

Abstract
BACKGROUND:  may be a reliable noninvasive alternative to the
may be a reliable noninvasive alternative to the  index. Furthermore, the ROX index (ie, the ratio of
index. Furthermore, the ROX index (ie, the ratio of  to breathing frequency) has been validated to predict high-flow nasal cannula failure in subjects under spontaneous breathing. However, these indices have not been tested in subjects with COVID-19 receiving invasive mechanical ventilation. This study aims to verify the correlation between both the ROX index and
to breathing frequency) has been validated to predict high-flow nasal cannula failure in subjects under spontaneous breathing. However, these indices have not been tested in subjects with COVID-19 receiving invasive mechanical ventilation. This study aims to verify the correlation between both the ROX index and  with
with  and the ratio of
and the ratio of  to breathing frequency, and to determine the accuracy of the indices that use
to breathing frequency, and to determine the accuracy of the indices that use  for the prediction of extubation failure in subjects with COVID-19.
for the prediction of extubation failure in subjects with COVID-19.
METHODS: A prospective cohort study was conducted from May 15, 2020, to June 15, 2020, with subjects with COVID-19 on invasive mechanical ventilation. Indices using  in the formula were compared to those using
in the formula were compared to those using  . Additionally, the performance of the indices in predicting extubation failure was evaluated.
. Additionally, the performance of the indices in predicting extubation failure was evaluated.
RESULTS: This study included 69 subjects age 64.8 ± 14.6 y. There were no differences between the median values of the indices, including between the ROX index and  to breathing frequency (P = .40) or between
to breathing frequency (P = .40) or between  and
and  (P = .83). When comparing the ROX index with the
(P = .83). When comparing the ROX index with the  index to breathing frequency, they were found to be strongly correlated (R2 = 0.75 [95% CI 0.6763–0.8152], P < .001). The comparison of
index to breathing frequency, they were found to be strongly correlated (R2 = 0.75 [95% CI 0.6763–0.8152], P < .001). The comparison of  with
with  revealed R2 = 0.70 (95% CI 0.563–0.749, P < .001). The area under the receiver operating characteristic curve for the ROX index to determine extubation failure was 0.74 (P = .01), whereas for
revealed R2 = 0.70 (95% CI 0.563–0.749, P < .001). The area under the receiver operating characteristic curve for the ROX index to determine extubation failure was 0.74 (P = .01), whereas for  it was 0.78 (P < .001).
it was 0.78 (P < .001).
CONCLUSIONS: The indices presented a good correlation in subjects with COVID-19 on invasive mechanical ventilation, and both the ROX index and  can discriminate extubation failure in this population.
can discriminate extubation failure in this population.
Introduction
The use of  is one of the most important methods to evaluate respiratory function and the degree of hypoxia in critically ill subjects.1,2 However, this ratio is obtained through invasive tests, which are not always readily available. A noninvasive substitute for
is one of the most important methods to evaluate respiratory function and the degree of hypoxia in critically ill subjects.1,2 However, this ratio is obtained through invasive tests, which are not always readily available. A noninvasive substitute for  , based on the measurement of
, based on the measurement of  using a pulse oximeter, allows disease severity to be evaluated in patients without arterial blood gas data. Thus,
using a pulse oximeter, allows disease severity to be evaluated in patients without arterial blood gas data. Thus,  has been proposed as a noninvasive substitute for
has been proposed as a noninvasive substitute for  .3-6 When these findings were applied to the ROX index (ie, the ratio of
.3-6 When these findings were applied to the ROX index (ie, the ratio of  to breathing frequency [f]) using high-flow nasal cannula in subjects who had acute respiratory failure, the results showed that
to breathing frequency [f]) using high-flow nasal cannula in subjects who had acute respiratory failure, the results showed that  could represent
could represent  .7,8 However, it remains to be seen whether the use of the ROX index is feasible and reliable in different situations and whether it can be used to predict extubation failure in subjects receiving invasive mechanical ventilation.9,10
.7,8 However, it remains to be seen whether the use of the ROX index is feasible and reliable in different situations and whether it can be used to predict extubation failure in subjects receiving invasive mechanical ventilation.9,10
The aims of this study were to assess whether the ROX index and  could predict extubation failure in subjects receiving invasive mechanical ventilation during the COVID-19 pandemic and to verify the correlations of
could predict extubation failure in subjects receiving invasive mechanical ventilation during the COVID-19 pandemic and to verify the correlations of  and the ROX index with
and the ROX index with  and the ratio of
and the ratio of  to f. These parameters may present as a less invasive substitute for
to f. These parameters may present as a less invasive substitute for  and a reliable oxygenation evaluation method.
