
Abstract
BACKGROUND: To increase the understanding of the self-extubation phenomena, we assessed its rate in our medical ICU and aimed to identify the risk factors of self-extubation and the risk factors for re-intubation.
METHODS: We prospectively identified subjects who self-extubated. Their baseline characteristics, including the Richmond Agitation Severity Scale score, reason for intubation, shift, distance of the endotracheal tube tip to the carina, and outcomes were collected retrospectively. For every subject who self-extubated, a control subject was selected from the mechanical ventilation database.
RESULTS: During the study period, there were 2,578 admissions with 4,072 mechanical ventilation days. Fifty-three cases of self-extubation were recorded, which resulted in a self-extubation event rate of 1.3 per 100 days of mechanical ventilation. Forty-five controls were identified. The most common reason for intubation was hypoxic respiratory failure, followed by the need for airway protection and hypercapnic respiratory failure. Sedation was administered continuously in 34% of the subjects. Thirty-seven percent received no sedation. At the time of the event, the subjects who self-extubated had a higher Richmond Agitation Severity Scale score, a longer distance from the endotracheal tip to carina on the chest radiograph preceding the event, and a shorter duration of mechanical ventilation, and were more likely to be on volume-controlled mechanical ventilation. ICU mortality was lower in the self-extubation group, despite having a trend toward a higher Simplified Acute Physiology Score II. Sixteen subjects required re-intubation. Independent predictors of re-intubation were hypoxic respiratory failure as the reason for the initial intubation and self-extubation that occurred at night. The need for re-intubation was not associated with higher mortality.
CONCLUSIONS: Results of our study showed that, in the era of reduced use of sedatives in the ICU, clinicians must be vigilant of the risk of self-extubation in the first 2 d of mechanical ventilation in patients who are agitated and with a longer endotracheal tube to carina distance on chest radiograph.
- self-extubation
- mechanical ventilation
- medical intensive care unit
- predictors of self-extubation
- predictors of reintubation
Introduction
ICUs admit patients who are the most vulnerable and ill. These patients are frequently defenseless, fully dependent on the care provided by the medical staff, and frequently unable to communicate. This is most apparent in patients on mechanical ventilation, who constitute up to 46% of patients in an ICU.1 Although frequently lifesaving, mechanical ventilation has its complications. One of which is the unplanned removal of the endotracheal tube (ETT) or unplanned extubation. This encompasses self-extubation in which the ETT is removed deliberately by the patient and accidental extubation in which the ETT is dislodged from the airway due to maneuvers during patient care.
Unplanned extubation has been associated with increased morbidity and mortality,2–5 particularly when patients require re-intubation.2,3,6 Understanding the burden of this phenomenon is confounded by how it is reported. Rates of unplanned extubation, accidental extubation, and self-extubation are reported separately or are aggregated. Rates of unplanned extubation range from 0.5 to 19 per 100 patients on mechanical ventilation or 0.1 to 3.6 per 100 mechanical ventilation days. Self-extubation accounts for the majority of unplanned extubations (68–95%).7–9
The current understanding of unplanned extubation is from prospective and retrospective cohort studies.2–9 Some investigators have used an historical case-control study design to identify risk factors for unplanned extubations. The majority of these studies4,5,7,9 have shown that patients at risk for unplanned extubation are restless and agitated; however, other studies found that awake and cooperative patients are also at risk.7,10 Some studies found that age, sex, underlying chronic respiratory disease, severity of illness, mode of mechanical ventilation, nursing level of experience, night shift, time around shift change, and a shorter ICU length of stay were associate with unplanned extubation.5,7,10–17 Only one study found that a longer distance of the ETT tip from the carina was associated with an increased risk for self-extubation.18 The reason for the variability in the identified risk factors found for unplanned extubation and self-extubation are due to the differences in design, sample size, care of subjects on mechanical ventilation, type of ICU, diagnosis, reason for mechanical ventilation, and if only self-extubation or all unplanned extubations were assessed as outcomes.
Outcomes of unplanned extubations vary, depending on the type of ICU (surgical vs medical vs mixed), patient population (young vs elderly), diagnosis, and need for re-intubation.2,5,7 Between 2 and 90% of patients with unplanned extubation require re-intubation, with approximately half of these patients needing it within the first hour of self-extubation. The reasons for re-intubation are mostly airway or hemodynamic compromise, and many of these intubations are difficult.2–4,6,7,11,12,19–22 Risk factors for re-intubation include age, underlying pulmonary disease, severity of illness, the presence of >2 comorbidities, level of alertness, mode of mechanical ventilation, and  /
/ .2,7,12,22–26 Re-intubation prolongs ICU and hospital length of stay and duration of mechanical ventilation, and can result in higher mortality.2–5 Due to the inconsistency of the currently available literature and to increase the understanding of the self-extubation phenomena, we assessed the rate of self-extubation in our medical ICU and aimed to identify (1) the incidence of self-extubation, (2) its risk factors, and (3) the risk factors for re-intubation. The study was approved by the local institutional review board.
