

Abstract
BACKGROUND: It is unknown how the initial choice of respiratory support by pediatric ICU providers contributes to outcomes of nonintubated obese children with respiratory failure. We hypothesized that body mass index and the type of initial respiratory support applied are associated with poor clinical outcomes in patients who carry respiratory failure-associated diagnoses.
METHODS: This is a retrospective analysis of de-identified patient data obtained from the Virtual PICU System database (2009–2018). We included subjects 2–18 y old who received bi-level positive airway pressure/CPAP or high-flow nasal cannula as the initial respiratory support and were assigned respiratory failure-associated diagnoses (ie, acute hypoxic respiratory failure). The study population was divided into 2 body mass index percentile groups, underweight/healthy weight (< 85th percentile) and overweight/obese (≥ 85th percentile), and subjects were evaluated for the following outcomes: endotracheal intubation requirement, medical and physical PICU length of stay, and mortality scores.
RESULTS: A total of 1,721 subjects were included: 1,091 (63.4%) underweight/healthy weight and 630 (36.6%) overweight/obese. Body mass index percentile was not associated with the initial respiratory support utilized (odds ratio 0.961 [95% CI 0.79–1.17], P = .73). Multivariable logistic regression analysis demonstrated that the odds of requiring endotracheal intubation (odds ratio 1.60 [95% CI 1.10–2.35], P = .02) were significantly higher in overweight/obese subjects initially placed on high-flow nasal cannula. Body mass index and bi-level positive airway pressure/CPAP therapy were both positively associated with medical and physical PICU length of stay, Pediatric Risk of Mortality Score 3 (PRISM3) scores, and Pediatric Index of Mortality 2 (PIM2) scores when separate multivariable models were fit for these 4 response variables.
CONCLUSIONS: The selection of respiratory support may place overweight/obese pediatric patients at higher risk for endotracheal intubation. Due to methodological limitations, we were unable to draw conclusions about the initial approach to the respiratory management of overweight/obese pediatric patients. Further investigation may be warranted.
- pediatrics
- obesity
- acute respiratory failure
- bilevel invasive respiratory support
- high flow nasal cannula
Introduction
Childhood and adolescent obesity are significant health concerns throughout the world. It is associated with adverse health outcomes, including hypertension, hyperlipidemia, metabolic syndrome, type II diabetes, sleep apnea, asthma, and fatty liver disease, as well as a long-term increased likelihood of morbidity and mortality.1,2
In the United States, the prevalence of pediatric obesity has been increasing,3 and critically ill obese children have an increased overall mortality risk.4 For obese children with respiratory failure, the mortality risk is similar to normal-weight children, but it is associated with a significant increase in the use of noninvasive as well as invasive mechanical ventilation and longer duration of invasive mechanical ventilation in indirect lung injury ARDS.5-7
Obese children with respiratory failure require special consideration, as they have a variety of altered respiratory mechanics and comorbidities.8-10 Therefore, it stands to reason that the initial approach to respiratory support should be focused on understanding the factors that have an impact on the outcomes of obese pediatric patients with respiratory failure. It is unknown, however, whether the clinician’s initial approach to the management of respiratory failure is a contributing factor to overall clinical outcomes. It is also unknown whether the use of noninvasive positive pressure therapy, such as bi-level positive airway pressure (BPAP)/CPAP and high-flow nasal cannula (HFNC), is beneficial in this group. By evaluating the outcomes associated with initial respiratory support in obese pediatric patients with respiratory failure, physicians may be able to provide better care to this population.
The objective of this study is to analyze data from the multi-institutional Virtual PICU Systems database (VPS LLC, Los Angeles, California) to determine the outcomes of pediatric subjects with an elevated body mass index (BMI) who received non-invasive respiratory support (BPAP/CPAP or HFNC) as an initial mode of respiratory support for respiratory failure-associated VPS Star diagnostic codes. We hypothesized that, for overweight/obese subjects diagnosed with acute hypoxemic respiratory failure, the type of initial respiratory support applied is associated with increased mortality, longer ICU length of stay, increased duration of HFNC or BPAP/CPAP, and the need for endotracheal intubation.