and a reliable oxygenation evaluation method.
QUICK LOOK
Current Knowledge
 -based markers present valuable correlations with
-based markers present valuable correlations with  , and the ROX index (ie, the ratio of
, and the ROX index (ie, the ratio of  to breathing frequency) can predict high-flow nasal cannula failure. However, the feasibility of using these indices for the prediction of extubation failure has never been studied.
to breathing frequency) can predict high-flow nasal cannula failure. However, the feasibility of using these indices for the prediction of extubation failure has never been studied.
What This Paper Contributes to Our Knowledge
 -based markers showed a moderate to strong correlation with
-based markers showed a moderate to strong correlation with  -based markers. The ROX index presented similar prediction accuracy for extubation failure and failure of high-flow nasal cannula.
-based markers. The ROX index presented similar prediction accuracy for extubation failure and failure of high-flow nasal cannula.
Methods
This was a prospective, observational, cohort study evaluating adult subjects receiving invasive mechanical ventilation due to respiratory failure from COVID-19 in a tertiary hospital; the Research Ethics Committee approved the study and waived the requirement for informed consent. From May 15, 2020, to June 15, 2020, subjects > 18 y old with COVID-19 who were admitted to the ICU on invasive mechanical ventilation and were in the process of undergoing removal of the ventilator liberation were included. Pregnant women and patients with a previous diagnosis of heart failure were excluded from the study (Fig. 1).

Flow chart.
The primary outcome of the study was the accuracy of the ROX index and  to predict extubation failure in subjects with COVID-19 receiving invasive mechanical ventilation. Secondary outcomes were the presence of correlations of the ROX index and
to predict extubation failure in subjects with COVID-19 receiving invasive mechanical ventilation. Secondary outcomes were the presence of correlations of the ROX index and  with the ratio of
with the ratio of  to f and
to f and  , respectively.
, respectively.
The  values were extracted from routine arterial gas analysis,
values were extracted from routine arterial gas analysis,  data were obtained from a pulse oximeter,
data were obtained from a pulse oximeter,  was determined by the mechanical ventilator, and f was used to obtain the ROX index (ie, the ratio of
was determined by the mechanical ventilator, and f was used to obtain the ROX index (ie, the ratio of  to f), the ratio of
to f), the ratio of  to f,
to f,  , and
, and  after simultaneous serial evaluation of the pulse oximeter and arterial blood gases during the first, third, and seventh day and during the process of extubation. The indices were determined using the worst values of the variables. These indices were compared in the same subjects and at the same time of the day and immediately after the subjects started the process of invasive mechanical ventilation withdrawal.
after simultaneous serial evaluation of the pulse oximeter and arterial blood gases during the first, third, and seventh day and during the process of extubation. The indices were determined using the worst values of the variables. These indices were compared in the same subjects and at the same time of the day and immediately after the subjects started the process of invasive mechanical ventilation withdrawal.
In addition, data from chest computed tomography (CT) scans obtained at the time of admission to the ICU were used, which quantified the degree of involvement of the pulmonary parenchyma. For statistical analysis, the lung parenchyma involvement percentage was dichotomized as higher or lower than 50%.
