

Abstract
BACKGROUND: The SARS-CoV-2 pandemic increased the number of patients needing invasive mechanical ventilation, either through an endotracheal tube or through a tracheostomy. Tracheomalacia is a rare but potentially severe complication of mechanical ventilation, which can significantly complicate the weaning process. The aim of this study was to describe the strategies of airway management in mechanically ventilated patients with respiratory failure due to SARS-CoV-2, the incidence of severe tracheomalacia, and investigate the factors associated with its occurrence.
METHODS: This retrospective, single-center study was performed in an Italian teaching hospital. All adult subjects admitted to the ICU between February 24, 2020, and June 30, 2020, treated with invasive mechanical ventilation for respiratory failure caused by SARS-CoV-2 were included. Clinical data were collected on the day of ICU admission, whereas information regarding airway management was collected daily.
RESULTS: A total of 151 subjects were included in the study. On admission, ARDS severity was mild in 21%, moderate in 62%, and severe in 17% of the cases, with an overall mortality of 40%. A tracheostomy was performed in 73 (48%), open surgical technique in 54 (74%), and percutaneous Ciaglia technique in 19 (26%). Subjects who had a tracheostomy performed had, compared to the other subjects, a longer duration of mechanical ventilation and longer ICU and hospital stay. Tracheomalacia was diagnosed in 8 (5%). The factors associated with tracheomalacia were female sex, obesity, and tracheostomy.
CONCLUSIONS: In our population, approximately 50% of subjects with ARDS due to SARS-CoV-2 were tracheostomized. Tracheostomized subjects had a longer ICU and hospital stay. In our population, 5% were diagnosed with tracheomalacia. This percentage is 10 times higher than what is reported in available literature, and the underlying mechanisms are not fully understood.
- severe acute respiratory syndrome
- SARS-CoV-2
- mechanical ventilation
- airway management
- tracheostomy
- tracheomalacia
Introduction
Italy was hit by the first pandemic wave of a new coronavirus,1 subsequently named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), at the end of February 2020. The novel virus causes a disease named coronavirus disease 2019 (COVID-19), which has a wide variety of clinical presentations, ranging from asymptomatic carriers to severe cases of ARDS. ICU admission, endotracheal intubation, and mechanical ventilation are frequently required in patients with severe COVID-19.2-6
Tracheostomy is a common procedure in the ICU, particularly in difficult-to-wean patients.7 Tracheostomy can be performed either percutaneously or surgically.8 The first is associated with fewer infections and bleeding, whereas the latter guarantees less risk of posterior wall injury and accidental decannulation.8 Acquired tracheomalacia is a rare but potentially life-threatening complication of intubation and mechanical ventilation.9 The incidence and risk factors associated with tracheomalacia in critically ill patients with COVID-19 are currently unknown.
The aims of the present study are, therefore, (1) to describe the strategies of airway management in critically ill patients with COVID-19, (2) to describe the incidence of tracheomalacia, and (3) to investigate possible factors associated with the development of tracheomalacia.
QUICK LOOK
Current Knowledge
The current SARS-CoV-2 pandemic is markedly increasing the number of patients undergoing invasive mechanical ventilation. Therefore, the use of tracheostomy in COVID-induced ARDS is more frequent compared to the classical ARDS (32–60%), and it is associated with longer ICU length of stay. Artificial airway management in the ICU is associated with multiple complications, including tracheomalacia. Risk factors for development of tracheomalacia in the adult population are COPD and chronic inflammation, trauma, infection, prolonged intubation, and tracheostomy.
What This Paper Contributes to Our Knowledge
We analyzed airway management modalities in 151 critically ill, mechanically ventilated subjects with COVID-19 admitted to the ICUs of one of the largest hospitals in Italy during the first SARS-CoV-2 pandemic wave. We observed that tracheostomized subjects had a longer duration of mechanical ventilation and longer ICU and hospital length of stay. No difference in mortality was observed between subjects with tracheostomy versus subjects without. Tracheomalacia was diagnosed in 5% of subjects, which is a higher percentage than reported in literature. In our study, obesity, female gender, and tracheostomy were associated with the development of tracheomalacia.
