

Abstract
BACKGROUND: Post–COVID-19 syndrome has affected millions of people, with rehabilitation being at the center of non-pharmacologic care. However, numerous published studies show conflicting results due to, among other factors, considerable variation in subject characteristics. Currently, the effects of age, sex, time of implementation, and prior disease severity on the outcomes of a supervised rehabilitation program after COVID-19 remain unknown.
METHODS: This was a non-randomized case-control study. Subjects with post–COVID-19 sequelae were enrolled. Among study participants, those who could attend an 8-week, supervised rehabilitation program composed the intervention group, whereas those who couldn’t the control group. Measurements were collected at baseline and 8 weeks thereafter.
RESULTS: Study groups (N = 119) had similar baseline measurements. Participation in rehabilitation (n = 47) was associated with clinically important improvements in the 6-min walk test (6MWT) distance, adjusted (for potential confounders) odds ratio (AOR) 4.56 (95% CI 1.95–10.66); 1-min sit-to-stand test, AOR 4.64 (1.88-11.48); Short Physical Performance Battery, AOR 7.93 (2.82–22.26); health-related quality of life (HRQOL) 5-level EuroQol-5D (Visual Analog Scale), AOR 3.12 (1.37–7.08); Montreal Cognitive Assessment, AOR 6.25 (2.16–18.04); International Physical Activity Questionnaire, AOR 3.63 (1.53–8.59); Fatigue Severity Scale, AOR 4.07 (1.51–10.98); Chalder Fatigue Scale (bimodal score), AOR 3.33 (1.45–7.67); Modified Medical Research Council dyspnea scale (mMRC), AOR 4.43 (1.83–10.74); Post–COVID-19 Functional Scale (PCFS), AOR 3.46 (1.51–7.95); and COPD Assessment Test, AOR 7.40 (2.92–18.75). Time from disease onset was marginally associated only with 6MWT distance, AOR 0.99 (0.99–1.00). Prior hospitalization was associated with clinically important improvements in the mMRC dyspnea scale, AOR 3.50 (1.06–11.51); and PCFS, AOR 3.42 (1.16–10.06). Age, sex, and ICU admission were not associated with the results of any of the aforementioned tests/grading scales.
CONCLUSIONS: In this non-randomized, case-control study, post–COVID-19 rehabilitation was associated with improvements in physical function, activity, HRQOL, respiratory symptoms, fatigue, and cognitive impairment. These associations were observed independently of timing of rehabilitation, age, sex, prior hospitalization, and ICU admission.
- post–COVID-19 syndrome
- 6-min walk test (6MWT)
- pulmonary rehabilitation
- physical function
- respiratory symptoms
- fatigue
- mental health
- health-related quality of life (HRQOL)
Introduction
Post–COVID-19 sequelae are emerging as a new public health issue, with more than 65 million people affected worldwide. More than 200 symptoms have been recorded, with multiple organ systems affected, thereby frequently resulting in functional capacity impairment, fatigue, mental health issues, respiratory symptoms, and poor health-related quality of life (HRQOL).1 Emerging evidence places rehabilitation at the heart of non-pharmacologic interventions that improve multiple parameters of post–COVID-19 sequelae.2,-,4 However, the numerous studies that have been published are characterized by heterogeneity and increased risk of bias due to differences in rehabilitation programs, study design elements, and diversity of subject populations.3
A certain degree of natural recovery in post–COVID-19 sequelae has been noticed early in the pandemic.5 Consequently, the outcome measurements of patients participating in rehabilitation during or immediately after hospitalization6,7 may differ from patients recruited weeks or months after discharge,8 due to the effect of natural recovery. Prior disease severity may impact outcome measurements as well. Critical illness is associated with an increased risk of subsequent post–COVID-19 complications1 in addition to more severe post-discharge health impairments, thus providing the potential for greater improvements.7 Disease severity, middle age, and female sex have also been linked to poor recovery after COVID-19.9,10 A recent review and meta-analysis highlighted significant improvement in functional status in elderly subjects after rehabilitation.11
Despite heterogeneity of the studies, physical function, mental health, HRQOL,3 and respiratory symptoms are consistently the outcomes with moderate-to-large improvements.2 However, with few exceptions, rehabilitation studies lack outcome control for confounding factors.3 The aim of the present study was to investigate whether the implementation of a supervised rehabilitation program in a mixed population of post COVID-19 patients with varying degrees of prior disease severity, time of rehabilitation intervention in relation to the onset of symptoms of COVID-19, age and sex were associated with potential improvements in post COVID-19 symptoms/sequelae.
