xbox Kinect (12 of 30 subjects, P = .02). The percentage of subjects who reached 80% of their maximum heart rate at any point during training was 67% for the stationary cycle group and 40% for the Xbox Kinect group. In addition, heart rate showed an incremental trend in both experimental conditions: continuous in the stationary cycle group and discontinuous in the Xbox Kinect group (Fig. 2). SpO2 was slightly lower for the Xbox Kinect group at baseline but was similar during the 2 exercise interventions. Xbox Kinect provided a lower level of dyspnea (P = .001) and fatigue (P < .001). The subjects reported that Xbox Kinect exercise was more enjoyable than traditional stationary cycle exercise (P < .001), as shown in Figure 3.

Comparison of cardiorespiratory responses during exercise with a stationary cycle and Xbox. A: heart rate (HR) at various times/levels with reference to the target heart rate. B: SpO2 measured via pulse oximetry. C: dyspnea measured using a visual analog scale (happy-face pain-rating scale). D: perception of fatigue using the Children's OMNI-Step Scale. Whiskers denote the minimum and maximum values. The bottoms and tops of boxes represent the first and third quartiles. The middle lines and dots represent the median and the mean value, respectively. Horizontal lines in A represent target heart rate range (162–169 beats/min).

Distribution of average heart rate (HR) every second.