QUICK LOOK
Current Knowledge
Childhood and adolescent obesity are significant health concerns throughout the world. Obese children with respiratory failure require special consideration, as they have altered respiratory mechanics and comorbidities.
What This Paper Contributes to Our Knowledge
Body mass index was not associated with time on bi-level positive airway pressure/continuous airway pressure (BPAP/CPAP) or high-flow nasal cannula (HFNC). Overweight/obese subjects initially placed on HFNC had an increased odds of endotracheal intubation, and overweight/obese subjects initially placed on BPAP/CPAP were associated with higher mortality scores as well as an increased PICU length of stay. These results may have implications for the approach to the initial respiratory management of overweight/obese patients admitted for acute respiratory failure in the pediatric ICU.
Methods
Data Source
Data for this study were obtained from the Virtual PICU Systems (VPS) database, a prospectively collected web-based research database developed by an online pediatric critical care network formed by the Children’s Hospital Association and Children’s Hospital Los Angeles.11 It is a prospective observational cohort of consecutive pediatric ICU (PICU) admissions from a variety of hospitals caring for children across the United States, where the data were collected and entered by trained individuals. The institutional review board at Penn State College of Medicine categorized this study as non-human research because the data involved the analysis of de-identified patient information.
Patient Population
Using this data source, de-identified data were obtained from the VPS database for subjects 2–18 y old who were unscheduled admissions receiving HFNC or BPAP/CPAP for their initial respiratory support from January 1, 2009, through December 1, 2018. The initial study population included 3,780 PICU admissions from 142 hospitals. Diagnostic and procedure codes were used to identify the included cohort. Unscheduled PICU admission subjects were included in this study if they were between the ages of 2 and 18 y; were determined to have any one of the following VPS Star code diagnoses: (1) pulmonary insufficiency/shock lung, adult respiratory distress syndrome, acute hypoxic respiratory failure, acute lung injury (ie, VPS Star Codes 518.84, 518.81, 518.83, 518.5, 518.82); (2) dyspnea/tachypnea, respiratory distress/insufficiency, respiratory distress (ie, VPS Star Codes 786.06, 786.01, 786.09, 786.00, 786.05, 786.02); and (3) asphyxia (not birth or trauma), hypoxemia, and hypoxia (ie, VPS Star Codes 799.02, 799.01, 799.0); and were initially placed on non-invasive respiratory support (HFNC or BPAP/CPAP) as the initial respiratory treatment strategy. Subjects who received BPAP and CPAP were placed in the same group due to the low quantity of subjects placed on CPAP first.
The following patients were excluded from the study: < 2 y old, > 18 y old, encounters lacking height data, encounters that triggered a height or weight error during BMI calculation, patients who were not initiated on HFNC, BPAP, or CPAP upon admission, patients who were started on 2 different forms of respiratory support (HFNC, BPAP, or CPAP upon admission), or patients who had a tracheostomy in place on admission.
Data Collection
Demographic data (age, gender, and anthropometric data including height and weight) and clinical data (primary diagnosis, secondary diagnosis, PICU mortality, Pediatric Index of Mortality 2 [PIM2] scores, Pediatric Risk of Mortality Score 3 [PRISM3]), procedure codes, the start and end time of each procedure code, length of PICU medical stay (time spent in the PICU until medically discharged from PICU services), and length of PICU physical stay (time spent in the PICU until physically discharged) were collected. The procedure codes were used to determine the proportion and duration of subjects requiring HFNC, BPAP/CPAP, and endotracheal intubation. Due to the limitations of the database, we were unable to determine the HFNC or BPAP/CPAP settings and the reasoning behind the interventions applied.