.2,7,12,22–26 Re-intubation prolongs ICU and hospital length of stay and duration of mechanical ventilation, and can result in higher mortality.2–5 Due to the inconsistency of the currently available literature and to increase the understanding of the self-extubation phenomena, we assessed the rate of self-extubation in our medical ICU and aimed to identify (1) the incidence of self-extubation, (2) its risk factors, and (3) the risk factors for re-intubation. The study was approved by the local institutional review board.
QUICK LOOK
Current knowledge
Patients at risk for unplanned extubation are restless, older men with underlying chronic respiratory disease, and with the ETT tip farther from the carina, being taken care of by a nurse with less experience and during the night shift, and in the ICU for a shorter period. Between 2% and 90% of patients with unplanned extubation require re-intubation within the first hour. Unplanned extubation has been associated with increase morbidity and mortality, particularly when patients require re-intubation.
What this paper contributes to our knowledge
We showed that, in the era of reduced use of sedatives in the ICU, clinicians must be vigilant of the risk of self-extubation in patients who are agitated during the first 2 days of mechanical ventilation, especially when the ETT tip is far from the carina on a chest radiograph. We also found that re-intubation was more likely when self-extubation occurred at night and in subjects with hypoxic respiratory failure. Mortality was lower in the subjects who self-extubated compared with those who did not self-extubate. Subjects who required re-intubation had similar mortality to those who did not require re-intubation.
Methods
Setting
In the year 2011, the 22-bed, 2-pod medical ICU at Cook County Hospital participated in a multi-center study in which a daily sedation awakening trial combined with a spontaneous breathing trial was introduced.27 After the conclusion of the study, we continued to perform daily sedation awakening trials. Two board certified intensivists staffed the medical ICU during the daytime, and 1–2 critical care fellows and 3–10 residents (RG, AT) staffed it for 24 hours. All intubation decisions between 8 am and 5 pm were made by the intensivist (RG, AT) taking care of the subject and, during after-hours, were made by the on-call critical care fellow. All intubations were performed under the supervision of the intensivist (RG, AT) or an anesthesiologist. All the subjects on mechanical ventilation underwent daily screening for a sedation awakening trial by the nursing staff, and, if passed, sedation was stopped. The intensivist (RG, AT) dictated the timing and method of weaning. All ETTs were fixed with tape and had high-volume low-pressure cylindrical cuffs, without subglottic suction. Restraints were applied when indicated.
Cases
We prospectively collected data on adverse events that occurred in our medical ICU. Every day, critical care fellows documented, in a shared database, any adverse events and the subjects' outcomes during their shift. One of the events of interest was self-extubation. An investigator (RG) reviewed each case for completeness and accuracy. The daily reporting started in August 2012 and continued for 29 months.
Controls
For every subject who self-extubated, one control subject was selected randomly from the hospital's mechanical ventilation administrative database. The control subject had to be on mechanical ventilation in the medical ICU on the same day of the matching case of the self-extubation event, or, if not available, within 24 h of the self-extubation event. This method was chosen to control for seasonal variation in respiratory illnesses, work load, and personnel (nursing, respiratory therapist, and physician).
Data Collection
The following subject variables were recorded: age, sex, admission diagnosis, reason for intubation, and severity of illness (Simplified Acute Physiology Score II), duration of mechanical ventilation to the time of the event, mechanical ventilation mode and settings, ETT size, need for restraints, Richmond Agitation Severity Scale (RASS) score, shift (day shift [7 am to 7 pm], night shift [7 pm to 7 am]) and occurrence of the event within 1 h of shift change, and the distance of the ETT tip to the carina. The distance was measured on 2 separate chest radiographs acquired within the 48 h before the event (for both cases and controls): the first chest radiograph before the self-extubation and the second chest radiograph before the event. The change of the tip of the ETT position between these 2 latest chest radiographs was calculated. Outcomes were re-intubation within 48 h, time to re-intubation, and death in the ICU.