Subject enjoyment.
Discussion
Recent advances in technology have facilitated the development of virtual reality, enhanced, physical activity programs, and the new generation of active video games may offer the potential to meet some of the challenges associated with exercise adherence in patients with CF. An exercise program using a gaming console may improve exercise adherence among young subjects with CF because it is perceived to be enjoyable, which may increase motivation.
We believe that children and adolescents with CF are an appropriate audience for the use of active video games. Therefore, we studied the outcomes of training sessions using an Xbox Kinect game (River Rush) in a group of children and adolescents with CF. In the literature, there are few articles about use of active video games in subjects with CF. Kuys et al22 showed that Nintendo Wii induced significantly higher maximum and minimum heart rates compared with cycle ergometry or treadmill exercise in 19 adults with CF admitted to the hospital. In that study, subjects enjoyed the gaming console more than standard-care exercise.
O'Donovan et al23 recorded no significant difference in exercise intensity reached by children with CF compared with healthy children when using Nintendo Wii. Playing Wii Boxing resulted in light-intensity physical activity, whereas playing Wii Fit Free Jogging resulted in moderate-intensity physical activity. The authors concluded that active video games with Nintendo Wii are a useful source of light-to-moderate-intensity physical activity in children with CF. Holmes et al24 found that exercise with the Your Shape Fitness Evolved program for Xbox Kinect was high intensity and therefore likely to be a suitable alternative to conventional exercise modalities. They compared the intensity of exercise achieved while using this interactive gaming console with peak exercise capacity measured during a cardiopulmonary exercise test in a group of adults with CF. Their results demonstrated that the mean intensity of exercise elicited during Xbox Kinect activity, expressed as a percentage of the peak heart rate achieved in the cardiopulmonary exercise test, was 86% (95% CI 81–92). The cardiopulmonary exercise test is performed on a cycle ergometer and consists of 3 min of rest and 3 min of unloaded pedaling, followed by an incremental phase of exercise every minute (5–25 W/min) until the subject reaches volitional exhaustion or the test is terminated by the medical monitor. Xbox Kinect is a non-laboratory aerobic exercise in which the peak heart rate may not be reached. The peak heart rate achieved with the cardiopulmonary exercise test results from a controlled laboratory-based test, whereas with Xbox Kinect, it is the effect of cardiovascular changes during a free unstructured physical activity.
In this study, we compared cardiorespiratory responses and enjoyment in 2 different experimental conditions: Xbox Kinect game playing and exercise with a traditional stationary cycle. Although our data suggest that both experimental conditions induce a significant increase in maximum heart rate, the heart rate target was reached more often during stationary cycle exercise (20 of 30 subjects) than during Xbox Kinect exercise (12 of 30 subjects). We investigated only one short session of exercise with Xbox Kinect, and we could not establish whether Xbox Kinect provides a sufficient cardiovascular training stimulus. We hypothesize that increasing the duration of the Xbox Kinect exercise session or selecting a different Xbox Kinect modality may help more subjects to reach the heart rate target. In addition, heart rate increase was discontinuous with Xbox Kinect exercise, but showed a linear trend during stationary cycle exercise. It could be argued that Xbox Kinect exercise is similar to interval training; in fact, gaming console exercises use a number of different matches (2 for every level), each lasting for up to 2–3 min. The River Rush game contained 5 rest pauses (1 min each) between each match due to the console game-loading time. However, a discontinuous exercise does not exclude the benefits of aerobic training. Indeed, high-intensity interval training involves repeated exercise at a high intensity for 30 s to several min, separated by 1–5 min of recovery (either no or low-intensity exercise). It is associated with increased subject compliance and improved cardiovascular and metabolic outcomes.25
In terms of perception of effort, our data indicate that dyspnea and muscle fatigue were greater during stationary cycle exercise compared with Xbox Kinect exercise. The perception of fatigue during stationary cycle exercise often exceeded values of 5–6, corresponding to an intense effort related to achievement of the heart rate target. The severity of dyspnea was also significantly different between the 2 types of exercise and was increased during stationary cycle exercise. It has been demonstrated that interval training allows work of maximal intensity to be performed with a relatively low perception of dyspnea compared with continuous training26 and produces similar improvements in exercise performance and quality of life.27 The game playing used in our study involves the whole body, as opposed to stationary cycling, which involves predominantly the lower limbs. Gulmans et al28 investigated the effects of a 6-month cycling program in 14 children with CF. After completion of a cycle training program, exercise tolerance, oxygen uptake, leg muscle strength, and feelings of perceived competence significantly increased. The authors found a significant increase in leg muscle strength in 2 of 3 muscle groups of the lower extremities, with no differences in the upper extremities. The subjects considered a cycle ergometer as unacceptable because of the intensity (perceived exertion) and the lack of exercise variation, as shown accordingly by our results. For this reason, the cycle ergometer may not be the most effective and appreciated instrument to train children with CF.
Of note, in this study, we showed that subjects expressed more enjoyment when training with Xbox Kinect, and we know that this is a key factor in exercise adherence. Our data are in line with other reports.15,18,22 In addition, our results suggest that a type of training such as a stationary cycle is an efficient way to train cardiovascularly, but it may not be an effective exercise program if children with CF do not enjoy it and, as such, have poor participation. We showed that interaction, presence of feedback, and variation in the exercise program influence enjoyment. The River Rush game for Xbox Kinect gives constant feedback that motivates the player to reach the goal. This game also offers the motivation of different levels, and therefore, it is unlikely that a player will lose concentration, compared with a standard cycling exercise session. Further studies are necessary to determine the long-term results on exercise capacity and adherence to an exercise program with Xbox Kinect compared with a traditional stationary cycle.
Conclusions
Xbox Kinect induces a significant increase in maximum heart rate, but we could not establish if it provides a cardiovascular demand similar to a traditional stationary cycle. Subjects expressed greater enjoyment when using Xbox Kinect with a lower perception of dyspnea and muscle fatigue. Based on these preliminary data, it would be advisable to investigate the medium-to-long-term effects of an Xbox Kinect-based physical exercise program on cardiovascular adaptation and exercise adherence in subjects with CF.
Acknowledgments
We thank all of the subjects who took part in this study and their parents.
Footnotes
- Correspondence: Elena Salonini PT, Centro Fibrosi Cistica, Azienda Ospedaliera Universitaria Integrata, Piazzale Stefani 1, 37126 Verona, Italy. E-mail: elena.salonini{at}ospedaleuniverona.it.
Dr Assael has disclosed relationships with Vertex and Gilead. The other authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}