Once the data were collected, BMI percentiles were calculated using the Centers for Disease Control and Prevention’s online information: “Children’s BMI Tool for Schools.” (https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/tool_for_schools.html Accessed April 6, 2021). The cohort was then determined by splitting the subject population into 2 groups: underweight/healthy weight group defined as having a BMI percentile < 85%, and overweight/obese group characterized as having a BMI percentile ≥ 85%.12
Statistical Analysis
Summary statistics were computed for quantitative variables (eg, means and standard deviations) and categorical variables (eg, counts and proportions). Contingency tables, odds ratios, and chi-square tests were used to explore associations between pairs of binary variables of interest. Negative binomial regression was applied to explore the association between PRISM3 scores and BMI while controlling for respiratory therapy (HFNC or BPAP) after goodness-of-fit testing suggested that Poisson regression was not appropriate. Because linear model diagnostics suggested that the necessary model assumptions were not satisfied, a robust linear modeling approach based on bootstrap resampling was utilized to fit linear models to investigate the association between log-transformed values of the response variables of length of medical stay, length of physical stay, and BMI while controlling for respiratory therapy. Briefly, linear models were fit and the regression coefficients were recorded based on 10,000 bootstrap samples. The empirical covariance matrix of the bootstrap regression coefficients was then computed, and this was used to perform separate Wald tests for each of the explanatory variables based on the appropriate contrast matrices. Multivariable logistic regression models were used to explore the association between endotracheal intubation and obesity after controlling for PIM2 scores and age. These models were fit separately after restricting to subjects who received either HFNC or BPAP. Hosmer-Lemeshow tests were applied to assess goodness of fit for the logistic regression models. The Spearman correlation coefficient was used to assess the association between respiratory therapy time and BMI. R 3.6.3 (R Core Team) was used to perform all statistical analyses.13
Results
Overview
A total of 3,780 patient encounters were provided. Patient encounters were excluded if anthropometric data lacking height (n = 1,663), height or weight error was triggered during BMI percentile calculation (n = 75), if the encounter was a scheduled admission (n = 48), if the patient was not initiated on HFNC, BPAP, or CPAP upon admission (n = 268), or if the patient was placed on 2 different forms of respiratory support upon admission (n = 5). Following exclusion criteria, the study population totaled 1,721 subjects.
Subject Demographics
The non-overweight/obese (< 85%) group consisted of 1,091 (63.4%) subjects, while 630 subjects (36.6%) comprised the overweight/obese (≥ 85%) group. Baseline demographic data were similar in both groups, including age, height, race, subject origin, outcome, limitation of care, withdrawal of support, critical care role in the management of these subjects, length of PICU medical stay, length of PICU physical stay, PIM2 and PRISM3 scores, and overall mortality. Mean weight, BMI, and BMI percentiles were within the ranges expected for each group (Table 1).
Demographics
Initial Respiratory Support Utilized
Subject body type was not associated with the initial respiratory support utilized (odds ratio 0.961 [95% CI 0.79–1.17], P = .73). Of the study population, 915 (53.2%) subjects were placed on BPAP/CPAP, and 806 (46.8%) were placed on HFNC oxygen as their initial respiratory therapy. Of the overweight/obese subjects, 331 (52.5%) were initially placed on BPAP/CPAP, and 299 (47.4%) were placed on HFNC as the initial mode of respiratory support upon admission to the PICU. Of the underweight/healthy weight subjects, 584 (53.5%) were placed on BPAP/CPAP, and 507 (46.5%) were placed on HFNC as the initial mode of respiratory support. There was no statistically significant association noted between BMI and time spent on HFNC (Spearman r = –0.036, P = .31) or BPAP/CPAP (Spearman r = –0.05, P = .13).
