

Abstract
BACKGROUND: For patients with chronic respiratory failure or sleep breathing disorders, adaptation and training are important prerequisites for successful home noninvasive ventilation (NIV) and CPAP. In Europe, management of NIV/CPAP is sometimes performed by physiotherapists (PTs). However, their role within the NIV/CPAP management team is not well defined.
OBJECTIVE: To describe the implementation of a standardized protocol to NIV adaptation for patients with chronic respiratory disease. Secondary outcomes were to evaluate the PT's role and time-consumption.
METHODS: We enrolled 201 patients with chronic respiratory disease, referred to the cardiopulmonary rehabilitation service (CPRS). Anthropometric and clinical data, adaptation sessions, ventilator typology, side effects, plus activities conducted by the CPRS were recorded. The time spent on a single protocol task plus total time spent on the entire management procedure for NIV/CPAP adaptation was also documented.
RESULTS: Adaptation to NIV/CPAP was completed in 8.2 ± 3.2 sessions, lasting 17.2 ± 15.4 min/session. Total CPRS activity included 61% adaptation procedures, 22% educational sessions, 8% evaluation, 7% monitoring and follow-up, and 2% administrative activities. CPRS time-consumption per patient was 149.5 ± 113.7 min. Total CPRS time-consumption was 28,870 min, corresponding to 1.52 hours/working day and 21% of total PT daily activity. After protocol implementation, PTs were able to cover 65% and 35% of the time devoted to ventilation procedures typically carried out by physicians and nurses, respectively. Amyotrophic lateral sclerosis/neuromuscular patients required more time for adaptation and education, compared to patients with obstructive sleep apnea syndrome (P < .001) and pulmonary restrictive disease (P < .001).
CONCLUSIONS: Our study has demonstrated that the PTs can play a key role in the respiratory care management of patients with chronic respiratory disease and sleep breathing disorders with neuromuscular diseases requiring higher time consumption, and the inclusion of PTs in the NIV/CPAP management procedure reduces the time spent by other health professionals. The cost effectiveness of this management needs to be verified in larger clinical trial settings.
Introduction
There is increasing evidence in support of noninvasive ventilation (NIV) in chronic respiratory failure.1–4 Furthermore, there is increased frequency for the use of CPAP treatment, indicated for patients with diagnosed obstructive sleep apnea syndrome (OSAS) or other sleep-related disorders.5–7
The prevalence of chronic respiratory failure with indication for home mechanical ventilation in Europe is 6.6 per 100.000 patients, while in Italy it is 3.9 per 100.000 patients.8 There are no published data on the number of CPAP users in Europe, but the literature suggests that the prevalence of patients with sleep breathing disorders is about 3–7% of the adult population, with a strong variability in relation to sex, age, body weight, and comorbidities.9 For successful implementation of NIV or CPAP therapy a period of adjustment and education about the self-use of ventilatory prosthesis is important.10
In the United States, respiratory therapists (RTs) usually manage the NIV/CPAP adaptation in emergency or respiratory clinics and subsequent execution of respiratory care therapeutic treatments.11 In Europe, RT is not a recognized profession, while physiotherapists (PTs) who have additional specialized training in respiratory care are usually involved in respiratory departments. However, there may be important differences in tasks and responsibilities among different countries and hospitals.12,13
European surveys have demonstrated the feasibility of implementing protocols that include PTs as an integral part of a cardiopulmonary rehabilitation service (CPRS) team.12,13 In Italy, the assessment, education, and care for patients with pulmonary disorders, in acute and chronic settings, are managed mainly by pulmonologists and nurses. PTs may be involved as part of the dedicated care team in tasks related to monitoring a patient's physiological responses to pharmacologic therapies (eg, vital signs, oximetry), to supervise exercise training sessions, and to perform airways clearance techniques. However, in a few specialized hospitals, some PTs are trained to perform tasks that fall outside their traditional role. They perform more specialized activities such as sleep-related disorders care, pulmonary function test execution, or mechanical ventilation administration. Despite this, the role of PT in the management of patients with ventilatory disorders is still undefined, unknown, and debated. For these reasons, the writing of a management procedure that includes a PT with defined roles is needed.