Methods
This single-center, observational retrospective study was approved by the local ethical committee (approval number: 593–06102020). The need for informed consent from individual subjects was waived owing to the retrospective nature of the study. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology statement guidelines for observational studies.
All patients admitted between February 22, 2020, and June 30, 2020, inclusive for those days, to the 5 COVID-19 ICUs of the Grande Ospedale Metropolitano Niguarda were screened for eligibility. Laboratory-confirmed SARS-CoV-2 infection, (ie, positive result of real-time reverse transcriptase-polymerase chain reaction assay of nasal or pharyngeal swabs) and ICU admission for acute respiratory failure constituted the inclusion criteria. Exclusion criteria were age < 18 y, admission for causes other than respiratory failure, and patients admitted for respiratory failure but treated exclusively with noninvasive respiratory support.
The clinical management followed local protocols and suggestions from scientific societies.10 The decision to perform a tracheostomy was at the discretion of the attending physicians. Tracheostomy was considered in patients without evidence of coagulopathy, whose respiratory function had stabilized (mainly PEEP ≤ 10 cm H2O and  ≤ 0.6), where it was unlikely to require further cycles of prone positioning, if the clinician predicted a prolonged and difficult weaning from mechanical ventilation. The procedure was performed either by 2 surgeons, with the assistance of an anesthesiologist (surgical technique), or by 2 anesthesiologists (percutaneous technique).
≤ 0.6), where it was unlikely to require further cycles of prone positioning, if the clinician predicted a prolonged and difficult weaning from mechanical ventilation. The procedure was performed either by 2 surgeons, with the assistance of an anesthesiologist (surgical technique), or by 2 anesthesiologists (percutaneous technique).
Subjects included in the analysis were divided into 2 groups according to their airway management: (1) subjects treated with endotracheal tube only and (2) subjects who had a tracheostomy performed in the ICU. A subgroup of subjects where tracheomalacia was first suspected clinically and then confirmed through an endoscopic evaluation (performed by an experienced thoracic surgeon, SC) was identified. Tracheomalacia was defined, according to available literature, as a weakness of the trachea, likely due to a reduction and/or atrophy of the elastic fibers, determining a tendency to tracheal collapse.9
Data Collection
Clinical data were extracted from the patient data management system, and a unique database was created using the web-based software REDCap (electronic data capture tools). For every included subject, we recorded demographic and anthropometric data, comorbidities, and medical history. Clinical data, including but not limited to severity scores, vital signs, respiratory mechanics, and gas exchange, were collected on the day of ICU admission. Information regarding airway management, that is, performance of a tracheostomy, extubation, or decannulation, was collected daily until ICU discharge or subject’s death. Moreover, information regarding tracheostomy complications, such as bleeding and stomal infections, was collected retrospectively. The final date of follow-up for patient outcomes was July 31, 2020, and the following patient outcomes were recorded: ICU and hospital survival, ICU and hospital length of stay, duration of invasive mechanical ventilation, incidence of tracheostomy, and incidence of tracheomalacia.
Statistical Analysis
All data were tested for homogeneity of variance and normality of distribution using the Shapiro-Wilk test. Normally distributed data were expressed as mean ± SD, whereas non-normally distributed data were reported as median and interquartile range. Binary data were summarized as percentages frequency of occurrence. To compare study groups (tracheostomy vs nontracheostomy and tracheomalacia vs nontracheomalacia), Mann-Whitney rank-sum test and chi-square test or Fisher exact test was used for nonparametric continuous variables and categorical variables, respectively. All statistical tests were 2-tailed, and statistical significance was defined as P < .05. The analyses were performed using SigmaPlot 12.0 (Systat Software, San Jose, California).
