

Abstract
BACKGROUND: Subjects with thoracic scoliosis were an important group in early studies of noninvasive ventilation (NIV). The aim of this study was to describe current rates of initiation of NIV and survival after initiation in this population.
METHODS: This study included patients identified as having thoracic scoliosis and established between 1993 and 2018 on home NIV. Patients with scoliosis secondary to neuromuscular disease (other than poliomyelitis) were excluded. Survival rates were calculated for various time intervals up to 25 y.
RESULTS: A total of 53 subjects with thoracic scoliosis were successfully established on NIV.  levels prior to starting NIV were 55 ± 23 mm Hg. FVC was 0.5 ± 0.1 L, 18.5 ± 9% of predicted, with a Cobb angle of 101 ± 3.5 degrees. The 5-, 10-, 15-, 20-, and 25-y survival rates were 96%, 88%, 61%, 46%, and 39%, respectively. At the time of death, subjects had been on home NIV for 9.2 ± 5.1 y and were 75.5 ± 9.2 y old. There was no significant correlation between mortality and age at time of commencing home NIV, initial arterial blood gas results, FVC, or Cobb angle. There was no significant difference in survival between those with and without poliomyelitis. In 8 of 10 of the most recent years of this survey, subjects with scoliosis have been commenced on home NIV.
levels prior to starting NIV were 55 ± 23 mm Hg. FVC was 0.5 ± 0.1 L, 18.5 ± 9% of predicted, with a Cobb angle of 101 ± 3.5 degrees. The 5-, 10-, 15-, 20-, and 25-y survival rates were 96%, 88%, 61%, 46%, and 39%, respectively. At the time of death, subjects had been on home NIV for 9.2 ± 5.1 y and were 75.5 ± 9.2 y old. There was no significant correlation between mortality and age at time of commencing home NIV, initial arterial blood gas results, FVC, or Cobb angle. There was no significant difference in survival between those with and without poliomyelitis. In 8 of 10 of the most recent years of this survey, subjects with scoliosis have been commenced on home NIV.
CONCLUSIONS: Small numbers of subjects with scoliosis continued to present with respiratory failure. Once established on home NIV, around 40% survived ≥ 25 y. Long-term care will be needed for many years to come for this patient population.
- scoliosis
- spine
- chest wall
- poliomyelitis
- respiratory failure
- hypercapnia
- noninvasive ventilation
- intermittent positive-pressure ventilation
- forced vital capacity
Introduction
Noninvasive ventilation (NIV) using positive airway pressure applied via a mask (or mouthpiece) was first developed in the 1980s and rapidly surpassed older methods of supporting breathing such as iron lungs, cuirasses, rocking beds, and pneumobelts. NIV proved to be particularly effective in correcting type 2 (hypercapnic) respiratory failure in individuals with thoracic scoliosis, these patients being one of the main diagnostic groups in the early reported series on its long-term use.1-10 We report a retrospective cohort analysis of home NIV in subjects with scoliosis over a 25-y period, with the aim of describing current rates of initiation of NIV and survival after initiation in this population.
Quick Look
Current Knowledge
Patients with thoracic scoliosis were among the first to benefit from noninvasive ventilation (NIV) when it was introduced more than 30 years ago. Now that the indications for NIV have been extended to obesity-hypoventilation, COPD, and many neuromuscular conditions, those with scoliosis are at risk of receiving less attention.
What This Paper Contributes to Our Knowledge
Subjects with thoracic scoliosis continued to present with respiratory failure, albeit in small numbers. With home NIV, survival rates were ∼ 40% at 25 years. Long-term care will be needed for many years to come for this small but important group.
Methods
Our unit provides a regional home ventilation service, with specialist neurological and spinal surgery services also based at our hospital. From our database of home ventilation users, we identified those with scoliosis who had been commenced on home NIV between 1993 and 2018. The criteria for commencing home NIV were daytime  > 52.5 mm Hg or a rise in overnight transcutaneous carbon dioxide level of > 7.5 mm Hg above awake values, associated with symptoms of nocturnal hypoventilation. We identified 7 patients (4 female and 3 male, median age 55 y) who were unable to use NIV for an average of > 4 h in a 24-h period; we deemed these patients not to have been successfully established on long-term NIV, and we excluded them from further analysis.11,12 We also excluded patients with scoliosis associated with progressive neuromuscular diseases (eg, muscular dystrophy, spinal muscular atrophy), but we included those with poliomyelitis.