The main aim of this prospective study was to report the results of the implementation of a standardized protocol to NIV adaptation for patients with chronic respiratory disease. We also describe the role and time-consumption by PTs in the multidisciplinary team.
QUICK LOOK
Current knowledge
Patient adaptation to noninvasive ventilation (NIV) is an important component of NIV success. During the first 1–2 hours of NIV, clinician time with the patient is intensive and leads to adaptation success.
What this paper contributes to our knowledge
In Italy, physiotherapists trained in respiratory care play a key role during NIV adaptation in patients with chronic respiratory failure and sleep breathing disorders requiring more intensive treatment. The cost effectiveness of this approach needs study.
Methods
The study was conducted at the Fondazione Salvatore Maugeri Institute, a rehabilitative hospital located in Lumezzane, Brescia, Italy, and was designed and performed by its CPRS, which is a professional service for cardiac and pulmonary rehabilitation for hospitalized patients, out-patients, and home patients.
The institute employs 6 PTs (with a 3-year degree course) and a senior PT coordinator. (with a 5-year degree). Each PT has attended several medical meetings and at least 2 specific courses on NIV, physiopathology applied on mechanical ventilation, sleep, monitoring, and chronic respiratory failure. All PTs also serve as tutors during the required internship on respiratory diseases for students attending the Degree in Physiotherapy at the University of Brescia, Italy. The CPRS carries out services mostly for 3 departments: Pulmonary Rehabilitation Division (which includes a weaning center for critical patients), Cardiac Rehabilitation, and Telemedicine Services. The main activities performed by PTs are supervision and management of endurance training, muscle training, airways clearance, health education, and lung expansion for patients undergoing pulmonary and cardiac rehabilitation. The study was approved by our local technical-scientific committee. All subjects gave their informed consent to participate.
Subjects
From June 2009 to September 2010, consecutive chronic respiratory disease (COPD, neuromuscular, amyotrophic lateral sclerosis [ALS], and restrictive disorders) or sleep breathing disorders (OSAS) patients referred to CPRS by a pulmonologist for NIV/CPAP adaptation and follow-up were recruited. All subjects were admitted to the institute for rehabilitation purposes and were treated as both in-patients or out-patients.
Management Procedure for NIV/CPAP Adaptation
On April 2009, a new formal management procedure for NIV/CPAP adaptation was prepared by 2 pulmonologists from the Pulmonary Rehabilitation Division and 2 PTs from the CPRS. The protocol was written according to literature reports, expert consensus, and clinical personnel experience. A summary of the NIV/CPAP management procedure protocol is shown in the supplementary materials at http://www.rcjournal.com.5,14–16
Prior to April 2009, our unit used an “operative instruction” on adaptation for NIV/CPAP, with structured aims and procedures formulated by 2 clinical professions (nurse and physician). The present study describes the implementation of the former operative instruction inclusive of the new profession (ie, PT), thus remodeling the previous operational procedures.
Before the implementation of the protocol, all PTs underwent 2 sessions of training consisting of two 1-hour educational lectures to explain the details of the protocol. In addition, each PT underwent 15 days of full time apprenticeship conducted by pulmonologists. These sessions were designed to provide the PTs an opportunity to learn how to manage the definitive application of the protocol. A final practical and comprehensive test was given to establish appropriate standards of skill and knowledge.
The NIV/CPAP management procedure team was composed of 8 pulmonologists, 7 PTs, and 20 ward nurses. The NIV/CPAP management procedure setting decision was performed in relation to the patient's disease and on an individual needs basis. Details of this specific strategy and mandatory items pursued are shown in the supplementary materials at http://www.rcjournal.com.