Results
Overall Study Population
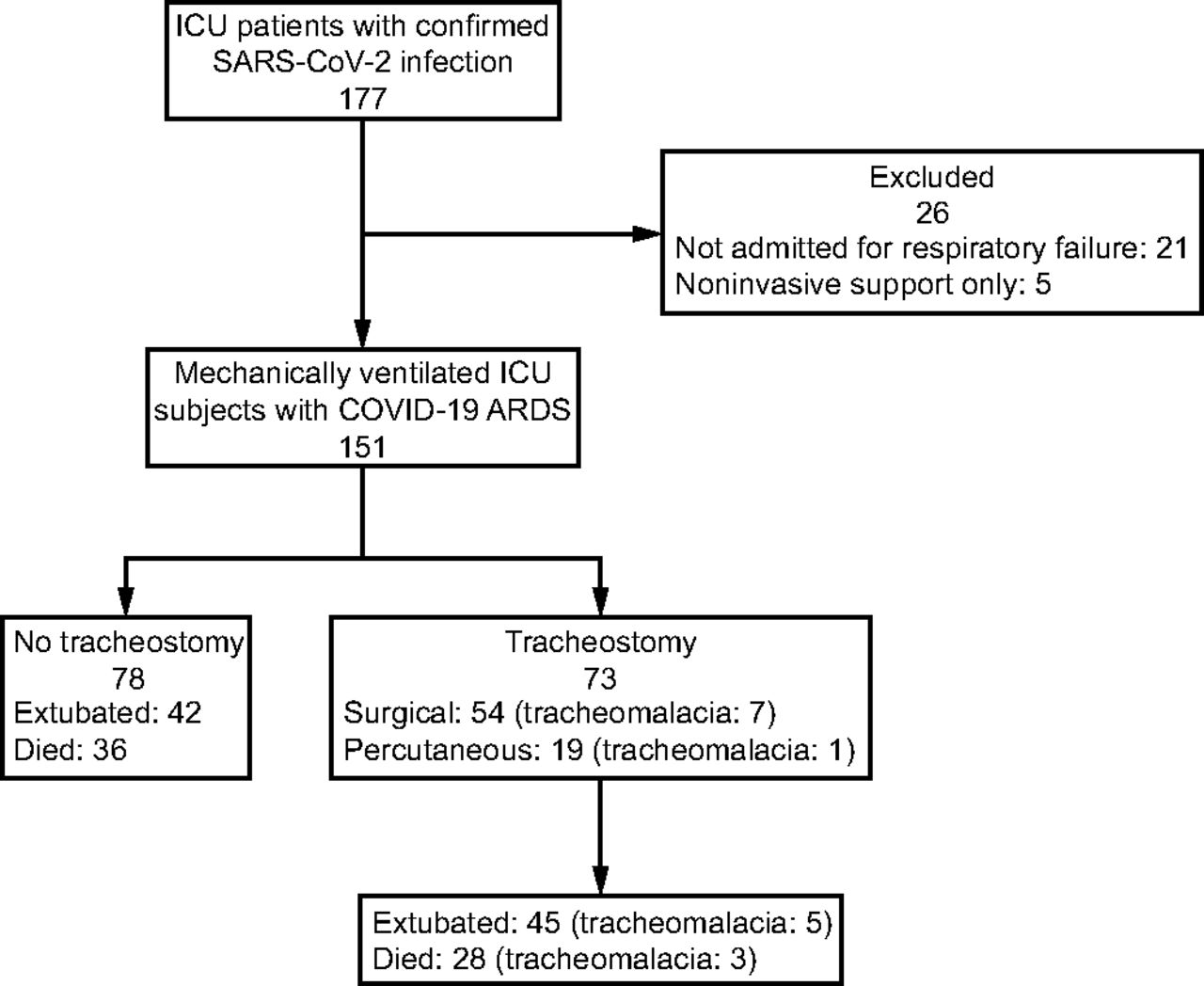
A total of 177 patients were admitted to the ICU with laboratory-confirmed SARS-CoV-2 infection during the study period. Twenty-six patients were excluded (in 21 patients the admission was not primarily for respiratory failure, and 5 patients received exclusively noninvasive ventilation), leaving 151 subjects for analysis (Fig. 1).