Association of Body Type With Endotracheal Intubation
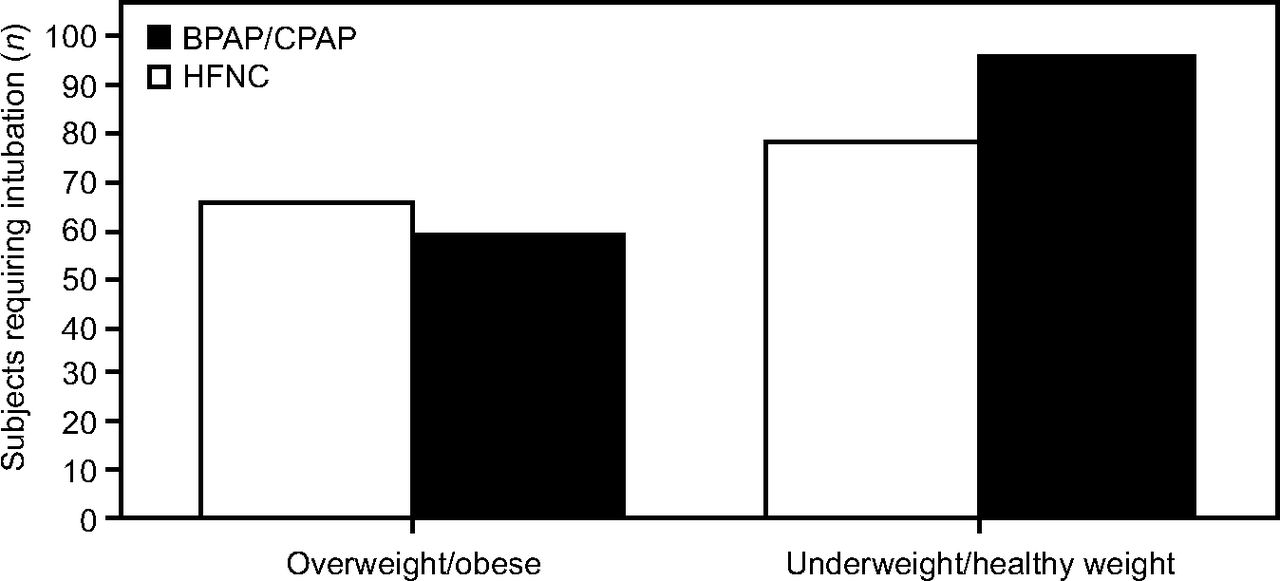
A total of 302 (17.5%) subjects required endotracheal intubation. Of the HFNC group, 66 (10.5%) overweight/obese subjects required endotracheal intubation versus 79 (7.2%) in the non-overweight group. For subjects placed initially on BPAP/CPAP, 60 (9.5%) overweight/obese subjects required endotracheal intubation compared to 97 (8.9%) in the non-overweight group (Figure 1).

Subjects initially placed on high-flow nasal cannula (HFNC) or bi-level positive airway pressure (BPAP)/CPAP on admission requiring endotracheal intubation.
For subjects who initially received HFNC, obese subjects had significantly increased odds of requiring endotracheal intubation (odds ratio 1.53 [95% CI 1.07–2.21], P = .026). In contrast, for subjects who were originally treated with BPAP/CPAP, obesity was not associated with endotracheal intubation. Similar findings were observed after fitting multivariable logistic regression models. For subjects who initially received HFNC as their respiratory support, those who were obese had significantly increased odds of requiring endotracheal intubation (odds ratio 1.61 [95% CI 1.10–2.35], P = .01) after controlling for age and PIM2 scores. The associations between obesity and endotracheal intubation were not statistically significant for subjects who were originally treated with BPAP/CPAP (odds ratio 1.12 [95% CI 0.78–1.59], P = .55), again after controlling for age and PIM2 scores. Age for all groups and the PIM2 in the BPAP group were not significant factors for endotracheal intubation in multivariable models (Table 2).