Measures
During the study period, the following data were recorded in an electronic database. From each subject we collected anthropometric data (age, sex, caregiver availability), diagnosis, admission regimen, number of sessions for adaptation, ventilator typology, side effects during NIV adaptation, NIV/CPAP comfort by a subjective score (0 = minimum comfort to 10 = maximum comfort), and subject's acceptance of the physiotherapy. For the CPRS we collected type and number of services performed (in-patient and out-patient adaptation sessions, educational sessions, sleep cardiopulmonary complete monitoring delivery, compilation of prescriptions, administrative activities), time spent by PT (in minutes) for each subject adaptation and for each performance.
Statistical Analysis
All measures are described as mean ± SD. A statistical analysis by one-way analysis of variance was performed to detect significant variations of total time spent in the diagnosis groups. Then a post hoc analysis to evaluate significant differences between groups was administered by a Student t test with Bonferroni adjustment. A P value < .05 was considered statistically significant.
Results
During the 16 months of activity, 201 patients with chronic respiratory diseases were referred to the CPRS for NIV/CPAP adaptation and revaluation and reinforcement visits. Table 1 shows the anthropometric and clinical data after CPRS referral. The in-hospital subjects were in hospital for 27 ± 4 days. The out-patients attended 24 ± 2 rehabilitative sessions.
Anthropometric and Clinical Data
Of the 201 subjects, 166 (82.6%) were submitted to home mechanical ventilation (invasive or noninvasive) or CPAP. According to diagnoses, the 2 more common ventilation typologies proposed were CPAP (51.8%) and bi-level positive airway pressure (36.7%) in spontaneous temporized mode. During the NIV/CPAP management procedure, PTs spent a mean 17.2 ± 15.4 min for each