
Abstract
BACKGROUND: The objective of the present study was to develop predictive equations for maximum respiratory pressures in women according to anthropometric characteristics.
METHODS: This cross-sectional study included 156 women between ages 25 and 65 y with a body mass index (BMI) between 18.5 and 55 kg/m2, who were evaluated for body mass, height, BMI, neck circumference, waist circumference, hip circumference, and waist/hip ratio. Respiratory muscle strength was assessed by measuring the maximum inspiratory pressure (PImax) and maximum expiratory pressure (PEmax) with an analog vacuum manometer. For statistical analysis, the Kolmogorov-Smirnov test, Spearman correlation test, and stepwise multiple regression were used. The level of statistical significance was set at 5% (P < .05).
RESULTS: Body mass, BMI, neck circumference, waist circumference, hip circumference, and waist/hip ratio showed significant and positive correlations with PImax and PEmax. On the other hand, age and height showed no significant correlations with PImax and PEmax. In the regression analysis, the variables that correlated significantly with PImax and PEmax were used.
CONCLUSIONS: Body mass was the variable that best contributed to predicting maximum respiratory pressures values in women (11.70% of the variations of the PImax and 21.05% of the variations of the PEmax). For PImax measurements, the equation −0.2 × body mass − 65.6 was established, and for PEmax, the equation 0.3 × body mass + 66.4 was used. It is suggested that the predictive equations developed in this study can be used in the interpretation of the assessment of respiratory muscle strength in morbidly obese women 25–65 y of age.
- women
- obesity
- respiratory muscle
- muscle strength
- reference values
- physical therapy
Introduction
Obesity has been regarded as a public health problem for some time, and it is currently becoming a worldwide epidemic. In 2008, >1.4 billion adults were overweight, 300 million of whom were women.1 In addition to promoting the development of comorbidities,2 obesity can modify respiratory muscle strength.3 However, no consensus has been reached in the literature concerning the behavior of the respiratory muscles in the presence of increased body mass index (BMI).4–6
According to Magnani and Cataneo,5 individuals with obesity have respiratory muscle dysfunction due to changes in the relationship between the lung, chest wall, and diaphragm muscle, which in turn alter respiratory mechanics and gas exchange. It is believed that these changes cause overload in the respiratory muscles, increasing the mechanical work involved in respiration. This occurs due to the increased deposition of fat in the chest wall, which increases the body mass that needs to be moved during the respiratory cycle. This overload can cause an increase in the activity of respiratory muscles and causes the training effect and, in the long term, may increase respiratory muscle strength.5,7,8
One of the ways of evaluating respiratory muscle strength is by measuring the maximum respiratory pressure produced during maximum inspirations and expirations, thus characterizing the strength of the inspiratory and expiratory muscles.9 Based on the values obtained by measuring the maximum respiratory pressures, it is possible to calculate predicted values of normality through mathematical equations.
Several authors10–12 have determined reference values by means of equations considering sex and age. In a study of healthy sedentary individuals between 20 and 89 y old, Simões et al13 investigated the relationship of maximum respiratory pressures with age, height, and body mass and proposed predictive equations. They showed that, for women, age and body mass had a negative influence on measures of maximum respiratory pressures; however, it is worth noting that the BMI of the studied population was <30 kg/m2.
Pazzianotto-Forti et al14 evaluated the behavior of respiratory muscle strength in morbidly obese individuals using 3 different predictive equations and found 3 different results (predicted values) for the same value obtained. This suggests that the existing equations in the literature are not able to provide a reliable prediction of respiratory muscle strength for the morbidly obese and justifies the inconclusive results found in the literature on respiratory muscle strength in this population.
According to Harik-Khan et al,15 respiratory muscle strength is correlated with age, sex, weight, height, and body surface area. Given these findings, the authors developed a predictive equation for measurements of maximum inspiratory pressures (PImax), taking into account sex and height as well as body mass. However, we did not find predictive values for expiratory muscle strength according to body mass in the literature, emphasizing the need for the development of predictive equations to enhance the reliability and interpretation of the behavior of the respiratory muscles in the presence of obesity.
Due to the influence of anthropometric characteristics on respiratory muscle strength and considering the lack of predictive equations for respiratory muscle strength in morbidly obese women,10–13 the aim of this study was to develop predictive equations for maximum respiratory pressures in Brazilian women age 25–65 y according to body mass.
QUICK LOOK
Current knowledge
Due to the influence of anthropometric characteristics on respiratory muscle strength and considering the lack of predictive equations for respiratory muscle strength in morbidly obese women, there is a need for the development of predictive equations to enhance the reliability and interpretation of the behavior of the respiratory muscles in the presence of obesity.
