

Abstract
BACKGROUND: Infant respiratory distress remains a significant problem worldwide, leading to more than one million neonatal deaths each year. The cost, maintenance, energy, and personnel required to implement ventilators have proven to be a barrier in many resource-limited settings. To address these barriers, a nonelectric bubble noninvasive positive pressure ventilation (NIV) device was developed. This study aims to benchmark the performance of this bubble NIV device against commercially available ventilators.
METHODS: The delivered pressure waveforms and tidal volumes of the bubble NIV device were compared with those of 2 conventional ventilators (ie, Dräger Evita Infinity V500 and Hamilton G5) at the following pressure settings: 8/5, 12/5, and 15/5 cm H2O. To simulate the lung mechanics of an infant in respiratory distress, tests were conducted on the IngMar ASL 5000 Test Lung simulator. Resistance was set at 100 cm H2O/L/s, and compliance was tested at 0.5, 1.0, and 2.0 mL/cm H2O to simulate 3 different patients.
RESULTS: The delivered pressure waveforms and compliance curves of the bubble NIV device are similar to those of the Hamilton and Dräger ventilators. The mean ± SD differences between delivered versus set pressure gradient (ie, the difference between the high delivered pressure and the low delivered pressure) for each treatment modality across the various values of compliance were −2 ± 8% for the bubble NIV device, 3 ± 4% for the Dräger ventilator, and 7 ± 10% for the Hamilton ventilator.
CONCLUSIONS: The similarity of pressure waveforms and delivered tidal volumes in this simulated clinical scenario suggest that the bubble NIV device may provide comparable efficacy compared with traditional ventilator treatment for a range of patients. This may provide clinicians in resource-limited settings with an additional, simple, nonelectric treatment modality for the management of infant respiratory distress.
Introduction
Infant respiratory distress remains a significant problem worldwide, leading to more than one million neonatal deaths each year.1 Leading etiologies include respiratory distress syndrome, pneumonia, transient tachypnea of the newborn, meconium aspiration syndrome, and apnea. There has been a growing interest in noninvasive ventilation modalities such as CPAP and noninvasive positive pressure ventilation (NIV) to decrease the incidence of complications associated with invasive mechanical ventilation such as bronchopulmonary dysplasia.2
Bubble CPAP, a simple mechanism of noninvasive respiratory support, has been successfully implemented across low- and high-resource settings.3 For sicker infants, NIV can provide additional respiratory support and decrease the work of breathing.4 The cost, maintenance, electrical demand, and personnel required to implement ventilator-driven NIV have proven to be a barrier in many resource-limited settings. We developed a nonelectric bubble NIV device that can be implemented in locations presently using bubble CPAP.
We sought to benchmark the performance of this bubble NIV device against conventional ventilator-driven NIV over a range of commonly prescribed pressure settings (8/5, 12/5, and 15/5 cm H2O). Resistance was set at 100 cm H2O/L/s, and compliance was set at 0.5, 1.0, and 2.0 mL/cm H2O to simulate 3 distinct pathophysiologic states of respiratory distress. We used the Hamilton G5 ventilator (Hamilton Medical, Bonaduz, Switzerland) and the Evita Infinity V500 ventilator (Dräger, Lubeck, Germany). Tests were completed on the ASL 5000 Test Lung Simulator (IngMar Medical, Pittsburgh, Pennsylvania), and measured outputs included delivered pressure waveform and tidal volumes.
QUICK LOOK
Current knowledge
Bubble CPAP has been effectively used to treat infants in respiratory distress across low- and high-resource settings. Noninvasive ventilation (NIV) can provide additional support and decrease the work of breathing. Currently, barriers of cost, complexity, and power requirements prevent many low-resource settings from implementing NIV.
What this paper contributes to our knowledge
In 3 models of infant respiratory distress (ie, transient tachypnea of the newborn, pneumonia, and respiratory distress syndrome) on an infant lung simulator, a bubble NIV device delivered pressure waveforms and volumes comparable to those delivered with conventional ventilators.