session dedicated to a single subject. No subject abandoned the training sessions provided by the PTs, and there were no clinical sequelae requiring additional intervention. Total time spent according to diagnosis is shown in Figure 1. A significant difference among diagnosis groups was detected (Fisher test = 0.000). A post hoc analysis described a higher time spent with subjects with ALS/neuromuscular diseases, compared to those with OSAS (P < .001) or pulmonary restrictive disease (P < .001).
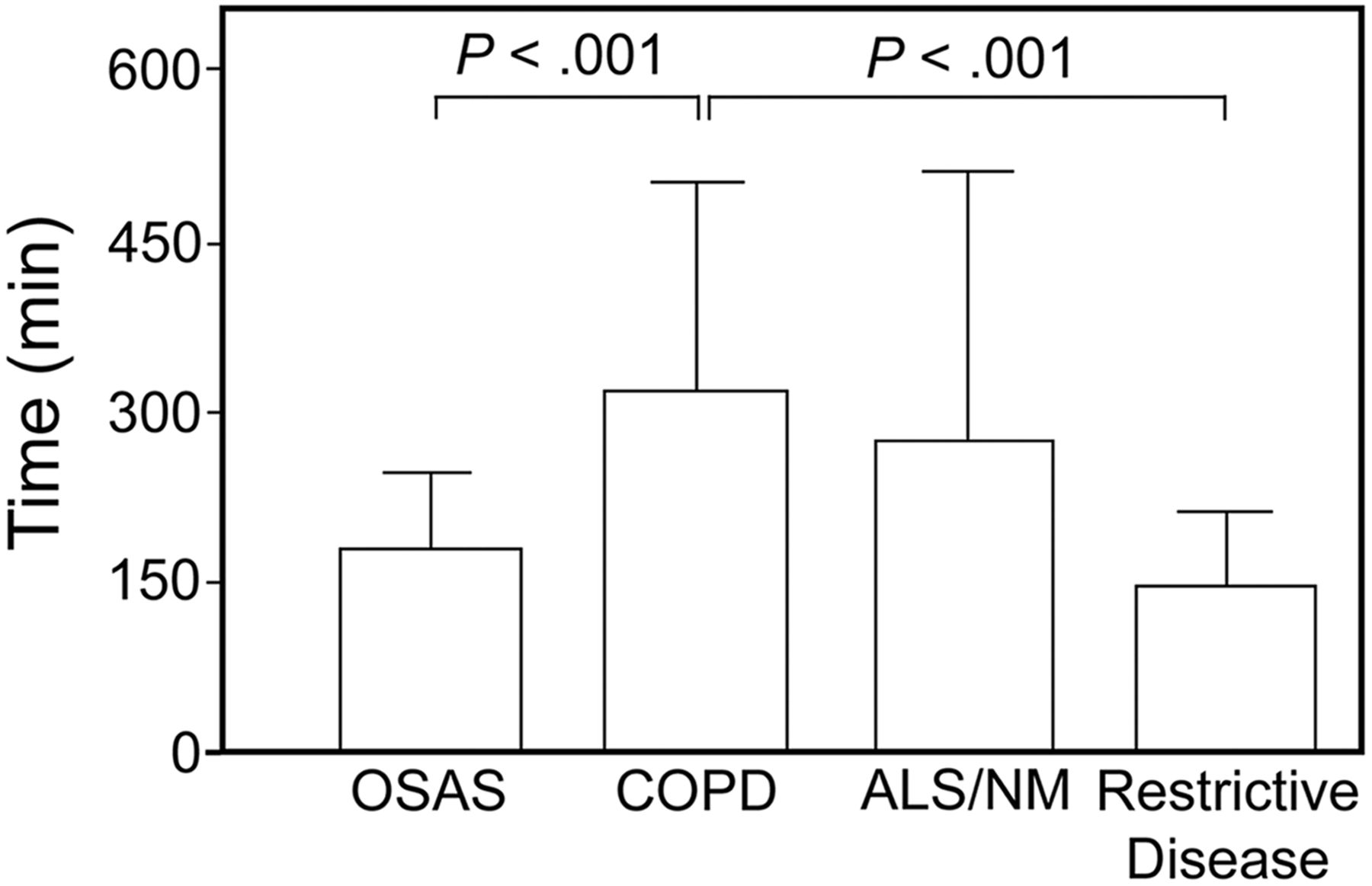
Minutes spent by the physiotherapists in 4 disease categories. OSAS = obstructive sleep apnea syndrome. ALS = amyotrophic lateral sclerosis. NM = neuromuscular.
NIV/CPAP adaptation was completed in a mean 8.2 ± 3.2 sessions (range 2–16 sessions). NIV/CPAP revaluation in subjects adapted to NIV previously required a mean 2.93 ± 2.10 sessions (range 1–9 sessions). A high level of comfort (8 ± 2, on a scale of 1–10, with 10 being the highest satisfaction) during NIV/CPAP adaptation was expressed by the subjects.
CPRS Results
Activities.
In the study period a total of 396 activities were delivered by CPRS. Table 2 shows the mean time spent for each session during the entire protocol. Of the 117 NIV/CPAP new adaptations performed, 114 were completed successfully, while only 3 adaptations failed: 2 were switched to invasive ventilation (1.0%), and one subject refused mechanical ventilation. We conducted 48 revaluations/reinforcement in subjects who were previously NIV adapted. We performed 28 prescriptive bureaucracy compilations, 71 sleep cardiopulmonary complete monitorings, and 132 in-patient educational sessions.
Activities Time Per Subject During the Entire Protocol
Time-Consumption.
During the entire study period, the CPRS spent a total time of 28,870 min (481 h) on NIV/CPAP activities. Figure 2 shows the distribution (%) and minutes dedicated to the different PT activities.