Univariate and Multivariate Analysis for Type of Noninvasive Respiratory Support and Association With Endotracheal Intubation
Hosmer-Lemeshow goodness-of-fit tests suggested potential issues with model fit when applied to the multivariable logistic regression model for endotracheal intubation with the BPAP/CPAP group. For this reason, a more complex model was fit that included interaction terms between overweight/obesity and age as well as overweight/obesity and PIM2. No issues with goodness of fit were identified in the more complex model. As observed earlier, the association between obesity/overweight and endotracheal intubation was not statistically significant (odds ratio 1.49 [95% CI 0.35–6.27], P = .59; see the supplementary materials at http://www.rcjournal.com). When the likelihood ratio test was applied to perform model selection, the results indicated that the more parsimonious model without the interaction terms was preferred (likelihood ratio test P > .05).
Association of Mortality Scores With BMI and BPAP/CPAP Usage
Subjects requiring BPAP/CPAP usage as the initial respiratory support and subjects with elevated BMI were significantly associated with higher PRISM3 scores (Table 3). Subjects placed on BPAP had a significantly higher PIM2 score, and this association was seen regardless of body type (Table 4).
Negative Binomial Regression Analysis for PRISM3 Scores and Association With BMI and BPAP/CPAP Usage
PIM2 Scores and Association With BMI and HFNC or BPAP/CPAP Usage
Association of Length of Stay With BPAP/CPAP Usage and BMI
Utilizing HFNC as the reference state, increasing BMI and BPAP/CPAP usage were significantly associated with longer medical stay and physical PICU stay. These groups included subjects who received endotracheal intubation (Table 5).
Bootstrap Analysis Between Length of Stay and BPAP/CPAP Usage and BMI
Discussion
We hypothesized that, for overweight/obese subjects diagnosed with acute hypoxemic or hypercapnic respiratory failure, the type of initial respiratory support provided (ie, BPAP/CPAP or HFNC) is associated with poor clinical outcomes. The main findings of this study were that BMI is not associated with time on BPAP/CPAP or HFNC; overweight/obese subjects initially placed on HFNC have an increased odds of endotracheal intubation, and overweight/obese subjects initially placed on BPAP/CPAP are associated with an increased length of medical and physical length of PICU stay. These results may have implications on the approach to the initial respiratory management of overweight/obese patients admitted for acute respiratory failure in the PICU.
Noninvasive forms of respiratory support such as BPAP/CPAP and HFNC have been used increasingly for pediatric respiratory failure.14,15 Both BPAP/CPAP and HFNC facilitate respiratory distress resolution and can reduce the need for invasive mechanical ventilation.16-21 When both of these modes are compared, HFNC appears to be non-inferior to BPAP/CPAP in certain clinical conditions.18 Obese children, however, have special considerations that may need to be assessed before the selection of respiratory support. They have reduced chest wall compliance, often have restrictive and obstructive lung disease, and are at increased risk of atelectasis.22 While HFNC may prevent airway collapse and avoid decreases in functional residual capacity and anatomical dead space depending on the settings utilized, the data supporting its use in this subject population are limited.23 Focusing on the approach to initial respiratory management and the clinical decision-making process may be a novel way to improve patient outcomes and may potentially highlight new areas of research to improve the morbidities associated with overweight and obese pediatric patients who are experiencing respiratory failure.
In this study, we investigated whether there is a difference in outcomes depending on the initial respiratory therapy selected for the obese population. We found that the odds of requiring endotracheal intubation were significantly higher in overweight/obese subjects placed on HFNC compared to those initially placed on BPAP/CPAP. These findings may indicate that BPAP/CPAP should be favored as the initial form of respiratory support in overweight/obese patients. HFNC provides humidified gas through a nasal cannula interface, allows more precise oxygen delivery by decreasing the amount of room air entrainment, and increases functional residual capacity.24,25 The pressure applied by HFNC is variable depending on whether the patient is breathing with the mouth open or closed, and HFNC may not be able to provide sufficient PEEP in patients with severe lung disease (ie, ARDS).26 These are important factors, considering that obese patients’ underlying respiratory physiology may require more PEEP to not only address the patient’s underlying lung disease but abdominal competition.