Flow chart.
Table 1 summarizes baseline characteristics of the study population at ICU admission and their clinical outcomes. In the study population, 116 (77%) were male and 50 (33%) were obese (body mass index [BMI] > 30 kg/m2). The most common comorbidities were hypertension (48%), diabetes mellitus (15%), and COPD (12%). At ICU admission, median (IQR) APACHE and SOFA scores were 23 (21–27) and 5 (3–7), respectively; and ARDS severity was mild in 21%, moderate in 62%, and severe in 17%. One or more infective complications (microbiologically confirmed) were reported in 81 (54%) during the ICU stay. Fifty-six (37%) subjects developed sepsis, and in 32 (21%) it worsened into septic shock. The median (IQR) duration of antibiotic therapy was 6 (2–15) d. Overall, median ICU and hospital length of stay were 14 (9–27) d and 26 (14–46), respectively. Sixty (40%) died in the ICU; mortality increased according to disease severity at admission (25%, 40%, and 58%, P = .04, for mild, moderate, and severe ARDS, respectively).
Subjects’ Characteristics at Admission in ICU and Outcome. Comparison Between Tracheostomized Subjects and Subjects Treated With Endotracheal Tube Exclusively
Tracheostomy Practice and Comparison With Endotracheal Tube
A tracheostomy was performed in 73 (48%) subjects. There was no significant difference in the performance of tracheostomy according to ARDS severity at admission (41%, 51%, and 50%, P = .62 for mild, moderate, and severe ARDS, respectively). The approach was surgical in 54 (74%) cases and percutaneous, using a single-dilator Ciaglia technique, in the remaining 19 (26%) cases. The median time of tracheostomy performance was 11 (8–15) d after tracheal intubation. Differences between the subgroup treated exclusively with endotracheal intubation and the subgroup undergoing a tracheostomy are reported in Table 1.
Mortality in the ICU did not differ between tracheostomized subjects and subjects treated exclusively with endotracheal intubation (34% vs 45%, respectively, P = .24). Subjects who had a tracheostomy performed had a significantly longer duration of mechanical ventilation (25 [15–36] vs 8 [5–12] d, P < .001) in both ICU (27 [17–39] vs 9 [5–14] d, P < .001) and hospital length of stay (45 [27–58] vs 17 [9–26] d, P < .001).
Fifty-four percent of tracheostomized subjects developed at least one infective complication, as compared to 27% in subjects treated with endotracheal tube exclusively (P < .001). Moreover, sepsis and septic shock during the ICU stay occurred more often in tracheostomized subjects (60% vs 15%, P < .001 and 32% vs 12%, P = .005, respectively). Bacterial pneumonia was the most common infection (62% vs 23%, P < .001) followed by bloodstream infections (64% vs 22%, P < .001). The median duration of antibiotic therapy was longer in tracheostomized subjects (15 [6–21 vs 3 [0–6] d, P < .001).
Complications related to tracheostomy were recorded in 32 subjects. Bleeding occurred in 16 (22%) tracheostomized subjects, and 3 cases required blood transfusions. Stoma infection was reported in 23, and in 6, antibiotics were prescribed. Finally, 3 tracheoesophageal fistula cases were diagnosed (4% tracheostomized subjects).