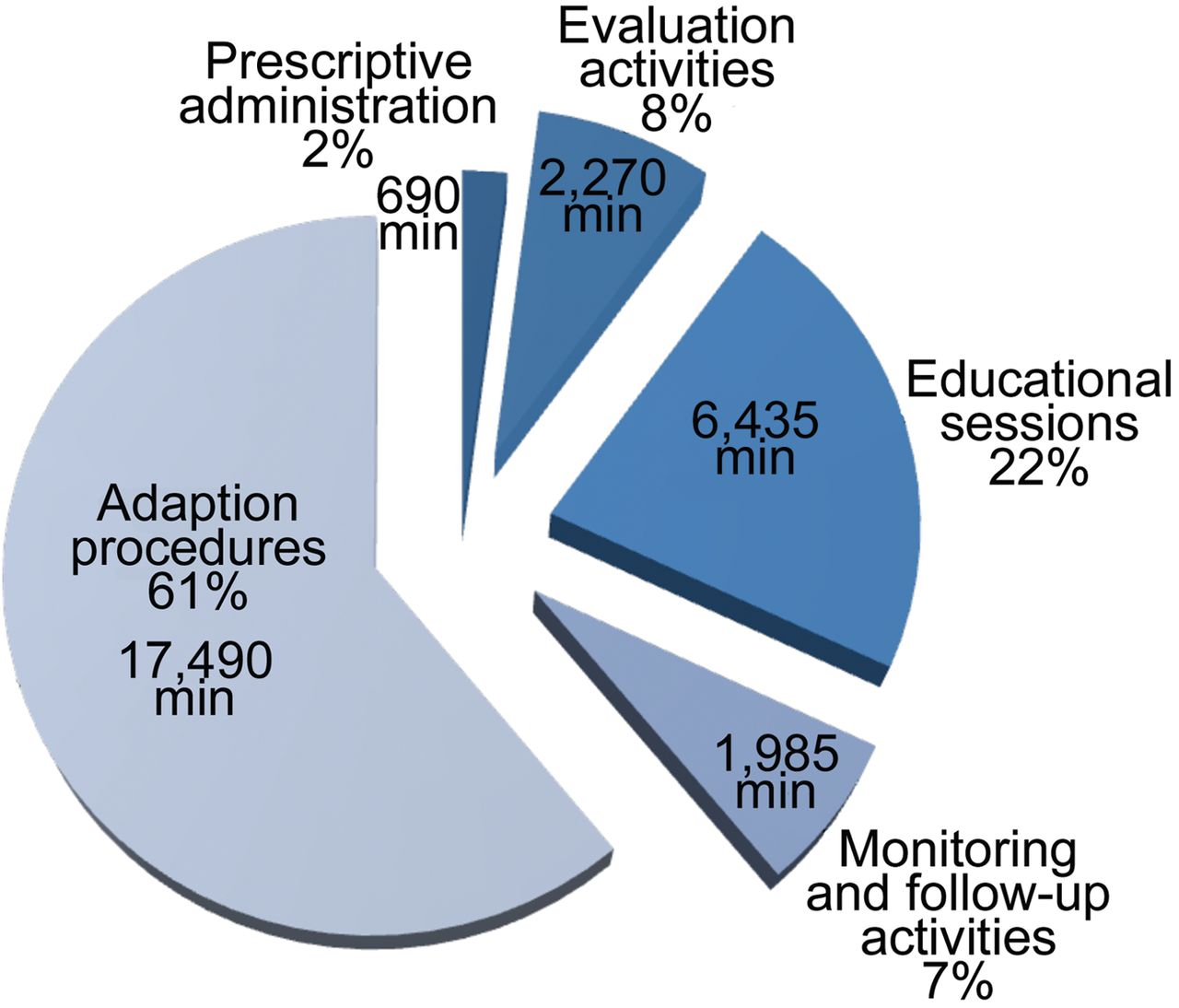
Time breakdown of the physiotherapists' noninvasive ventilation activities.
The total daily CPRS time-consumption corresponded to approximately 1.52 hour per working day, and involved the care of 6 to 7 subjects. The work load corresponds to 21% of total time involvement by the PT (on the basis of 7.12 h/d for 6 d a week). For the first adaptation the total mean time spent by CPRS on a subject was 149.5 ± 113.7 min (range 10–840 min).
Before the introduction of the formal NIV/CPAP management procedure protocol, the activities were divided between nurses and pulmonologists as follows: the nurses spent 35% of their time for activities such as diagnostic/assessment (8%), monitoring (4%), and education (23%), while the physicians dedicated 65% of the time to adaptation and administrative activities. The time spent by PTs for the NIV protocol was summed up to that of a broad rehabilitative program that required a mean time of 500 min/week for each subject.