What this paper contributes to our knowledge
Given that to date, no study has provided maximum respiratory pressures specific for the obese and morbidly obese populations or indicated the most appropriate equations available in the literature, these results will be useful in understanding and assessing the behavior of respiratory muscle strength in obesity and will also assist in the development of treatments to maintain and improve the strength of these muscles.
Methods
Subjects
Recruitment.
This was a cross-sectional study consisting of 156 adult women, who were informed about the objectives of the study and signed a consent form. The study was approved by the Research Ethics Committee of Universidade Metodista de Piracicaba (UNIMEP), Piracicaba, São Paulo, Brazil (protocol number 49/12).
The sample size calculation was based on a pilot study that aimed to evaluate the influence of age and anthropometric characteristics on respiratory muscle strength. A significant correlation between BMI and PImax was considered. The value of r = 0.35 was used for the calculation because it was the strongest correlation found between BMI and PImax. The linear correlation test, adopting a statistical power of 95% and an α of 0.05, was also used. Thus, a minimum of 101 subjects was determined. The processing of the sample size calculation was performed using BioEstat 5.3 (Instituto de Desenvolvimento Sustentável Mamirauá, Belém, Brazil). Then 101 subjects were divided into 16 groups according to age and BMI. For homogenization of the groups regarding the number of subjects, each group had at least 6 subjects.
Obese and morbidly obese women were screened in a treatment clinic of obesity. Eutrophic and overweight women were recruited in the community by invitation to participate in the study.
Inclusion Criteria.
The inclusion criteria were women with a BMI between 18.5 and 55 kg/m2, age between 25 and 65 y, and sedentary lifestyle.
Exclusion Criteria.
The exclusion criteria were as follows: presence of comorbidities, such as decompensated hypertension and diabetes; cardiovascular or pulmonary disease; presence of alterations in the thoracic and/or abdominal region; respiratory dynamics alterations; smoking; and inability to perform the assessments. All experimental procedures were performed in the Laboratory for Assessment and Intervention in Cardiorespiratory Physiotherapy of the university.
Clinical Assessment
After anamnesis and clinical history, anthropometric measurements were taken. To measure body mass, the subjects stood without shoes or heavy clothing on a digital scale (Welmy, Santa Bárbara D'Oeste, Brazil) calibrated with maximum capacity of 300 kg and 100 g resolution. Height was measured with the scale's stadiometer with resolution in millimeters.
The calculation of BMI was obtained by the equation, body mass/height2 (kg/m2). The circumferences were measured in centimeters using a non-elastic tape measure. Neck circumference was measured at the cricoid cartilage16; waist circumference was measured at the midpoint between the margin of the last rib and the upper margin of the iliac crest; hip circumference was measured at the greater trochanter of femur17; and with the measures of waist circumference and hip circumference, the waist/hip ratio was obtained.
For the assessment of respiratory muscle strength, maximum respiratory pressures were measured using an analog vacuum manometer (Criticalmed, Rio de Janeiro, Brazil), with an operating range of ±300 cm H2O. The mouthpiece has a 2-mm leak hole to prevent glottic closure during the maneuver of PImax and reduce the use of facial muscles during the PEmax maneuver.
The PImax was measured from residual volume, and PEmax was measured from total lung capacity. A 1-min interval was allowed between efforts. To perform these measurements, subjects were instructed to remain seated and use a nose clip. All subjects performed ≥3 technically acceptable and reproducible efforts (ie, without perioral air leakage, sustained for at least 2 s, and with similar values [within 10%]). For data analysis, the highest value was used.11
Data Analysis
The distribution of data was verified by the Kolmogorov-Smirnov test, followed by the Spearman correlation test to assess possible relationships of variables with PImax and PEmax. Stepwise multiple regression was used to develop predictive equations for the maximum respiratory pressures. Only variables that showed significant correlations with PImax and PEmax were included in the model. The level of statistical significance was set at 5% (P < .05). All statistical procedures were performed using the statistical programs SPSS 17.0 (SPSS, Chicago, Illinois) and R 3.1.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Subjects
One hundred eighty-one subjects were screened, 25 of whom were excluded according to the established criteria. Therefore, 156 women, divided for convenience into groups according to BMI and age, were evaluated as shown in the flow diagram (Fig. 1).

Flow chart.
Findings From Clinical Assessment
Table 1 shows the data for the age, anthropometric characteristics, and body fat distribution of the sample, divided by BMI. Table 2 shows the values for the maximum respiratory pressures collected from the 156 subjects. Figures 2 and 3 show the results of the correlations of the maximum respiratory pressures with anthropometric characteristics.