Incidence of Tracheomalacia and Associated Factors
In the overall study population, tracheomalacia was diagnosed in 8 (5%). Figure 2 shows an endoscopic image of a subject with tracheomalacia and SARS-CoV-2 ARDS. The diagnosis was performed 27 (21–32) d after endotracheal intubation. Compared to the remaining population (Table 2), more subjects with diagnosed tracheomalacia were female (75% vs 20%, P = .002; odds ratio 11.8, 95% CI 2.3–61.5) and obese (88% vs 30%, P = .003, OR 16.3, 95% CI 1.9–136.4). All subjects diagnosed with tracheomalacia were treated with a tracheostomy for airway management (100% vs 45%, P = .008). No difference was found regarding the use of the surgical approach (87.5% vs 72.3%, P = .67), the timing of tracheostomy (11 [7–14] d vs 11 [8–17], P = .37), and decannulation (35 [23–56] d vs 19 [14–33], P = .11) comparing subjects that developed tracheomalacia with the remaining population. Conversely, the duration of mechanical ventilation (29 [22–34] d vs 13 [8– 24], P = .007) was significantly longer in subjects diagnosed with tracheomalacia.

An endoscopic image showing a tracheal malacia in a subject with SARS-CoV-2 ARDS.
Comparison Between Subjects With and Without a Diagnosis of Tracheomalacia
All subjects with tracheomalacia developed one or more microbiologically confirmed infections during ICU stay (100% vs 51%, P = .02). Sepsis was reported more frequently (75% vs 35%, P = .057), and the median duration of antibiotic therapy was longer (22 [5–28] d vs 6 [2–15], P = .02) in subjects who were diagnosed with tracheomalacia. Similarly, ICU and hospital length of stay were significantly longer in these subjects (29 [24–41] d vs 14 [8–26], P = .006 and 55 [35–90] d vs 25 [13–43], P = .002, respectively). Of note, the 3 trachea-esophageal fistula cases observed occurred in subjects who had tracheomalacia diagnosed. ICU and hospital mortality were not different between subjects with tracheomalacia and the remaining subjects (25% vs 41%, P = .61 and 38% vs 43%, P = .94, respectively).
Discussion
In this single-center, retrospective observational study, we analyzed the modalities of airway management in 151 critically ill, mechanically ventilated subjects with COVID-19, admitted to the ICUs of one of the largest hospitals in Italy, during the first SARS-CoV-2 pandemic wave. In addition, we focused our attention on subjects that were diagnosed with tracheomalacia during their ICU stay.
A major finding of our study is that a tracheostomy was performed in almost 50% of subjects treated with invasive mechanical ventilation for COVID-19-related respiratory failure and that in our cohort of subjects the incidence of tracheostomy was not different according to admission ARDS severity. These findings differ markedly from what has been described in the classic ARDS population. Indeed, a recent worldwide observational study evaluating the incidence and characteristics of subjects with ARDS in the ICU described that a tracheostomy was performed in 13% of the overall ARDS population,11 increasing from 9.6% in mild to 14.5% in severe ARDS.12 On the contrary, recent literature regarding COVID-induced ARDS already described an increased use of tracheostomy, in line with our findings, ranging from 32–60%.13-16
The major contributing factor to this high incidence of tracheostomies might be the fact that patients with COVID-induced ARDS seem to require more time to improve, as compared to classic ARDS.13 Indeed, in our population, the median ICU length of stay was 14 (9–27) d, which is longer as compared to the 10 (5–20) d of the LUNG SAFE study.12 The reasons for this longer ICU stay have not been fully understood. It is conceivable that several aspects related to COVID pathophysiology, such as the marked vascular and endothelial involvement,14 a high rate of secondary bacterial infections,15,17 and a high incidence of barotrauma,18-19 contribute to the longer course of the disease. Indeed, a high rate of bacterial infections is reported also in our cohort of subjects, more frequently in tracheostomized subjects with a longer stay.