QUICK LOOK
Current knowledge
Rehabilitation services have been suggested to ameliorate post–COVID-19 sequelae, including decline in physical fitness, impairments in mental health and health-related quality of life (HRQOL), as well as respiratory symptoms. However, the possible importance of various confounding factors, including patient demographics and prior disease severity, remains unexplored.
What this paper contributes to our knowledge
Rehabilitation was associated with improvements in physical function, HRQOL, respiratory symptoms, fatigue, and cognitive impairment post COVID-19. These associations were independent of, age, sex, timing of rehabilitation, prior hospitalization, and ICU admission.
Methods
This was a prospective, non-randomized case-control study conducted from June 2022–September 2023. Early in the pandemic our center designed and implemented a supervised rehabilitation program for patients suffering from persistent post–COVID-19 symptoms. The program structure was based on the guidelines for post–COVID-19 rehabilitation issued by the American Thoracic Society (ATS), European Respiratory Society (ERS), and the British Thoracic Society (BTS)12,13 and was subsequently adopted by the Hellenic Thoracic Society.14 At the beginning of the pandemic, the patients recovering from severe COVID-19 pneumonia were given priority since they needed supported recovery.9 Our rehabilitation program has been associated with improvements in physical function and symptoms.8 However, as the pandemic progressed, so did the number of patients with post–COVID-19 symptoms who recovered after mild illness at home.1 Consequently, rehabilitation services were made available to all symptomatic patients who were referred to the Long COVID day clinic of our hospital, irrespective of previous hospitalization (for COVID-19). Subjects who were able to attend our 8-week supervised program composed the intervention (rehab) group, whereas those who could not (eg, due to transportation issues along with professional or other competing obligations) the control group. Subject evaluation was conducted at study enrollment (baseline) and after 8 weeks of either rehabilitation or usual care (control). Following their first visit to our clinic, all study participants signed an informed consent form to participate in the study, according to the protocol approved by the Scientific Council of Evangelismos General Hospital, Athens, Greece (approval number 09–06-2022/188).
Participants
Inclusion criteria.
Patients > 18 y of age who suffered from persistent symptoms after COVID-19 infection confirmed by real-time polymerase chain reaction (PCR) were eligible for enrollment. Patients with prior hospitalization had to have persistent symptoms for > 8 weeks after hospital discharge, and patients with mild disease had to have persistent symptoms for at least 12 weeks from disease onset to become eligible for enrollment.12,13,15
Exclusion criteria.
Patients who were not ambulatory, chronically paralyzed, with paraplegia, multiple injuries or other serious orthopedic problems that caused disability, and those suffering from dementia or very serious underlying diseases such as end-stage cancer were excluded. Patients treated for COVID-19 infection while being hospitalized for another reason (eg, coronary heart disease, elective surgery) and patients with active disease were also excluded.13
Measurements and Clinically Relevant Thresholds
Subject improvement was assessed with tests that measured physical function, symptoms, HRQOL, and mental health. Thresholds of impairment or improvement were pre-specified for each test. Thresholds of impairment were cutoff score points indicating impairment (eg, COPD Assessment Test [CAT] score ≥ 10). Τhe below-defined minimum clinically important difference was used to define an improvement threshold. Subject clinical status was considered as improved when a test’s improvement threshold was exceeded at 8 weeks post enrollment. In tests with thresholds of impairment, subjects with normal baseline measurements that remained unchanged or deteriorated were considered as not improved.