Even though obese children with respiratory failure who initially received BPAP/CPAP for support were not associated with intubation, increasing BMI and BPAP/CPAP usage were significantly associated with greater length of medical and physical PICU length of stay and higher PRISM3 scores. This implies that patients who have an elevated BMI and are initially placed on BPAP/CPAP therapy have a higher severity of illness, may be at higher risk of complications related to acute illness, and may have a prolonged recovery period.27 Alternatively, these findings may indicate that a different respiratory strategy needs to be considered. Endotracheal intubation, for instance, may offer benefits in this patient population, such as the unloading of ventilatory muscles decreasing systemic or myocardial oxygen consumption and allowing for suctioning of secretions.28,29 Due to the limitations of this study, additional study is warranted to investigate the optimal approach to respiratory illness for overweight and obese patients and whether the benefits associated with invasive mechanical ventilation outweigh the risks.30
Limitations
This study has several limitations. We were limited to the variables collected and present within the VPS database. The VPS database does not account for patients who utilize home CPAP/BPAP. Because the VPS database does not record the flow for patients initially placed on HFNC, it is unknown whether the set flow exceeded the patient’s inspiratory flow and minimized room air entrainment or its PEEP effect. Device settings for BPAP or CPAP were not available, so we were unable to determine whether intubation in this study population was due to progressive respiratory failure or the settings initially selected. Due to lack of arterial access (and/or arterial blood sampling) on admission for a significant number of subjects, variables such as  in arterial blood, the
in arterial blood, the  in arterial blood, and
in arterial blood, and  were not available. Without these variables, we were limited in our ability to determine whether the differences we observed between the 2 groups were due to differences in BMI or in the severity of respiratory failure. The presence of other medical comorbidities (ie, asthma, obstructive sleep apnea) as well as the pathologies that lead to acute respiratory failure were not assessed, limiting our ability to control for these factors in multivariate analyses. An evaluation of significantly obese children (BMI > 99th percentile or Z score > 2.3) was considered. Due to a small population of subjects, however, we opted not to evaluate this subset of patients. As more data are collected on critically ill obese children, it may be possible to examine this population more closely in the future. Due to the retrospective, multi-institutional nature of this study and the limitations of the database, we could not consider the different clinical approaches, types of equipment, escalation of care in subjects with progressive respiratory failure, and regional PICU practices in this analysis.
were not available. Without these variables, we were limited in our ability to determine whether the differences we observed between the 2 groups were due to differences in BMI or in the severity of respiratory failure. The presence of other medical comorbidities (ie, asthma, obstructive sleep apnea) as well as the pathologies that lead to acute respiratory failure were not assessed, limiting our ability to control for these factors in multivariate analyses. An evaluation of significantly obese children (BMI > 99th percentile or Z score > 2.3) was considered. Due to a small population of subjects, however, we opted not to evaluate this subset of patients. As more data are collected on critically ill obese children, it may be possible to examine this population more closely in the future. Due to the retrospective, multi-institutional nature of this study and the limitations of the database, we could not consider the different clinical approaches, types of equipment, escalation of care in subjects with progressive respiratory failure, and regional PICU practices in this analysis.
Conclusions
The selection of respiratory support may place overweight/obese pediatric patients at higher risk for endotracheal intubation, but it may also result in a decreased length of PICU stay. Due to methodological limitations, we are unable to draw conclusions about the initial approach to the respiratory management of overweight/obese pediatric patients. Further investigation may be warranted.
ACKNOWLEDGMENTS
The authors thank VPS, LLC for providing the data.
Footnotes
- Correspondence: Conrad Krawiec MD, Penn State Hershey Children’s Hospital, Department of Pediatrics, 500 University Drive, PO Box 850, Hershey, PA 17033–0850. E-mail: ckrawiec{at}pennstatehealth.psu.edu
Supplementary material related to this paper is available at http://www.rcjournal.com.
This work was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1 TR002014. The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises









{kind=link}