Anthropometric Characteristics and Measurements of the Circumference of the Neck, Waist, and Hip and Waist/Hip Ratio of the 156 Subjects Studied, Distributed in Groups According to Body Mass Index
Maximal Respiratory Pressures Obtained From 156 Subjects Studied

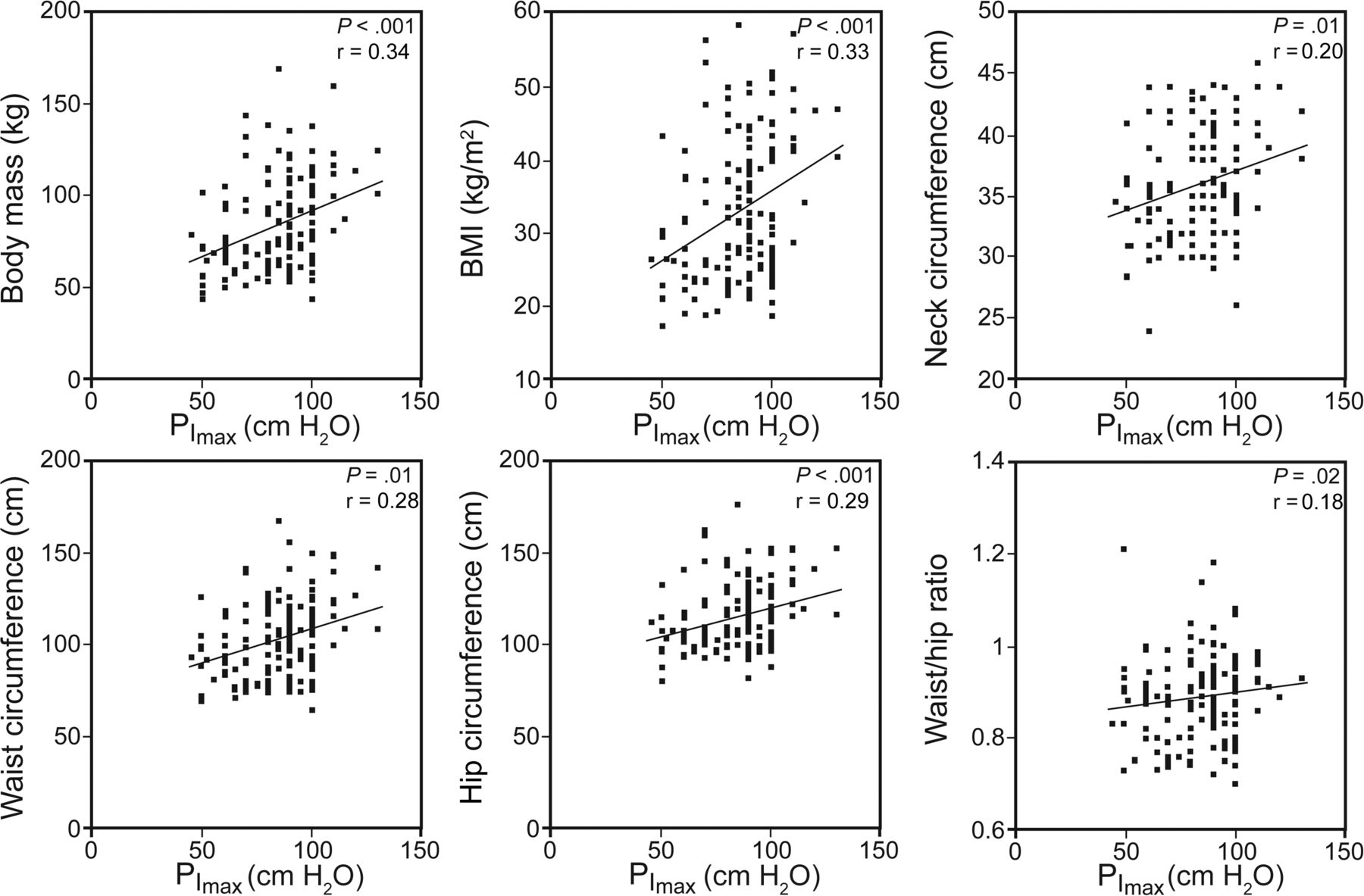
Correlations between PImax and anthropometric variables.

{kind=link}
{kind=link}
{kind=link}
Correlations between PEmax and anthropometric variables.
Age and height had no significant correlations with PImax (P = .96 and P = .70) or PEmax (P = .14 and P = .20). On the other hand, body mass, BMI, neck circumference, waist circumference, hip circumference, and waist/hip ratio showed significant and positive correlations with PImax and PEmax (P < .05).