Physical function was evaluated with the 6-min walk test (6MWT), the Short Physical Performance Battery (SPPB), the 1-min sit-to-stand test (STS), and the Activities-Specific Balance Confidence (ABC) Scale. Physical activity was evaluated with the International Physical Activity Questionnaire-Short Form (IPAQ-SF). The 6MWT is the most widely used exercise field test for assessing functional exercise capacity, and a walking distance improvement threshold of 30 m is established for patients with chronic respiratory disease.16 A minimum clinically important difference for patients with Long COVID has not been established, however, given the younger age, the fewer comorbidities, and the spontaneous improvement;8 therefore, we adopted a more conservative threshold of 50 m.17 The SPPB is an established test for measuring physical performance, with a threshold of functional impairment of ≤ 10 points.9 The 1-min STS is an easy-to-perform test of lower muscle strength and endurance that measures the number of times a person can sit down and stand up on a chair in 1 min. A minimum clinically important difference after rehab of 3 repetitions was specified.18 The IPAQ-SF is a 7-item questionnaire exploring the frequency and the duration of physical activity performed in the last 7 d and estimating energy expenditure/week. Low physical activity profile corresponds to a total physical activity score of < 600 metabolic equivalent of task (MET) min/week; accordingly, the threshold for functional impairment was set at 600 MET min/week.19
Respiratory symptoms were assessed with the CAT and the Modified Medical Research Council (mMRC) dyspnea scale. Fatigue was assessed with 3 questionnaires covering short- and long-term impact or change. The Functional Assessment of Chronic Illness Therapy (FACIT), the Fatigue Severity Scale (FSS), and the Chalder Fatigue Scale (CFQ) were used to assess fatigue in the last 7 d, 2 weeks, and 1 month, respectively. General post–COVID-19 functional status was assessed with the Post–COVID Functional Scale (PCFS). The CAT, an 8-item questionnaire that was initially developed to assess COPD symptoms and qualify health status impairment,20 was used to assess rehabilitation outcomes in post–COVID-19 patients early in the pandemic.21 A score of ≥ 10 indicates increased symptoms and is used as a threshold for treatment.22 The mMRC scale is a 4-point scale based on the sensation of dyspnea during a patient’s daily activities, with a cutoff point of ≥ 2 used as a commonly accepted threshold of breathlessness.22 The FSS consists of 9 questions designed to assess the severity of fatigue symptoms. A scoring threshold of ≥ 36 may suggest severe fatigue or the need for further assessment.23 The CFQ is a self-report questionnaire for measuring the extent and severity of tiredness and fatigue within both clinical and non-clinical, epidemiological populations. The bimodal score (CFQ-bim) is used to assess the number of symptoms, with a threshold of ≥ 4 indicating severe fatigue.24 For evaluating post–COVID-19 functional status, we used the PCFS, which correlates with quality of life, dyspnea, and mental health. A score of ≥ 2 on this scale indicates impairment in daily life.25
Mental health was assessed with the Hospital Anxiety and Depression Scale (HADS), the Beck Depression Inventory (BDI), and the Impact of Event Scale - Revised (IES-R) for depression, anxiety, and posttraumatic stress disorder evaluation, respectively. The Montreal Cognitive Assessment (MoCA) was used as a brief screening tool for detecting mild cognitive impairment in subjects with a score of ≤ 25.26
HRQOL was evaluated using the 5-level EuroQol-5D (EQ-5D-5L) and the 36-Item Short Form Health Survey (SF-36) questionnaire. The EQ-5D-5L assesses HRQOL using a utility index (UI) and an EQ Visual Analog Scale (EQ-VAS). The minimum clinically important difference of the UI and EQ-VAS was set to 0.051 and 6.9, respectively.27 The SF-36 is a widely used instrument for assessing HRQOL, measuring 8 scales that represent physical and mental dimensions (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health). A score of 50 is considered normative for all scales and represents average health.28 The ABC scale, FACIT, BDI, IES-R, and SF-36 are described in the supplementary material (see related supplementary materials at http://www.rcjournal.com).