Another aspect that deserves discussion is the high percentage of surgical tracheostomies in our cohort. Italy was the first European country hit by the 2020 pandemic. In spring 2020, the knowledge about the novel β-coronavirus was extremely scarce, and no data were available about the safety of health care professionals performing tracheostomies in infected patients. Performing a tracheostomy is certainly a procedure at very high risk for infection. In addition, the generation of aerosol particles, potentially containing the virus, is certainly favored in critically ill patients by the necessity to use high-positive intrathoracic pressures. The idea that a surgical approach would be safer for the operator and the fact that surgeons were relatively free, due to the suspension of elective surgery, explain our finding. There is no evidence to recommend one method over the other, and the daily availability of an experienced surgical team avoided delays. Moreover, percutaneous tracheostomy might involve more extensive manipulation of the airway with increased aerosolization risk.20,21 In addition, it is certainly true that a surgical tracheostomy guarantees an easier cannula repositioning in case of accidental removal. This aspect might be of particular importance in the context of a pandemic surge characterized by the presence of inexperienced doctors and nurses in the ICU. Of note, several studies described that the surgical technique was not associated with higher complication rates.22-24
In our study, we compared the characteristics of subjects who had a tracheostomy performed with those ventilated exclusively via an endotracheal tube (Table 1). The major difference was a longer disease course in tracheostomized subjects, as demonstrated by a longer duration of mechanical ventilation and longer ICU and hospital length of stay. Moreover, tracheostomized subjects developed bacterial infections more frequently. No difference in mortality was observed in the 2 groups. Of course, our data are purely descriptive, and no conclusions on the effect of tracheostomy on COVID-induced ARDS can be drawn. Indeed, it is conceivable that the performance of a tracheostomy is a proxy of a complicated clinical course, (eg, difficult weaning from the mechanical ventilator or slow resolution of interstitial pneumonia).
Other authors investigated the use of tracheostomy in SARS-CoV-2 patients, describing the overall safety of the procedure.23,25-33 Several studies reported a longer ICU stay in tracheostomized subjects.28,34 The cohort of the Queen Elizabeth Hospital Birmingham26 is the only one describing a higher 30-d survival in subjects undergoing tracheostomy as compared to those who did not. Whereas the authors accounted for disease severity in their analysis, it is important to underline the observational, nonrandomized nature of the study.
Finally, in the present study, we focused our attention on tracheomalacia, a rare complication of mechanical ventilation. Several factors are considered a risk for the development of tracheomalacia. In the general adult population, the most important one seems to be chronic inflammation in the context of COPD.9 On the other hand, despite less evidence, trauma, infections, prolonged intubation, and tracheostomy have been considered potential risk factors.35-38
In our cohort, 8 (5%) of 151 subjects’ tracheomalacia was suspected clinically and confirmed with a fiberoptic evaluation. To the best of our knowledge, this is the largest report of tracheomalacia in COVID subjects. A single case of tracheomegaly, with clinical features similar to our subjects, has been recently described.39
The observed 5% is higher compared to the scarce literature, only referring to non-COVID patients. Karimpour and colleagues40 described that 0.6% of 184 subjects who underwent percutaneous Ciaglia tracheostomy in the ICU developed tracheomalacia, whereas Kandaswamy et al41 described an incidence of 0.7% in a case-control study including 576 mechanically ventilated subjects, regardless of the presence of a tracheostomy. Several factors could explain the observed higher incidence. On the one hand, a vascular and endothelial involvement in patients with COVID-19 has been described,42 particularly in the lungs. To the best of our knowledge, the microvascular involvement of the upper airways has not been documented so far; however, from a surgical perspective, we observed a macroscopic impairment of the vascularization of tracheal and peritracheal tissues.