Discussion
Our study showed that NIV or CPAP adaptation and its organizational procedures can be managed by a PT trained in respiratory care. Each new subject adapted to NIV requires < 3 hours of PT time (about 20 min/session) to be discharged with mechanical ventilation. The introduction of the PT profession in the NIV adaptation procedures and educational activities saves time for other health professionals.
The clinical practice of European PTs, in particular in the field of protocols and interventions, is emerging.13 Protocols are based on consensus, standardized care plan, and flow charts, according to objective measurable variables to allocate a performance and to reduce the time to be spent on it.17,18 Protocols are used as a strategy to lower the occurrence of medical errors, omissions, and delays.17,18 Protocols may reduce conflicts between team members, improve outcomes, decrease costs, and increase educational efforts.17,18 The development of protocols and guidelines for NIV/CPAP management is recommended in order to clarify the roles of each professional19 and to increase greater efficiency during NIV application.20
To our knowledge, no data from Italy are available on the PT's role in NIV/CPAP management. This lack may be due to differences in training courses offered to PTs, or to differences in hospital and health service organizations, compared to other countries. However, in Italy, in some acute units and rehabilitative institutes such as ours, PTs must develop skills that fall outside their traditional role, becoming involved in more specialized areas such as mechanical ventilation administration or sleep related disorder care.
Our study is consistent with existing literature regarding the role of each professional in the NIV management multidisciplinary team. Previous studies have pointed out that the role of the RT is mainly concentrated on ventilator and mask choice, the ventilator setup and the patient educational sessions,19–22 while the physician's role is mainly related to NIV indication.20 The nursing staff is usually identified as responsible for nocturnal monitoring and for catching problems and side effects such as facial skin damage.22,23 The PT has been chosen for skills in terms of scientific background, competence in NIV and cough-assist techniques, and educational attitude. After the application of this new NIV/CPAP management procedure, all subjects completed NIV adaptation with a good level of adherence and comfort.
During the entire study, no clinical situations directly related to PT care were recorded, and there was no increase in time expenditure for NIV adaptation. The effect of the introduction of RTs in NIV management teams has been examined in only one study, by Kareus et al.24 These authors demonstrated an improvement in NIV tolerance after RT involvement, increasing patient tolerance to NIV by about 51%. These data are in keeping with our results, since we found only one case of rejection of the proposed treatment. Results from 2 studies12,20 are in keeping with the finding that for NIV poor adherence is a major issue, which may have been compounded by the lack of medical and non-medical staff training and the absence of an RT. The availability of sufficient PTs, the presence of experienced staff, and the frequent NIV use in our department have undoubtedly facilitated the implementation of our NIV/CPAP procedures.
The majority of our subjects were treated as in-patients (77.6%): the reason for this depended on the severity of disease in our subjects and the rehabilitative mission of our hospital, which admits patients, not only to adapt to NIV, but also for stabilization after an acute relapse or hospitalization. In-patients receive multidisciplinary evaluation, education, drugs stabilization, effort training, muscle reconditioning, nutritional assessment, and attention to social problems. Other factors are difficult discharge, rural geographical location and difficulty in reaching a hospital, and local health organizational reimbursement. Out-patient setting was proposed in 22.4% of the subjects, according to stability of the subject and subject consent.
An important finding from our study, relates to the time consumption by the PT. There is lack of consensus on time spent on adaptation activities. Chatwin et al16 reported a mean of 4 days (range 2–7 d) for the adaptation of in-patients with chronic restrictive disease, with a time-consumption of 2.85 hours per day. Unlike our results, a review of the study by Leger et al,10 which included chronic patients, reported that, when necessary, a mean of 3–4 hospitalization days to complete the long-term NIV adaptation process was mandatory. Both studies are divergent with our findings, and the differences could be explained by the holistic rehabilitative approach used by our department and the different clinical characteristics of our subjects. Our subjects were stable and non-critical, but highly complex, elderly, and had comorbidities, including bulbar muscle weakness or dysphagia, disability for several years, and long history of frequent exacerbations and ICU admissions.