Rehabilitation Program
The program was multidisciplinary, including supervised interval aerobic and resistance training, education, physiotherapy, dietary advice, and psychological support twice a week for 8 weeks. Subjects assigned to the rehabilitation group performed a maximum incremental test on an electromagnetically braked cycle ergometer (Ironman M3, Key Fitness Products, Garland, Texas) to determine the peak work rate (WRpeak). The procedure included 3 min of rest measurements, 3 min of unloaded pedaling, followed by an increase in work rate every minute by 5–20 W to the limit of tolerance, while subjects maintained a pedaling frequency of 60 RPM. Heart rate and SpO2 were determined using a pulse oximeter (Onyx, Nonin Medical, Plymouth, Minnesota) as well as symptoms of dyspnea and leg discomfort using the 0–10 Borg scale.29 Subjects performed intermittent exercise on an electromagnetically braked cycle ergometer. Intensity at the beginning of the program was equivalent to 50% of WRpeak (measured at baseline), with 30 s of work alternated by 30 s of rest periods for 30 min/session.30 The work load was increased weekly by 10% of baseline work rate based on subject’s Borg scale symptoms of breathlessness and leg discomfort. The work load was increased when Borg dyspnea and/or leg discomfort were reduced by 1 unit for a given work load. During training, heart rate was recorded by a pulse oximeter, and the Borg (0–10) scale was used for the evaluation of breathlessness and leg discomfort. The rehabilitation program also included upper- and lower-limbs resistance training sessions using fitness equipment. In particular, subjects performed 4 resistance exercises, namely knee extension, seated chest press, peck deck, and lateral pulldown, at an intensity equivalent to 60–70% of one repetition maximum (performed at baseline) with 3 sets of 10 repetitions/exercise.31 The duration of each rehabilitation session was 1 h.
Safety precautions included infection prevention and control measures, exclusion of active infection, and control of disease-related complications. In brief, necessary protection measures were taken into consideration to avoid the spread of the virus in the facilities where the evaluation of subjects and delivery of rehabilitation services took place. These measures are described in detail by the Hellenic National Public Health Organization (HNPHO).32 Subjects upon arrival at the rehabilitation center were screened for active disease according to the guidance issued by the HNPHO for discontinuation of precautionary measures in a patient with (life threatening) COVID-19 infection following hospital discharge.32 Evaluation and rehabilitation of subjects took place in properly ventilated facilities, with each subject individually, and a time separation of 1 h between assessments and rehabilitation sessions was implemented. According to BTS guidance, a series of possible complications of COVID-19 infection were taken into account during the initial evaluation including thromboembolic disease; complications from the heart, mainly myocarditis; and the detection of hypoxemia during exertion.33 The safety precautions that were followed have been described in detail by the Hellenic Thoracic Society.14,34
Study Outcomes
Our primary objective was to determine whether increases in the 6MWT distance of ≥ 50 m at 8 weeks post enrollment was associated with rehab, while concurrently controlling for potential confounders such as time from COVID-19 symptoms onset to rehab initiation or study enrollment as control, age, sex, and preceding hospitalization and ICU admission for COVID-19. Our secondary objectives comprised the determination of potential associations of the above-defined, clinically relevant improvements in measurements of physical function, symptoms, mental health, and HRQOL at 8 weeks post enrollment with rehab, while concurrently controlling for all of the aforementioned potential confounders.
Statistical Analysis and Sample Size Estimation
Analyses were performed using SPSS version 25 (IBM, Armonk, New York). Distribution normality was tested by the Kolmogorov-Smirnov test. Descriptive statistics are presented as median (interquartile range). Depending on distribution normality, comparisons of baseline characteristics between the rehab and control groups were conducted using the independent samples t test or the Mann-Whitney U test. The Fisher exact test was used for between-group comparisons of proportions. All tests were 2 tailed.