All subjects were submitted to the extubation process once judged as being ready for extubation, according to the standard institutional protocol (Fig. 2); subjects were considered to have failed extubation if they presented a need for re-intubation within 48 h after extubation, which was defined as the presence of ≥ 2 of the following conditions:  > 0.50, signs of increased work of breathing (eg, tachypnea, use of accessory respiratory muscles, thoracoabdominal paradox) despite noninvasive ventilation support, inability to protect the airway (ie, Glasgow coma scale ≤ 8), upper-airway obstruction, severe respiratory acidosis (
> 0.50, signs of increased work of breathing (eg, tachypnea, use of accessory respiratory muscles, thoracoabdominal paradox) despite noninvasive ventilation support, inability to protect the airway (ie, Glasgow coma scale ≤ 8), upper-airway obstruction, severe respiratory acidosis ( > 50 mm Hg and pH < 7.25), or severe hemodynamic dysfunction (norepinephrine > 0.1 μg/kg/min and rising).
> 50 mm Hg and pH < 7.25), or severe hemodynamic dysfunction (norepinephrine > 0.1 μg/kg/min and rising).

Extubation protocol. PImax = maximum inspiratory pressure; PSV = pressure support ventilation.
Statistical Analysis
Considering the correlation of the ROX index with the success rate of high-flow nasal cannula and considering  with an area under the receiver operating characteristic (ROC) curve of 0.75 in relation to extubation failure, and based on previous studies,7,8,11 a sample of 62 subjects was required to confirm the main hypothesis with a sample power of 80% and a 5% risk for type 1 error.
with an area under the receiver operating characteristic (ROC) curve of 0.75 in relation to extubation failure, and based on previous studies,7,8,11 a sample of 62 subjects was required to confirm the main hypothesis with a sample power of 80% and a 5% risk for type 1 error.
On the basis of these premises, continuous parametric data are expressed as the mean ± SD, whereas nonparametric data are expressed as medians and interquartile ranges (IQR) and were statistically analyzed according to the distribution pattern of the variables. Qualitative data are presented as absolute frequencies and percentages and were compared using the chi-square test.
The Spearman correlation test was performed between the indices and the calculated coefficient of variation of percentages. Correlation values > 0.7 were considered good. Moreover, biases were checked with Bland-Altman analysis. The analysis of repeated measurements was verified using a general linear model (GLM). The consistency of the model was tested using the Mauchly sphericity test. Multivariate analysis of variance was conducted to confirm the final value of P; when the interactions were statistically significant, a Bonferroni post hoc correction was performed.
To assess the accuracy of the methods, sensitivity and specificity tests were performed for the ROX index measured during the extubation process. Thus, a ROC curve with sensitivity and specificity values was plotted, and the point of the maximum value (Youden J index) was defined as a cutoff point to determine extubation failure.
To avoid confounding factors in the interpretation of pulse oximetry values, clinically relevant variables such as hemoglobin, blood pressure, and age were inserted together with  into a multiple regression model. The model was calculated stepwise; interactions were tested, and the model defined the risks and confidence intervals. All tests were 2-tailed, and P values < .05 were considered significant.
into a multiple regression model. The model was calculated stepwise; interactions were tested, and the model defined the risks and confidence intervals. All tests were 2-tailed, and P values < .05 were considered significant.
Results
There were 180 encounters with the 69 subjects included (mean age 64.8 ± 14.6 y, 56.5% male, mean body mass index 28.6 ± 5.5 kg/m2). Hypertension was the most frequent comorbidity (39.4%). The laboratory diagnosis of COVID-19 was confirmed in 87% of the patients, and the remaining cases were treated as suspected of having COVID-19 due to the clinical presentation and suggestive CT findings. In the CT evaluation of the lung, 57.6% of the subjects presented > 50% pulmonary parenchyma involvement. During the evaluation period, 15.3% of the subjects experienced extubation failure, mainly on the third day of invasive mechanical ventilation (Table 1). Regarding the clinical variables during the evaluation period, the subjects had adequate mean blood pressure values, hemoglobin levels > 10 g/dL, no acidemia, and slightly altered arterial lactate (Table 2).