Analysis
In a univariate analysis, we compared the cases with the controls by using a chi-square test for categorical variables and the Mann-Whitney test for ordinal and continuous variables. We created a receiver operating characteristic curve for potential predictors of self-extubation to determine their strength and to identify optimum cutoff points. We used logistic regression to identify the independent predictors of self-extubation. P = .05 indicated the presence of a statistically significant difference. All statistical analysis were performed by using MedCalc (MedCalc Software, Mariakerke, Belgium).
Results
Rate of Self-Extubation and Its Predictors
During the 29-month period, there were 2,578 admissions to the medical ICU, which resulted in 4,072 mechanical ventilation days. During this period, there were 53 cases of subjects who self-extubated, which resulted in a self-extubation event rate of 1.3 per 100 days of mechanical ventilation. Forty-five controls were identified. There were no matches for 8 cases because there were no other subjects on mechanical ventilation on the day or within 24 h of the self-extubation event.
The most common reasons for intubation were hypoxic respiratory failure (n = 40), airway protection (n = 36), hypercapnic respiratory failure (n = 19), and the need for facilitation of procedures (n = 3). Eighty-seven percent of the subjects had restraints applied. Sedation was administered continuously in 34% and intermittently in 29% of the subjects. Thirty-seven percent received no sedation. Thirty of the subjects (83%) who received no sedation had restraints applied.
Most subject characteristics, including type of sedation (ie, none, intermittent, or continuous) and severity of disease were similar between the case subjects and the control subjects. In comparison with the control subjects, the case subjects had a higher RASS score, a longer ETT tip to carina distance on the chest radiograph closest to the self-extubation, a shorter duration of mechanical ventilation, and were more likely to be on volume-controlled mechanical ventilation (Table 1). ICU mortality was lower in the self-extubation group (5.5 vs 22%, P = .035).
Subject Baseline Characteristics
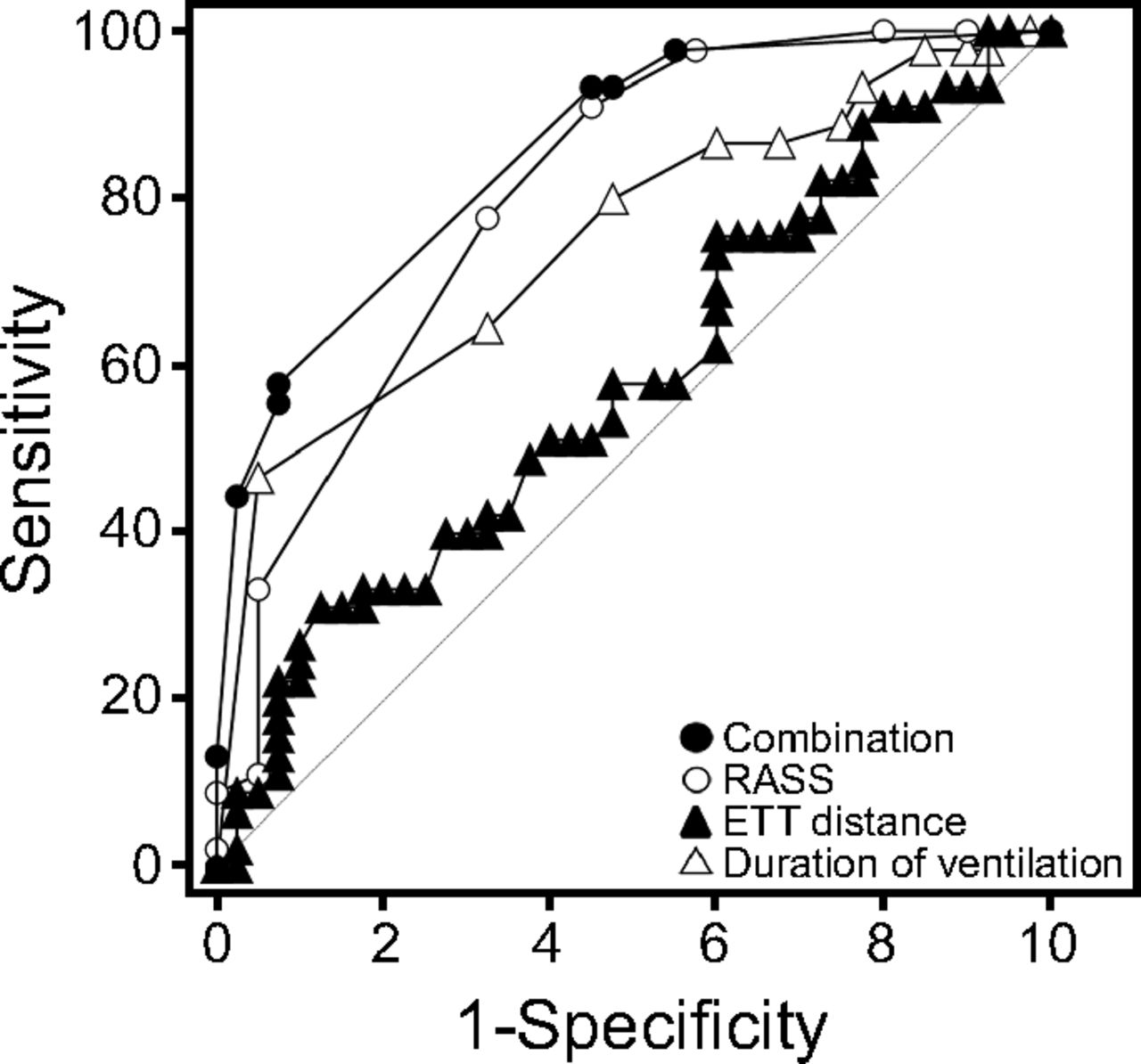
The area under the curve for RASS was 0.8 (95% CI 0.7–0.9; P < .001). A RASS score > 1 (the subject being agitated to combative), had a low sensitivity (11%) but high specificity (96%), whereas a RASS score > −2 (subject drowsy to combative) was associated with a high sensitivity (91%) but low specificity (58%) to predict self-extubation. The ETT tip to carina distance had an area under the curve of 0.6 (95% CI 0.5–0.7; P = .19). When using a distance cutoff of > 59 mm, this variable had a specificity of 87.5% and a sensitivity of 31% to predict self-extubation. Also, the area under the curve for the duration of mechanical ventilation was 0.7 (95% CI 0.6–0.8; P < .001).