Another factor potentially implied with the pathogenesis of tracheomalacia in this particular pandemic context is an excessive cuff pressure of the endotracheal/tracheostomy tube potentially leading to tracheal wall suffering. Usually, great attention is paid to this aspect by the nursing staff. However, on the one hand, the presence of inexperienced nurses, recruited from regular wards due to the extremely high number of patients in need, and on the other hand, the fear of infection due to cuff leakage and viral spread could have resulted in overall higher cuff pressures. Finally, it is conceivable to hypothesize a role of mechanical trauma of the tracheostomy tube on the tracheal wall during pronation.6
In our cohort, subjects diagnosed with tracheomalacia had a significantly longer clinical course (ICU and hospital length of stay), a higher rate of bacterial infections, but a similar mortality. In addition, we observed that subjects diagnosed with tracheomalacia had a higher BMI, were more frequently female, and the use of tracheostomy was higher.
On the one hand, the physiologic gender-related differences in connective tissue43-44 could maybe explain the observed higher incidence in females. On the other hand, the higher BMI, already identified as a potential risk factor,40 could be explained by the pro-inflammatory effect of obesity45-46 and a more difficult surgical or percutaneous access to the trachea during the performance of the tracheostomy. Moreover, obesity and obstructive sleep apneas might favor the development of tracheomalacia as a result of periodic markedly negative intrathoracic pressures generated during episodes of obstruction.47 Of course, this would imply that at least a mild form of tracheomalacia was already present before the COVID infection and was somehow exacerbated during the critical illness.
We observed a higher incidence of infections and a longer course of antibiotic therapy in the group of subjects with tracheostomy and with tracheomalacia. Certainly, the longer duration of ICU stay could simply have increased the probability of developing new bacterial infections, but the impact of repetitive infective events and the consequent systemic inflammation might have contributed to the pathophysiology of tracheomalacia.
The management of acquired tracheomalacia associated with mechanical ventilation is difficult and requires a multidisciplinary approach involving critical care physicians, anesthesiologists, thoracic surgeons, and respiratory therapists. The approach might be surgical35,38,48,49 endoscopic stent placement35,38,50 or conservative management with cycles of positive-pressure ventilation.35,41 In our cohort of subjects, a conservative approach, based on spontaneous breathing cycles and positive pressure after decannulation, was successful in subjects with isolated tracheomalacia, that is, in subjects that had not developed a tracheoesophageal fistula.
Limitations
Several limitations of our study need to be mentioned, first, its retrospective, single-center nature; second, the related limited sample size and associated statistical limitations. Indeed, given the low number of events of tracheomalacia, a multiple logistic regression model could not be performed.51 Moreover, a fiberoptic evaluation was performed only in subjects where tracheomalacia was suspected clinically. It is, therefore, conceivable that some cases of tracheomalacia were missed either in case of mild forms, not triggering a fiberoptic evaluation, or in subjects who died before extubation/decannulation. The real incidence of tracheomalacia could, therefore, be higher.
A comment on the potential role of the performance of a tracheostomy on the development of tracheomalacia is necessary. We have observed that all subjects that developed tracheomalacia had been previously tracheostomized. However, as stated above, tracheostomy was performed in subjects with predicted difficult and prolonged weaning from mechanical ventilation and might, therefore, be considered as a proxy for a complicated clinical course. The independent role of the performance of a tracheostomy is, therefore, very difficult to assess, and our data are thus inconclusive regarding this aspect.
Conclusions
In our cohort of 151 critically ill subjects with COVID-related ARDS, we observed that almost 50% mechanically ventilated subjects were tracheostomized. This percentage is significantly higher as compared to the classic ARDS population. Furthermore, we observed that 5% of the studied population was diagnosed with tracheomalacia. Again, this percentage is significantly higher than the available reports of non-COVID ICU patients. Obesity, female gender, and tracheostomy might play a role in the development of this rare and severe condition.
Footnotes
- Correspondence: Thomas Langer MD, Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy; Department of Anesthesia and Intensive Care Medicine, Niguarda Ca’ Granda, Milan, Italy. E-mail: Thomas.Langer{at}unimib.it
See the Related Editorial on Page 1927
The study was performed at the Department of Anesthesia and Intensive Care Medicine, Niguarda Hospital, Milan, Italy.
The authors have no conflicts to disclose.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}