Subject Characteristics
Subject Clinical Characteristics
There were no significant differences in the indices. In general, the median ROX index was 7.8 (IQR 5.4–9.8), and the median ratio of  to f was 7.3 (IQR 5.2–10.2) (P = .40). The median
to f was 7.3 (IQR 5.2–10.2) (P = .40). The median  was 172 (IQR 122–232), and the median
was 172 (IQR 122–232), and the median  was 188 (IQR 119–240) (P = .83). The trends in relation to the days of the index values were very similar for the comparison of
was 188 (IQR 119–240) (P = .83). The trends in relation to the days of the index values were very similar for the comparison of  and
and  (GLM, P = .78) and for the comparison of the
(GLM, P = .78) and for the comparison of the  to f and
to f and  to f (GLM, P = .16) (Fig. 3).
to f (GLM, P = .16) (Fig. 3).

Evolutive comparison of the indices according to the 7 d with connecting lines for the mean and choice of different error bars for the mean (range of 1 SD). A: 7-d comparison between mean values of  and
and  ; (B) 7-d comparison between
; (B) 7-d comparison between  and the ROX index (ie, the ratio of
and the ROX index (ie, the ratio of  to breathing frequency).
to breathing frequency).
When comparing the values of the ROX index with those of the ratio of  to f, we noted a correlation of R2 = .75 (95% CI 0.67–0.82, P < .001). On the other hand, the correlation of
to f, we noted a correlation of R2 = .75 (95% CI 0.67–0.82, P < .001). On the other hand, the correlation of  with
with  was R2 = 0.70 (95% CI 0.56–0.75, P < .001). The highest concentrations were located in the lowest index measurements (Fig. 4).
was R2 = 0.70 (95% CI 0.56–0.75, P < .001). The highest concentrations were located in the lowest index measurements (Fig. 4).

A: Correlation chart between  and
and  , accounting for pulmonary involvement. B: Correlation chart between
, accounting for pulmonary involvement. B: Correlation chart between  and ROX index, accounting for pulmonary involvement. ROX index = ratio of
and ROX index, accounting for pulmonary involvement. ROX index = ratio of  to breathing frequency.
to breathing frequency.
In the evaluation of biases comparing the indices, we found mean biases of 3.85 (95% CI −8.0 to 15.8, P = .52) and 0.008 (95% CI −0.41 to 0.42, P = .97) for  and
and  and for the ratio of
and for the ratio of  to f and the ratio of
to f and the ratio of  to f, respectively (Fig. 5).
to f, respectively (Fig. 5).
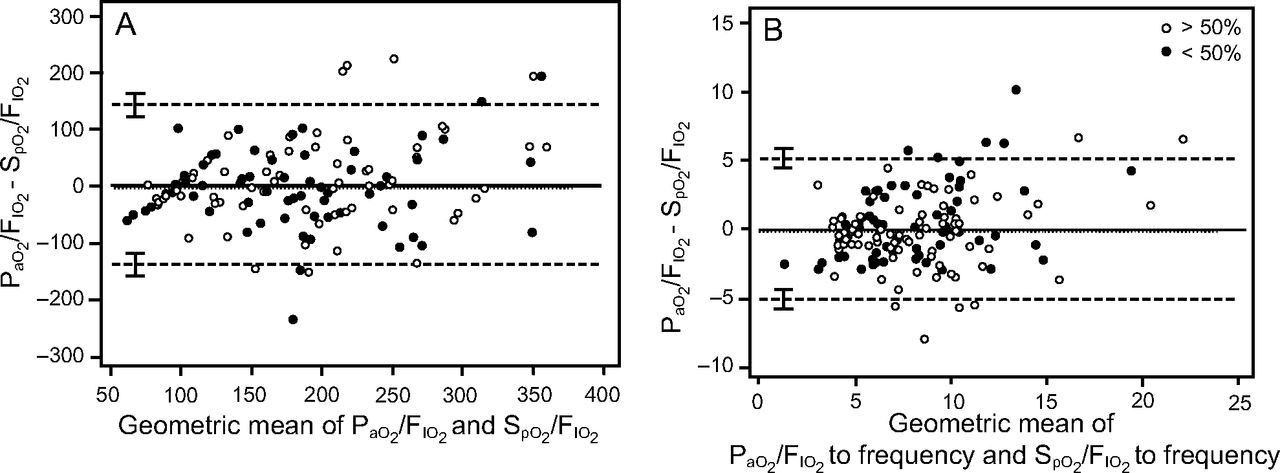
Bland-Altman graph comparing the indices for possible bias. Scatter diagram of the differences plotted against the averages of the measures (A)  and
and  and (B) the ROX index (ie, the ratio of
and (B) the ROX index (ie, the ratio of  to breathing frequency) and the ratio of
to breathing frequency) and the ratio of  to breathing frequency. The displayed horizontal lines represent the mean difference and the upper and lower limits of agreement, defined as the mean difference ± 1.96 SD of differences.