> 52.5 mm Hg or a rise in overnight transcutaneous carbon dioxide level of > 7.5 mm Hg above awake values, associated with symptoms of nocturnal hypoventilation. We identified 7 patients (4 female and 3 male, median age 55 y) who were unable to use NIV for an average of > 4 h in a 24-h period; we deemed these patients not to have been successfully established on long-term NIV, and we excluded them from further analysis.11,12 We also excluded patients with scoliosis associated with progressive neuromuscular diseases (eg, muscular dystrophy, spinal muscular atrophy), but we included those with poliomyelitis.
Spinal curvature was assessed from spinal radiographs by calculation of the Cobb angle.13 FVC and FEV1 were measured using a wedge-bellows spirometer, with predicted values taken from the Global Lung Initiative,14 substituting arm span for height.15 Survival was assessed with the Kaplan-Meier method. A log-rank test was used to compare survival in those with and those without a history of poliomyelitis. Risk factors for death were assessed using multivariate analysis. Results are expressed as mean ± SD unless stated otherwise. The level of statistical significance was taken as 0.05. The study was approved by the Clinical Ethics Committee of Nottingham University Hospital.
Results
We identified 53 subjects who were successfully established on home NIV over the 25 y of the survey (Table 1). Twenty-seven of the subjects were female; 31 had idiopathic or congenital scoliosis, 17 had post-poliomyelitis, 3 had kyphoscoliosis following spinal tuberculosis, and in 2 subjects spinal curvature was associated with osteogenesis imperfecta. Eight subjects had a diagnosis of asthma or COPD, and 5 were current or former smokers.
Demographics of Subjects With Thoracic Scoliosis at Start of NIV
Subjects used pressure-targeted NIV with a nasal mask. Inspiratory positive airway pressure was 27 ± 1.3 cm H2O. The cycling of NIV was based on a fixed time rather than being triggered by the subject, with a breathing frequency of 15 ± 1.1 breaths/min. Most subjects had an expiratory valve in the NIV circuit, with no positive airway pressure during expiration. Five (9%) used NIV for “top-up” periods during the day, in addition to overnight.16
The 5-, 10-, 15-, 20-, and 25-y survival rates were 96%, 88%, 61%, 46%, and 39%, respectively. At the time of death, subjects had been on home NIV for 9.2 ± 5.1 y and were 75.5 ± 9.2 y old. There was no significant association between mortality and age at time of commencing home NIV, initial arterial blood gas results, FVC, FEV1, or Cobb angle. When the subjects with scoliosis secondary to poliomyelitis were compared to those in whom the etiology was idiopathic or congenital, there was no significant difference in survival (Fig. 1). Figure 2 shows the total number of subjects using home NIV by year, together with the number of new subjects starting each year. Subjects with scoliosis started home NIV in 8 of the 10 most recent years of our survey.

Survival with home noninvasive ventilation of subjects with idiopathic or congenital scoliosis, or scoliosis secondary to poliomyelitis.