Our data are in keeping with findings from Lujan et al.25 Their prospective observational study investigated a population of chronic patients (neuromuscular, restrictive disease or COPD, not OSAS) similar to half of our subject group. These authors verified efficacy and efficiency of an NIV adaptation protocol conducted in about 5.5 out-patient sessions, compared to the usual average hospital adaptation time of 7 days.25
Moreover, an interesting aspect of our work is that the ALS/neuromuscular subjects required more time during adaptation and education, compared to those with OSAS and pulmonary restrictive disease. This is not surprising, since ALS/neuromuscular was the subgroup with the higher adaptation efforts due to their clinical complexity and dependence involving caregivers at discharge. We should also emphasize that mean time spent by the PT during the subject's entire hospitalization to complete the NIV or CPAP adaptation was less than 3 hours, distributed over a mean of 8 sessions. Our setting differs from clinical practice guidelines in that, after a decision to start, the protocol prescribes a specific series of behaviors or changes in treatment, without the requirement of further clinician input.18 Although we lack specific data on the PTs' time-efficiency during the time course of the protocol, we have noted a learning effect due to higher experience and training, as demonstrated by the decrease in the physicians' face to face visits, second opinion telephone calls, and inappropriate choice of devices, during the last months of the protocol application, compared to the starting months.
The introduction of a PT in the process/management of NIV/CPAP adaptation resulted in a decrease of time-consumption for other health professionals dedicated to the same protocol. In particular, pulmonologists decreased their time dedicated to activities such as ventilation management by 65%, and nurses by 35%. The consequent cost saving and/or economic rationalization in NIV/CPAP management could be very important for overall health care reimbursements. In order to verify cost/benefit outcomes, these data must be confirmed by large detailed studies.
From our data it must be stressed that PTs are not presented as an alternative to nurse and pulmonologist involvement, but, instead, they are complementary and synergic. Addition of a further professional to the team may optimize delivery of service
Another important key point is that our data were obtained from a single hospital in Italy. Similar outcomes might not be seen in other hospitals and in other countries. For example, in hospitals in North America, RTs are trained to initiate and monitor NIV. In countries or hospitals where RTs are not available, our protocol might be useful to consider. However, specialized training must be introduced to PTs who are being considered for such role. The lack of comparison with historical data or among different populations or among different health professionals is an important limitation of the study. Another major limitation in our work is related to the lack of long-term NIV/CPAP adherence outcomes. Our results would be more meaningful if comparative data with a randomized study or retrospective data prior to PT involvement would have been available. Another limitation is that we cannot gauge how much the implementation of our protocol per se improved care efficiency.
Conclusions
Our study has demonstrated that a PT trained in respiratory care can play a key role during NIV adaptation in patients with chronic respiratory disease and sleep breathing disorders, with neuromuscular diseases requiring more time consumption. There is the possibility to reallocate team member participation among various professions, which may lead to cost savings. However, the cost effectiveness of this approach needs to be verified in large clinical trials.
Acknowledgments
We thank Dr Alessandro Bettini for English editing assistance. For their collaboration during the protocol we thank Debora Trainini PT, Manuela Saleri PT, Roberta Peroni PT, Ilaria Speltoni PT, George Fokom Aubin PT, Mariarosa Guerini RN, Roberto Porta MD, Luca Barbano MD, Luca Bianchi MD, Domenico Fiorenza MD, Enrica Bertella MD, Sonia Gilè MD, and Katia Foglio MD.
Footnotes
- Correspondence: Mara Paneroni PT, Fondazione Salvatore Maugeri, Istituto di Ricovero e Cura a Carattere Scientifico, Pneumologia Riabilitativa, Via G Mazzini 129-25065, Lumezzane, Brescia, Italy. E-mail: mara.paneroni{at}fsm.it.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}