The primary outcome analysis comprised multivariate logistic regression with improvement or no improvement in the 6MWT as the binary dependent variable; the explanatory variables included in the model were rehab (yes vs no), time from COVID-19 symptoms onset to study enrollment (d), age (y), sex (male vs female), preceding hospital admission due to COVID-19 (yes vs no), and ICU admission (yes vs no) due to COVID-19. Secondary outcome analyses comprised the fitting of logistic regression models using the same explanatory variables and having as dependent variables the improvement or no improvement in each one of the abovementioned tests of physical function, symptoms, HRQOL, and mental health (besides the 6MWT). Results of logistic regression analyses are presented as adjusted odds ratios (aORs) (95% CI). To prevent overfitting of logistic regression models, at least 20 measurements (observations) per independent variable were required.35 As there were 6 pre-specified independent variables, the study was scheduled to end on the completion of the follow-up of 120 subjects. Statistical significance was set at P < .05 for all analyses.
Results
Subject Participation and Demographics
One hundred thirty-four subjects were initially recruited, of whom 9 in the control group were lost at follow-up and 5 in the rehab group who couldn’t complete the program due to transportation and logistics reasons. In total, 120 subjects completed the study; 47 participated in the rehabilitation program, and 72 composed the control group. Οne subject withdrew the informed consent and was excluded from the analysis, thus reducing the study population to 119 subjects. No adverse effects were reported during rehabilitation.
The subjects age ranged from 24–79 y, of whom 21 subjects (17.5%) exceeding 65 y. There were no significant between-group differences in sex, age, comorbidities, and number of symptoms between the 2 groups. Furthermore, rehab subjects and control subjects had similar numbers of days from COVID-19 symptoms onset until study enrollment. Hospitalization and ICU admission for COVID-19 were arithmetically (but not significantly) more frequent in the rehab group versus control (68% vs 51% and 40% vs 24%, respectively, P = .051 and .07). The rehabilitation center–to-home distance was significantly greater in the control group. Subjects’ demographics are reported in Table 1.