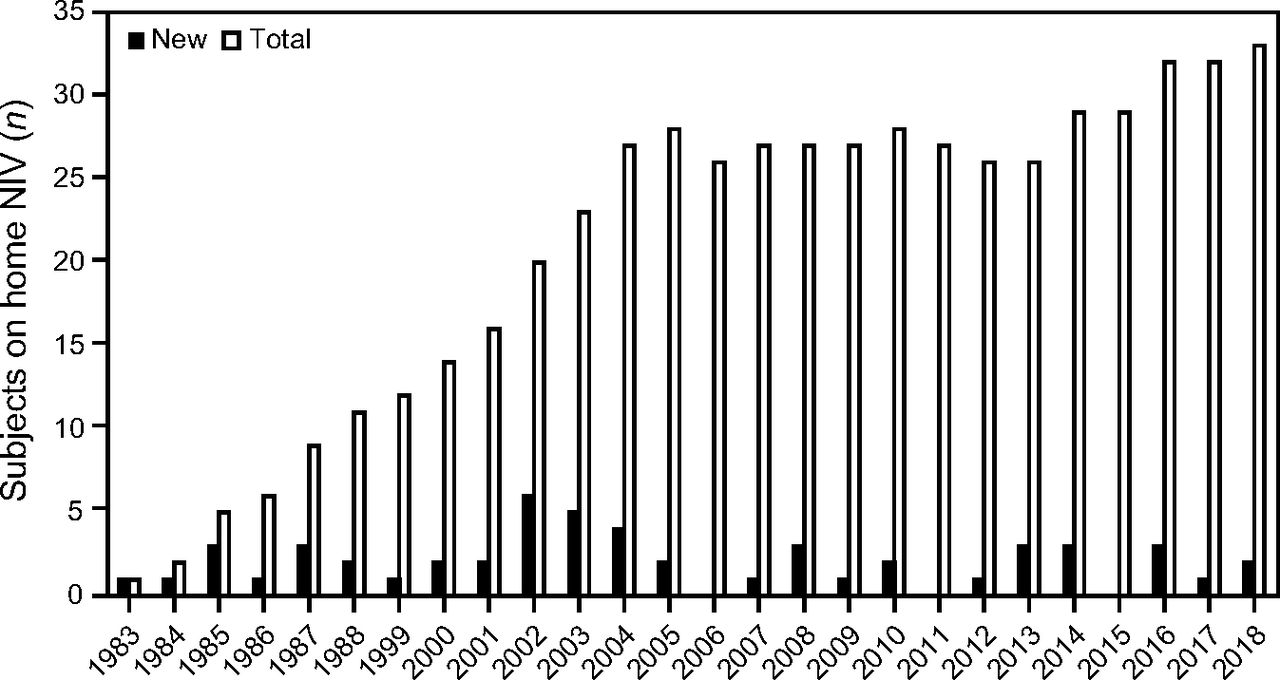
Number of subjects with scoliosis commenced on home noninvasive ventilation (NIV) by year, together with total number of subjects with scoliosis using home NIV each year.
Discussion
The survival rate of our cohort of subjects with thoracic scoliosis on home NIV is slightly better than previous reports.4,8-12,16-23 This may have been the result of our exclusion of patients who were unable to use NIV for > 4 h/d, but it may also reflect improvements in home NIV equipment and service provision.
With the eradication of poliomyelitis, the development of effective antituberculous drugs, and advances in spinal surgery, we had anticipated a decline in the number of patients with scoliosis needing NIV. Our unit services a catchment population of ∼ 1 million for neuromuscular problems,24 perhaps less for obesity-hypoventilation, which is more frequently managed in smaller peripheral units. With regional spinal surgical services on site, we may have seen a higher proportion of patients with scoliosis than would otherwise have been the case. Nevertheless, we suggest that any unit providing home ventilation services should expect to continue to see new referrals with scoliosis.
Poliomyelitis vaccination was introduced in the 1950s. It is unlikely that anyone born after about 1960 will present with respiratory failure as a late complication of polio. While declining numerically, these patients may continue to present with respiratory failure for at least another decade. Their outcomes seem to be the same as those with congenital or idiopathic scoliosis, which argues against there being ongoing neurological damage affecting the respiratory muscles as a late complication of poliomyelitis.25,26
Conclusions
Small numbers of subjects with scoliosis continued to present with respiratory failure. Once established on home NIV, around 40% were still alive 25 years later. Long-term care will be needed for this patient population for many years to come.
Footnotes
- Correspondence: William Kinnear, Erasmus Darwin Building, Clifton Campus, Nottingham Trent University, Nottingham NG11 8NS, UK. E-mail: william.kinnear{at}ntu.ac.uk
An earlier analysis of this cohort was presented at the Journee International de Ventilation a Domicile meeting, held on March 15–17, 2018, in Lyon, France.
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}