to breathing frequency. The displayed horizontal lines represent the mean difference and the upper and lower limits of agreement, defined as the mean difference ± 1.96 SD of differences.
Thus, considering the ROX index, the area under the ROC to determine extubation failure was 0.74 (P = .01, 95% CI 0.54–0.93, cutoff point ≤ 6.36, sensitivity 67%, specificity 71%). The same finding was identified for  , with an area under the ROC for extubation failure of 0.79 (P < .001, 95% CI 0.62–0.96, cutoff point ≤ 99, sensitivity 67%, specificity 71%) (Fig. 6).
, with an area under the ROC for extubation failure of 0.79 (P < .001, 95% CI 0.62–0.96, cutoff point ≤ 99, sensitivity 67%, specificity 71%) (Fig. 6).

Receiver operating characteristic curve for indices in relation to subjects who failed extubation.
In the evaluation of possible confounding factors that could influence noninvasive indices on the basis of pulse oximetry, we observed that these indices were strong indicators of extubation failure. For  , the odds ratio was 0.948 (95% CI 0.91–0.99); for the ROX index, the odds ratio was 0.45 (95% CI 0.23–0.88) (Table 3).
, the odds ratio was 0.948 (95% CI 0.91–0.99); for the ROX index, the odds ratio was 0.45 (95% CI 0.23–0.88) (Table 3).
Multivariate Analysis of Determinant Factors for Extubation Failure
Discussion
Our results show a good correlation between the noninvasive measures of the ROX index and  and the invasive measures of the ratio of
and the invasive measures of the ratio of  to f and
to f and  , respectively, in subjects receiving invasive mechanical ventilation with suspected or diagnosed COVID-19. The results suggest that the ROX index, as well as
, respectively, in subjects receiving invasive mechanical ventilation with suspected or diagnosed COVID-19. The results suggest that the ROX index, as well as  , can be used in subjects on invasive mechanical ventilation with good accuracy.
, can be used in subjects on invasive mechanical ventilation with good accuracy.
 presents a good correlation with
presents a good correlation with  and allows a dynamic bedside evaluation of the ventilatory weaning process.4,12 We found a positive correlation comparing the 2 proportions with R2 = 0.7 and with a significant linear equation:
and allows a dynamic bedside evaluation of the ventilatory weaning process.4,12 We found a positive correlation comparing the 2 proportions with R2 = 0.7 and with a significant linear equation:  = 51.8 + 0.74 ×
= 51.8 + 0.74 ×  .
.