Baseline Characteristics
Between-Group Comparisons
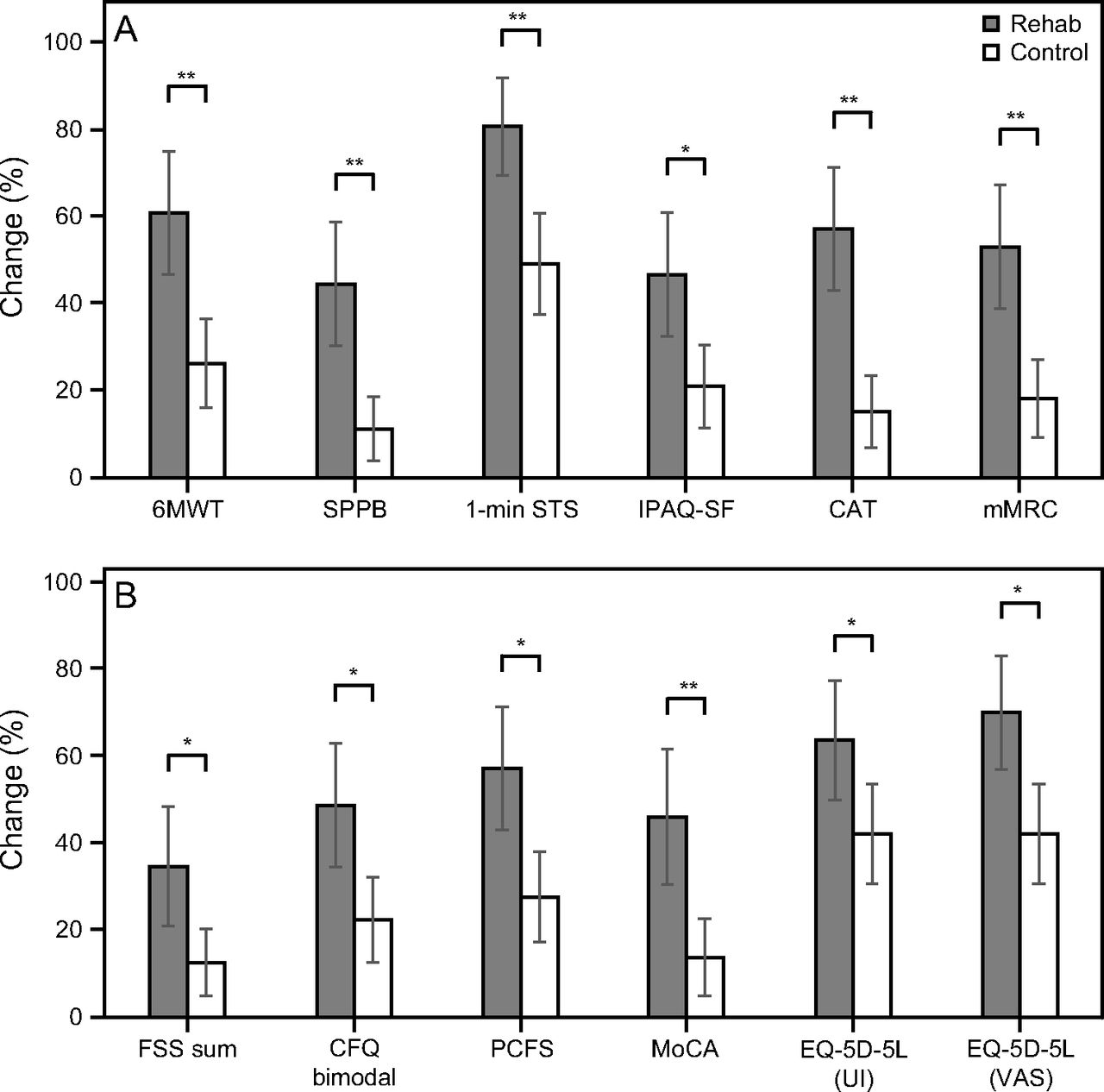
The baseline test measurements did not differ between groups, besides mMRC, which was significantly higher in rehab versus control (2 [1–3] vs 1 [1–2], respectively, P = .01) and IPAQ-SF, which was significantly higher in control versus rehab (930 [200–1,893] vs 636 [132–1,440], P = .03; e-Table 2, see related supplementary materials at http://www.rcjournal.com). Between-group comparisons of proportions are presented in the Fig. 1 and e-Table 1 (see related supplementary materials at http://www.rcjournal.com).

Between-group comparisons of proportions (expressed as percentages) after 8 weeks of A: 6-min walk test (6MWT), Short Physical Performance Battery (SPPB), 1-min sit-to-stand test (1-min STS); International Physical Activity Questionnaire - Short Form (IPAQ-SF), COPD Assessment Test (CAT), and Modified Medical Research Council dyspnea scale (mMRC); and B: Fatigue Severity Scale (FSS) sum, Chalder Fatigue Scale (CFQ) bimodal score, Post–COVID-19 Functional Status Scale (PCFS), Montreal Cognitive Assessment (MoCA), and 5-level EuroQol-5D (EQ-5D-5L) (utility index [UI] and visual analog scale [VAS]). Comparisons between groups were performed using Fisher exact test for categorical data. *P < .05. **P < .001. Error bars = 95% CI.
Results of Multivariate Analyses
Table 2 displays the main results of the primary and secondary outcomes logistic regression analyses. Participation in rehab versus control was 4.6 times more likely to increase the 6MWT distance more than 50 m, 7.9 times to restore physical performance (SPPB > 10), 4.6 times to perform > 3 repetitions in 1-min STS, 3.6 times to increase physical activity (IPAQ > 600), 7.4 times more likely to decrease the burden of respiratory symptoms (CAT < 10), 4.4 times to reduce dyspnea (mMRC < 2), 4.1 times to alleviate severe fatigue recorded over the past 2 weeks (FSS < 36) and 3.3 times over the past month (Chalder-bim < 4), 3.5 times to improve post–COVID-19 functional status (PCFS < 2), 6.3 times to restore cognitive function (MoCA ≥ 26), and 3.1 times to increase HRQOL (EQ-VAS ≥ 6.9). Neither rehab nor control subjects reached average health measured with SF-36 after 8 weeks (e-Table 3, see related supplementary materials at http://www.rcjournal.com).