The variables that showed positive correlations with PImax and PEmax were included in the stepwise multiple regression for the development of predictive equations for maximum respiratory pressures. Body mass was the variable that best contributed to variations in the maximum respiratory pressures. All variables added together explained 15.16% of the variations of the PImax and 24.69% of the variations of PEmax. Body mass alone explains 11.70% of the variations of the PImax and 21.05% of the variations of PEmax. Based on these results, the new equations were developed for maximum respiratory pressures, taking into account body mass.
Table 3 shows the predictive equations model proposed for maximum respiratory pressures in women according to body mass. These results are based on the stepwise multiple regression. Tables 4 and 5 show the stepwise multiple regression analyses.
Predictive Equations for Maximum Respiratory Pressures in Brazilian Women Age 25–65 y According to Body Mass
Regression Analysis Considering Maximum Inspiratory Pressure as a Dependent Variable
Regression Analysis Considering Maximum Expiratory Pressure as a Dependent Variable
Discussion
The study reveals that body mass showed the best contribution to the variations of maximum respiratory pressures in women. Therefore, body mass was included in predictive equations for PImax and PEmax prepared in this study.
Other studies15,18 found that body mass was a positive predictor of respiratory muscle strength in both sexes. According to Arora and Rochester,19 changes in body mass could affect diaphragmatic muscle mass influencing respiratory muscle performance and thus the maximum respiratory pressures.
Santiago-Recuerda et al20 have reported that the increase in respiratory muscle strength due to the increase in body mass happens through the reversal of the muscle fiber type (ie, larger quantities of type II fibers compared with type I fibers). This is explained by the adaptation to chronic overload that accompanies obesity. Wannamethee et al21 and Sutherland et al22 reported that the increase in respiratory muscle strength is due to the increase in lean mass, hence the importance of the presence of body mass in the predictive equations, particularly for assessing respiratory muscle strength in morbid obesity.
The predictive equations available in the literature10–13 demonstrate that age, body mass, height, and sex variables have an influence on the values for maximum respiratory pressures. However, it is noteworthy that, in most of these predictive equations, body mass was not used as a component because the regression analysis only shows predictive power for age and height. It should be emphasized that these equations were obtained in eutrophic populations and not in obese people. Therefore, the real contribution of obesity to respiratory muscle strength as an independent variable could not be evaluated and interpreted,23 making the behavior of respiratory muscle strength in obesity inconclusive and controversial.4–6
In this study, the variables age and height showed no correlations with the maximum respiratory pressures; thus, they were not included in the linear regression model. This may have been due to the homogeneity of the groups with regard to these variables, unlike in the studies of Black and Hyatt,10 Neder et al,11, Costa et al,12 and Simões et al,13 in which these variables showed a negative predictive importance for maximum respiratory pressures. One explanation for this may be the differences in age between the samples, which ranged from 20 to 86 y. These results may be due to the sarcopenia associated with aging,24 whereas in the present study, women up to 65 y old were assessed, who were probably not affected by the changes of aging.
Therefore, predictive equations of PImax and PEmax are possible alternatives and can be used for the obese and morbidly obese population and thus direct conclusions about the interpretation of respiratory muscle strength in obesity. That is especially relevant to morbidly obese candidates for abdominal surgery,25 given that respiratory muscle dysfunction is the major cause of pulmonary complications after surgical procedures.26 For obese individuals, independent of surgical procedures, respiratory muscle dysfunction may lead to hypoventilation, dyspnea, and exercise intolerance and, in extreme cases, respiratory insufficiency.27,28
Given that to date no study has provided maximum respiratory pressures specific for the obese and morbidly obese populations, or indicated the most appropriate equations available in the literature, we suggest that the predictive equations developed in this study be used in the interpretation of respiratory muscle strength assessments in morbidly obese women between the ages of 25 and 65 y.
Study Limitations
The study was conducted by means of BMI classification to identify eutrophic, overweight, obese, and morbidly obese subjects. Although BMI is recommended by the World Health Organization due to its convenience and affordability, we do not reject the contribution of a more reliable assessment to measure lean mass and body fat. The absence of men in the present study limits the results to the female sex.
Clinical Relevance
The use of the equations proposed in this study will be useful in understanding and assessing the behavior of respiratory muscle strength in obesity. These will also assist the development of treatments to maintain and improve the strength of these muscles, thus preventing respiratory complications as a result of surgery, pulmonary diseases, and aging, reducing dyspnea, and increasing tolerance to exercise. Finally, these treatments might improve health and quality of life and reduce mortality in this population.
Footnotes
- Correspondence: Eli Maria Pazzianotto-Forti PhD, Rodovia do Açúcar, 156 Km Taquaral CEP, 13400-911, Piracicaba-SP, Brazil. E-mail: empforti{at}unimep.br.
This work was supported by Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP), São Paulo, Brazil, process no. 13/06334-8. The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.