The ROX index is widely used to predict success in patients receiving noninvasive ventilation.9,10,13-15 Roca et al7 corroborated the correlation between ROX index values ≥ 4.88 and the avoidance of orotracheal intubation for invasive mechanical ventilation in subjects using high-flow nasal cannula and suggested greater importance of  in the ROX index in relation to f. In addition, in subjects with acute respiratory failure due to SARS-CoV-2 on ventilation via high-flow nasal cannula, the ROX index was effective in identifying the need for noninvasive mechanical ventilation.16
in the ROX index in relation to f. In addition, in subjects with acute respiratory failure due to SARS-CoV-2 on ventilation via high-flow nasal cannula, the ROX index was effective in identifying the need for noninvasive mechanical ventilation.16
Previous studies suggest that in subjects undergoing 12 h of high-flow nasal cannula use, ROX index values ≥ 4.88 predict success in the noninvasive management of hypoxemic respiratory failure, with a positive predictive value > 80%, and a ROX index cutoff of ≥ 3.85 provides specificity of 98–99%.9 Other noninvasive predictors, such as f and rapid/shallow breathing index,17 were previously used to assess weaning success, but they did not take into account pulmonary gas exchange performance. In the studied population of subjects with COVID-19 subjects, the values of the ROX index were similar to the index in which  was replaced with
was replaced with  (R2 = 0.75).
(R2 = 0.75).
According to our results, both a ROX index ≤ 6.36 and  ≤ 99 predicted extubation failure, with area under the ROC values of 0.74 and 0.79, respectively. The results were similar to those described in the literature for subjects with hypoxemic respiratory failure from other causes.3,7,8 The results can be of great value for identifying patients with COVID-19 on invasive mechanical ventilation with an increased risk of failed weaning from the ventilatory prosthesis. It is important to highlight that patients with COVID-19 may demand a long duration of mechanical ventilation,18,19 similar to our findings in this study, but the utilization of this index remained valid and exhibited good correlation over time.
≤ 99 predicted extubation failure, with area under the ROC values of 0.74 and 0.79, respectively. The results were similar to those described in the literature for subjects with hypoxemic respiratory failure from other causes.3,7,8 The results can be of great value for identifying patients with COVID-19 on invasive mechanical ventilation with an increased risk of failed weaning from the ventilatory prosthesis. It is important to highlight that patients with COVID-19 may demand a long duration of mechanical ventilation,18,19 similar to our findings in this study, but the utilization of this index remained valid and exhibited good correlation over time.
Lower ROX index values in patients whose pulmonary injury is more severe can be explained by physiological changes related to both the numerator ( ) and the denominator (f) of the index. Patients who are weaning from invasive mechanical ventilation and who have severe lung injury present a more significant loss in alveolar exchange capacity and, consequently, worse oxygenation and reduction in
) and the denominator (f) of the index. Patients who are weaning from invasive mechanical ventilation and who have severe lung injury present a more significant loss in alveolar exchange capacity and, consequently, worse oxygenation and reduction in  . These same patients may also present with increased CO2 production and respiratory muscle fatigue, which are contributing factors to hypoventilation, hypercapnia, and consequently increased f.11
. These same patients may also present with increased CO2 production and respiratory muscle fatigue, which are contributing factors to hypoventilation, hypercapnia, and consequently increased f.11
Notably, the proportion of altered lung parenchyma in the admission CT did not impact the ROX index or  values of subjects with COVID-19, which raises the hypothesis that quantitative lung damage is not representative of the functional impairment caused by the disease. However, this finding can perhaps be explained by the time lapse between the CT examination and the beginning of weaning from invasive ventilation. Figure 3 also corroborates this statement because the mean admission measure of
values of subjects with COVID-19, which raises the hypothesis that quantitative lung damage is not representative of the functional impairment caused by the disease. However, this finding can perhaps be explained by the time lapse between the CT examination and the beginning of weaning from invasive ventilation. Figure 3 also corroborates this statement because the mean admission measure of  was 127.6 ± 6.6, and it improved during the extubation period to 219.8 ± 13.6.
was 127.6 ± 6.6, and it improved during the extubation period to 219.8 ± 13.6.