Mechanical ventilation of ≤1 d was associated with a sensitivity of 44% and a specificity of 89% to predict self-extubation (Fig. 1, Table 2). The 3 variables of RASS score > −2, the ETT tip to carina distance of >59 mm, and days of mechanical ventilation of <2 were significant in the multivariate logistic regression model analysis. The duration of mechanical ventilation had the highest odds ratio (OR), followed by the RASS score and the ETT tip to carina distance (Table 3). The type of shift (day vs night) and proximity to shift change were not associated with self-extubation. Interestingly, the subjects who self-extubated during the night shift had a significantly higher median Simplified Acute Physiology Score II (42 [interquartile range |IQR}, 30–56] vs 29 [IQR, 17–42]; P = .004), were older (median 44 [IQR, 38–60] y vs 59 [IQR, 51–63] y; P = .03), and were more deeply sedated (median RASS score 0 [IQR, 0–1] vs 0 [IQR, –1 to 0]; P = .004).
{kind=link}
The receiver operating characteristic curve for Richmond Agitation Sedation Scale (RASS), duration of mechanical ventilation, and distance of endotracheal tube (ETT) are shown. Combination = combination of all measurements.
Predictors for Self-Extubation Subjects
Predictors for Self-Extubation Subjects by Using Logistic Regression
Re-intubation and Its Predictors
Sixteen of the 53 subjects (30%) who self-extubated required re-intubation within 48 h. These subjects were similar to the subjects who did not require re-intubation in age, sex, severity of disease, need for  > 40%, PEEP, need for >2 days of mechanical ventilation, and type of sedation. The re-intubation rate was higher if the initial indication for intubation was hypoxic respiratory failure (62%) than for other reasons (38%) (P = .046). Re-intubation was more likely in the subjects who were sedated (RASS score < −1) (P = .002) but was not associated with the type of administered sedation (P = .62). More subjects were re-intubated during the night shift compared with the day shift (12 vs 4; P = .01). Re-intubation was not associated with higher mortality in the subjects who self-extubated (Table 4). Independent predictors of re-intubation by using logistic regression analysis were hypoxic respiratory failure as the reason for the initial intubation (OR 6, 95% CI 1.4–23; P = .02) and self-extubation that occurred at night (OR 7, 95% CI 1.6–29; P = .01).