Main Results of the Primary and Secondary Outcomes Logistic Regression Analyses
The probability of increase in the 6MWT distance by ≥ 50 m decreased slightly with time from COVID-19 symptoms onset to study enrollment (AOR 0.996 [95% CI 0.993–1.000]). Subject hospitalization increased 3.4 times the probability of improving the post–COVID-19 functional status and 3.5 times the probability of dyspnea reduction after 8 weeks. Descriptive statistics and logistic regression models for HADS, SF-36, FACIT, ABC, BID, and IES-R as dependent variables are reported in the supplemental material (e-Table 3 and e-Table 4, see related supplementary materials at http://www.rcjournal.com).
Discussion
In the present study, rehabilitation was associated with concurrent, multiple improvements in the measures of physical and cognitive function, fatigue, respiratory symptoms, dyspnea, and HRQOL. These improvements were clinically important and not associated with age, sex, and ICU admission. Prior hospitalization was associated only with dyspnea and post–COVID-19 functional scale improvement. Days from disease onset to enrollment were marginally associated with not exceeding the 50-m distance threshold in 6MWT. These findings support the hypothesis that rehabilitation may substantially contribute to the reversal of multiple components of post–COVID-19 impairment in a population with substantially variable age, disease severity, and time elapsed from disease onset.
A strength of our study pertains to the adjustment of the multivariate analyses for potential confounders. The sole moderating effect on improved, rehabilitation-associated functional outcomes of elderly subjects who McCarthy et al11 were able to examine in their review and meta-analysis was the length of stay in rehabilitation units. Meta-regression showed that the length of stay was not associated with functional outcomes (P = .30). In another systematic review and meta-analysis of 14 observational studies, only two adjusted their analyses for potentially confounding factors (ie, ICU admission/length of stay and preexisting comorbidities), highlighting this absence as the most important risk of bias.3
Prior disease severity and time from disease onset to rehab might affect rehabilitation-associated outcomes due to the intervening natural recovery. Severely affected patients (lower baseline values) may have the potential of greater improvement, toward the predicted pre-disease values of population of similar age and comorbidities. In our previous study, post–COVID-19 subjects with severe pneumonia recruited 42 d after hospital discharge and following usual care increased the 6MWT distance from a mean ± SD of 408.3 ± 85.7 m to 466.2 ± 83.4 m in 8 weeks, not differing from rehab.8 Gloeckl et al7 recruited subjects with prior severe/critical and mild/moderate COVID-19 into a supervised rehabilitation program. Subjects with severe prior disease had a median increase in the 6MWT distance of 124 m, starting from a baseline median value of 344 m; subjects were recruited in the program at a median time of 18 d after hospital discharge. In contrast, subjects with mild-to-moderate COVID-19 who were recruited 178 d after positive PCR testing had a higher baseline exercise performance (ie, median 6MWT distance of 509 m) and achieved a smaller median increase of just 48 m at the end of the rehabilitation. This finding can be explained by the interaction of disease severity and natural recovery.7 In the present study, subjects’ mean baseline 6MWT distance was 490 m and increased by 62 m in rehab versus 11.5 m in the controls (P < .001, e-Table 3, see related supplementary materials at http://www.rcjournal.com).
An interesting finding of our study was that prior hospitalization was associated with improvements in dyspnea and post–COVID-19 functional status after 8 weeks. Dyspnea is a persistent symptom in patients with post–COVID-19 sequelae. In a large survey of post–COVID-19 subjects, over half of them (ie, 395 of 769 or 51.4%) suffered from breathlessness at 1 y after disease onset.10 Subjects with severe COVID-19 had worse mMRC scores at 14 d and 6 months after discharge compared to subjects with moderate disease.36 A small mean decrease in mMRC (ie, from 1.1 to 0.9) has been reported in a small series of subjects recovering from COVID-19 in just 15 d after hospital discharge.37 In the present study, rehabilitation was associated with amelioration of dyspnea since more than half (ie, 53%) of the rehab subjects had mMRC score 0 or 1 after 8 weeks of participation in the program.