Additionally, we emphasize that the impaired oxygenation indicated by low  is not exclusively a consequence of pulmonary shunt physiology due to pneumonia or lung injury, but it may also be a consequence of shock due to low mixed venous oxygen concentration or hemoglobin reduction. Thus,
is not exclusively a consequence of pulmonary shunt physiology due to pneumonia or lung injury, but it may also be a consequence of shock due to low mixed venous oxygen concentration or hemoglobin reduction. Thus,  may reflect oxygenation abnormalities originating from shock-related lung and systemic disorders or anemia. These facts could interfere with the results, but our subjects had adequate blood pressure and hemoglobin and perfusion values; in multivariate analysis, the blood pressure and hemoglobin parameters did not interfere with the predictive abilities of
may reflect oxygenation abnormalities originating from shock-related lung and systemic disorders or anemia. These facts could interfere with the results, but our subjects had adequate blood pressure and hemoglobin and perfusion values; in multivariate analysis, the blood pressure and hemoglobin parameters did not interfere with the predictive abilities of  -based indices for extubation failure. Even considering age in the regression model,
-based indices for extubation failure. Even considering age in the regression model,  had an odds ratio of 0.948 (95% CI 0.906–0.991), and the ROX index had an odds ratio of 0.447 (95% CI 0.226–0.882). This corroborates the finding that these noninvasive tools can be used regardless of the possible confounding factors.
had an odds ratio of 0.948 (95% CI 0.906–0.991), and the ROX index had an odds ratio of 0.447 (95% CI 0.226–0.882). This corroborates the finding that these noninvasive tools can be used regardless of the possible confounding factors.
Despite the significant results, this study has limitations, such as being observational, being conducted in a single center, and having a small sample, in addition to not being conducted in a population with worse hemodynamic and oxygenation data because the subjects were in the process of recovery. Nevertheless, the 7-d follow-up showed values of the invasive indices similar to those of noninvasive indices for evaluation of oxygenation exchange in the linear model of repeated measurements (Fig. 3).
Another concern is that several factors related to pulse oximetry values could influence the index measures, such as the site of  measurement, body movement, unreliable oximetry wave, temperature, and the subject’s disease state. Furthermore, pulmonary embolism can influence the clinical management of patients during the extubation period, and pulmonary embolism was not assessed in the study population due to the absence of routine angiotomography for patients with COVID-19. In addition, our results may not be applicable to subjects with lower
measurement, body movement, unreliable oximetry wave, temperature, and the subject’s disease state. Furthermore, pulmonary embolism can influence the clinical management of patients during the extubation period, and pulmonary embolism was not assessed in the study population due to the absence of routine angiotomography for patients with COVID-19. In addition, our results may not be applicable to subjects with lower  because, as reported in the literature,5 nonlinear equations are more accurate than linear models in situations involving hypoxemia. Therefore, a prospective validation of these results with a broad population and subjects with other clinical conditions incorporating such relevant factors for
because, as reported in the literature,5 nonlinear equations are more accurate than linear models in situations involving hypoxemia. Therefore, a prospective validation of these results with a broad population and subjects with other clinical conditions incorporating such relevant factors for  accuracy is indicated.
accuracy is indicated.
Conclusions
 and
and  were well correlated in subjects with COVID-19 receiving invasive mechanical ventilation, and both the ROX index and
were well correlated in subjects with COVID-19 receiving invasive mechanical ventilation, and both the ROX index and  can predict extubation failure in this population. Thus, these tools, using
can predict extubation failure in this population. Thus, these tools, using  instead of
instead of  , can provide a less invasive and reliable oxygenation evaluation method in subjects with COVID-19 who are in the process of extubation.
, can provide a less invasive and reliable oxygenation evaluation method in subjects with COVID-19 who are in the process of extubation.
Footnotes
- Correspondence: João Manoel Silva Jr MD PhD, Anesthesiology Division, Central Institute, University of São Paulo, Faculty of Medicine Clinics Hospital, 05403–000 São Paulo, Brazil. E-mail: joao.s{at}usp.br
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}