> 40%, PEEP, need for >2 days of mechanical ventilation, and type of sedation. The re-intubation rate was higher if the initial indication for intubation was hypoxic respiratory failure (62%) than for other reasons (38%) (P = .046). Re-intubation was more likely in the subjects who were sedated (RASS score < −1) (P = .002) but was not associated with the type of administered sedation (P = .62). More subjects were re-intubated during the night shift compared with the day shift (12 vs 4; P = .01). Re-intubation was not associated with higher mortality in the subjects who self-extubated (Table 4). Independent predictors of re-intubation by using logistic regression analysis were hypoxic respiratory failure as the reason for the initial intubation (OR 6, 95% CI 1.4–23; P = .02) and self-extubation that occurred at night (OR 7, 95% CI 1.6–29; P = .01).
Subjects Who Self-Extubated and Required Re-Intubation vs No Re-Intubation
Discussion
In this study, we reported a self-extubation rate in the range of previously reported rates. We also found that self-extubation was more likely early in the course of respiratory failure, in subjects who were awake, and when the ETT was distant from the carina. We also found that re-intubation was more likely when self-extubation occurred at night and in the subjects with hypoxic respiratory failure. Understanding the burden of self-extubation is difficult because the incidence of self-extubation has been reported in numerous ways.7 The study by da Silva and Fonseca12 stressed the importance of standard reporting and recommend the use of the number of unplanned extubations per 100 mechanical ventilation days as the ideal metric. Our self-extubation event rate was 1.3 per 100 days of mechanical ventilation, which is closer to the lower end of reported rates, which range from 0.1 to 3.6 unplanned extubation per 100 days of mechanical ventilation.7,8,10,13
Being awake and calm, and being agitated, which covers the RASS score range from −1 to 3, have consistently been associated with an increased risk of unplanned extubation in surgical, medical, adult, and pediatric ICUs.4,7,11–14,17,22,28–30 Our result confirmed the findings of de Groot et al,7 of very high odds for unplanned extubation with agitation. The OR increased to 36, similar to the 31 reported by de Groot et al,7 if, in the logistical regression, the RASS score threshold was changed from > –2 to > –3. Sedation with benzodiazepines has been associated with a higher risk of developing delirium and self-extubation.7,30–32 This has been attributed to the paradoxical excitatory effect of benzodiazepines.7,33 A sedation awakening trial can lead to agitation and drug withdrawal, and can potentially lead to self-extubation.29,30 Girard et al34 reported an increase in the incidence of self-extubation after implementation of a daily sedation awakening trial, whereas Tanios et al28 showed that continuous sedation with daily interruption had a lower rate of unplanned extubations than did the intermittent protocol and no sedation group. Similar to what other studies have shown, we found no association between the type of sedation and self-extubation.35–37
One interesting finding in our study was the association of the position of the distal tip of the ETT from the carina with self-extubation. To our knowledge, only one previous study examined the association between unplanned extubation and the position of the ETT tip.18 The median distance observed by Thille et al18 (56 mm in the case subjects and 41 mm in the control subjects) was comparable with what we observed in our study (52 mm in cases and 45 mm in controls). Because the carina to vocal cords distance is known to be 13 cm,38 if the ETT tip is in a high position, then the ETT cuff will be located 1 to 2 cm below the vocal cords.
One possible explanation for self-extubation is that a higher positioned ETT requires less excursion for removal. A second possible explanation is that a cephalad position of the ETT cuff might trigger the Widdicombe cough “receptors,” a subset of vagal afferent nerves in the large airways (larynx, trachea, and main-stem bronchus),39 which thus leads to more-intense irritation. This could result in restlessness and deliberate removal of the ETT. A third explanation is that the tube's higher position in patients who self-extubated might be a consequence of the patients' own movement or movements associated with care. If these movements continue, then the ETT ultimately dislodges.
The subjects who self-extubated were on ventilation for 2 fewer days than the controls. One possible explanation is that they had not yet received enough sedation to control their agitation. The fact that 21 of the subjects (40%) who self-extubated were on no sedation but still required the application of restraints supports the fact that these subjects may be delirious and inadequately sedated. Another possible explanation is that patients who were frail and weaker were ventilated longer, but their movements were not sufficient to result in self-extubation.
In our study, ICU mortality was lower in the self-extubation group, a finding supported by other publications.2,7,13 The survival advantage is possibly attributable to the subjects who did not require re-intubation.2,7,13 Other studies found similar or higher ICU or hospital mortality in the subjects who had a self-extubation or unplanned extubation.3–5,10 Contrary to other studies, we did not find differences in the rates of self-extubation during the day versus the night shift or at the time of shift change.13,15,30,32 Interestingly, the subjects who self-extubated at night were older, more sedated, and sicker. It is possible that older patients are more likely to be sicker due to comorbidities and be delirious at night, which required increased use of sedation.