Rehabilitation in elderly post–COVID-19 patients is challenging due to multiple comorbidities, frailty, immunosenescence, and an increased probability of more severe prior disease and accelerated functional decline.11 The understanding of the risk profiles of older patients and the development of individualized treatment regimens are of paramount importance.38 Improvements in functional outcomes,11 respiratory function, HRQOL, and mental health39 after rehabilitation in elderly patients are promising; however, there is lack of evidence regarding long-term effects.38,11 In the present study, age was not associated with changes in functional status, HRQOL, mental health, or symptoms after 8 weeks. However, < 1/5 of the study population was > 65 y of age; consequently, multivariable analytic determination of associations between rehabilitation and pre-specified study outcomes was not feasible in this small subgroup.
The current study is limited by the absence of randomization. Post–COVID-19 rehabilitation services are still limited in Greece, and with the number of symptomatic post–COVID-19 patients on the rise, it was considered as unethical to deny participation in a potentially effective and safe therapeutic intervention.3,4 The majority of controls couldn’t participate in the program, mainly for reasons beyond their will. Indeed, the mean distance to reach the rehabilitation center in the control group was significantly longer compared to the rehab group (Table 1). Logistic and transportation issues, along with inflexible obligations and poor perception of rehabilitation’s benefits have been previously identified as major factors for declining pulmonary rehabilitation.40 Although subject characteristics and most baseline measurements did not differ significantly between the 2 groups, we adjusted our analyses for several potential confounders.41 Therefore, our results strongly support the hypothesis that rehabilitation may effectively address post–COVID-19 sequelae, independently from confounders such as the timing of intervention relative to disease onset and disease-related hospital and/or ICU admission.
Another limitation of our study is the low frequency of supervised rehabilitation sessions (twice a week). The ERS/ATS,31 the American College of Sports Medicine,42 and American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR)43 recommend a frequency of 3–5 times/week of endurance training. However, our post–COVID-19 rehabilitation program was designed and implemented during the pandemic when lockdown measures were enforced, and transmission precautions were strictly followed. Consequently, rehabilitation sessions were held individually and 1 h apart between subjects to properly ventilate facilities and disinfect equipment, thereby significantly decreasing program capacity. Reducing session frequency to a minimum (supervised sessions twice a week according to BTS44) and keeping a total program duration of 8 weeks within recommendations (4–12 weeks according to AACVPR43 and 6–8 weeks according to BTS44) were seen as an unavoidable compromise in order to continue providing rehabilitation services during the pandemic to as many patients as possible. The duration of 30 min of aerobic training and 1 h total session duration was as recommended.45 The efficiency of our post–COVID-19 rehabilitation program has been proven,8 and there was no adjustment in duration and frequency after the end of the pandemic. Finally, an additional limitation pertains to the absence of long-term follow-up, which might have been informative as regard to any potential long-term effects of pulmonary rehabilitation.11
New randomized control studies aim to investigate the long-term effects of rehabilitation and compare directly supervised with non-directly supervised programs utilizing new supportive technologies.46 Such trials will provide valuable knowledge on the feasibility and effectiveness of new rehab programs in the context of personalized medicine.47
Conclusions
In the current non-randomized study, rehabilitation of subjects with post–COVID-19 sequelae was associated with improvements in physical function, respiratory symptoms, severe fatigue, cognitive impairment, and HRQOL. These improvements were clinically important and were not associated with preceding disease severity, time from disease onset to rehab, age, and sex.
Footnotes
- Correspondence: Andreas Asimakos MD PhD, Ypsilantou Street 45–47, 10676, Athens, Greece. E-mail: silverakos{at}gmail.com
The authors have disclosed no conflicts of interest.
A version of this paper was presented at the 32nd Panhellenic Pulmonology Congress, held December 7–10, 2023, in Athens, Greece.
Supplementary material related to this paper is available at http://www.rcjournal.com.
See the Related Editorial on Page 1477
- Copyright © 2024 by Daedalus Enterprises





{kind=link}