Re-intubation within 48 h was required in 30% of the subjects who self-extubated, with 50% of re-intubations occurring within 60 min and 80% within 12 h of the event. Other investigators reported similar or higher re-intubation rates, of up to 74%, with 90% being re-intubated within 12 h.3,4,7,10,21,26,28 In the study by Boulain,10 who studied self-extubation in a mixed ICU population, 61% required re-intubation up to 72 h after self-extubation, with the majority (68%) re-intubated within 2 h. We did not collect data on the reason for re-intubation but other investigators have shown that re-intubation is required in the majority (up to 91%) for respiratory distress and ventilatory failure.3,21,26 In the minority (8% to 19%), the reason for re-intubation was airway compromise.21,26,35
The subjects who required re-intubation were more sedated, had self-extubated at night, and were more likely to have been initially intubated for hypoxemic respiratory failure. We did not find any other demographic difference between those who required re-intubation and those who did not. Possible explanations for these findings are that, at night, patients are (1) more likely to be more sedated to facilitate care, (2) that less-experienced critical care fellows make the decision to re-intubate patients without exploring alternative treatments due to lack of confidence, (3) that nurses may pressure fellows to re-intubate the patient to facilitate care, or (4) that the disease process in patients who required initial intubation for hypoxemic respiratory failure had not reversed yet.
Other investigators found that subjects who required re-intubation were sicker, older, men, had higher oxygen requirements or PEEP, or required a certain mode of mechanical ventilation mode.7,22,23,25,26 The rates of re-intubation were also found to be lower in subjects undergoing a weaning trial, which is logical because those patients were deemed ready for exubation.3,40 Some investigators reported a higher risk of death due to self-extubation, especially in subjects who required re-intubation.2,4,22 Similar to Bouza et al,13 we found no association between mortality and re-intubation. In contrast to other reports, none of our subjects died directly as a consequence of re-intubation.10,17,29
Our study design had a few advantages. The case-control design is the most efficient to study rare conditions. We are confident that we did not miss any cases of self-extubation. Therefore, our study was a true sample of consecutive subjects who had a self-extubation event. The period of data collection spanned > 2 years, therefore, was minimally influenced by seasonal or transient changes in staffing and management. Although we were unable to obtain a control sample of equal size, they were similar to the case subjects in baseline characteristics.
Our study had few limitations. Although the cases were identified prospectively, the data were extracted retrospectively and, therefore, relied on the documentation by clinicians. The RASS score was recorded hourly by the nurse, we, therefore, could not ascertain it to reflect the RASS score at the time of the self-extubation event. It is unlikely though, that the RASS score changed significantly and suddenly from the time of documentation to the time of the event. Another limitation was that we were unaware of the head position at the time of the chest radiographs. It is well known that neck flexion advances the ETT toward the carina, whereas neck extension moves the tube away from the carina.41 If sedated, patients are less likely than awake patients to have their neck extended at the time of the chest radiographs, the difference in the ETT tip to carina distance might be a consequence of wakefulness.
This would only be possible by a prospective design in which the distance would be measured in every patient on mechanical ventilation, which would ensure a neutral head position at the time of obtaining the chest image until self-extubation occurs. Similarly, we used the chest radiograph before the self-extubation, so the true position of the ETT immediately before self-extubation might have been different in some cases. Another limitation was that our study was a single center and included subjects in the medical ICU only. Therefore, the findings might not apply to patients in other specialty ICUs.
Of the factors associated with self-extubation in our study, agitation is probably the one that is mechanistic. A high position of the ETT can be either a cause of agitation, a consequence of agitation, or a facilitator for self-extubation. As for the timing of self-extubation in our study, it was probably a consequence of these subjects not being adequately sedated.
Conclusions
It is likely that self-extubation is unavoidable in some patients. Our study showed that, in the era of reduced use of sedatives in the ICU, clinicians must be vigilant of the risk of self-extubation in the patients who are agitated on the first 2 days of mechanical ventilation, with the tip of the ETT being far from the carina. Further, patients who self-extubate should be closely monitored for at least 12 h, especially those who required mechanical ventilation support for hypoxemic respiratory failure.
Footnotes
- Correspondence: Renaud M Gueret MD, Department of Pulmonary, Critical Care and Sleep. John H. Stroger Hospital of Cook County, 1950 W Polk Street, Chicago, IL 60612. E-mail: rgueret{at}cookcountyhhs.org
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.