Methods
Description of Ventilation Equipment
The bubble NIV device was designed to provide time-cycled, pressure-limited respiratory support to spontaneously breathing infants using a modified bubble CPAP circuit. The device is powered by blended oxygen and air delivered to the circuit. The bubble NIV device utilizes a float, which collects bubbles, rises due to buoyancy, vents the bubbles, and sinks due to gravity. A bi-level pressure waveform is generated through a connected sleeve, which changes the effective length of the water column by alternately occluding and uncovering the submerged holes. When the float is high, delivered pressure is high, and when the float is low, delivered pressure is low (Fig. 1). The cycling frequency, peak pressure, and baseline pressures are set independently. Increasing the air flow decreases the time needed to collect bubbles, increasing the number of cycles per minute. The low level of pressure is set by the depth of water, as in the case of bubble CPAP. The high level of pressure is set by the value of the pressure relief valve.
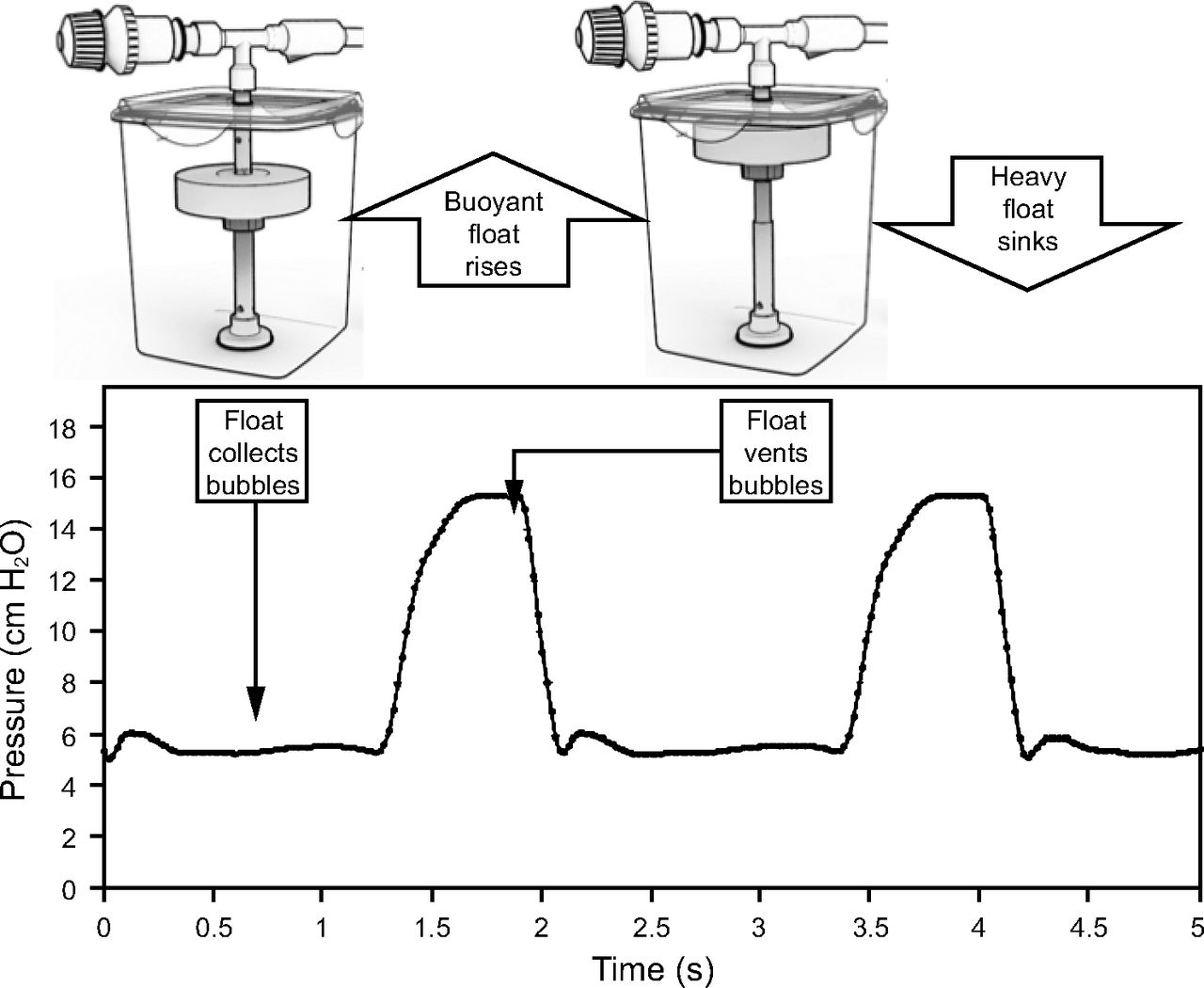
Bubble noninvasive ventilation functional design.
Experimental Setup
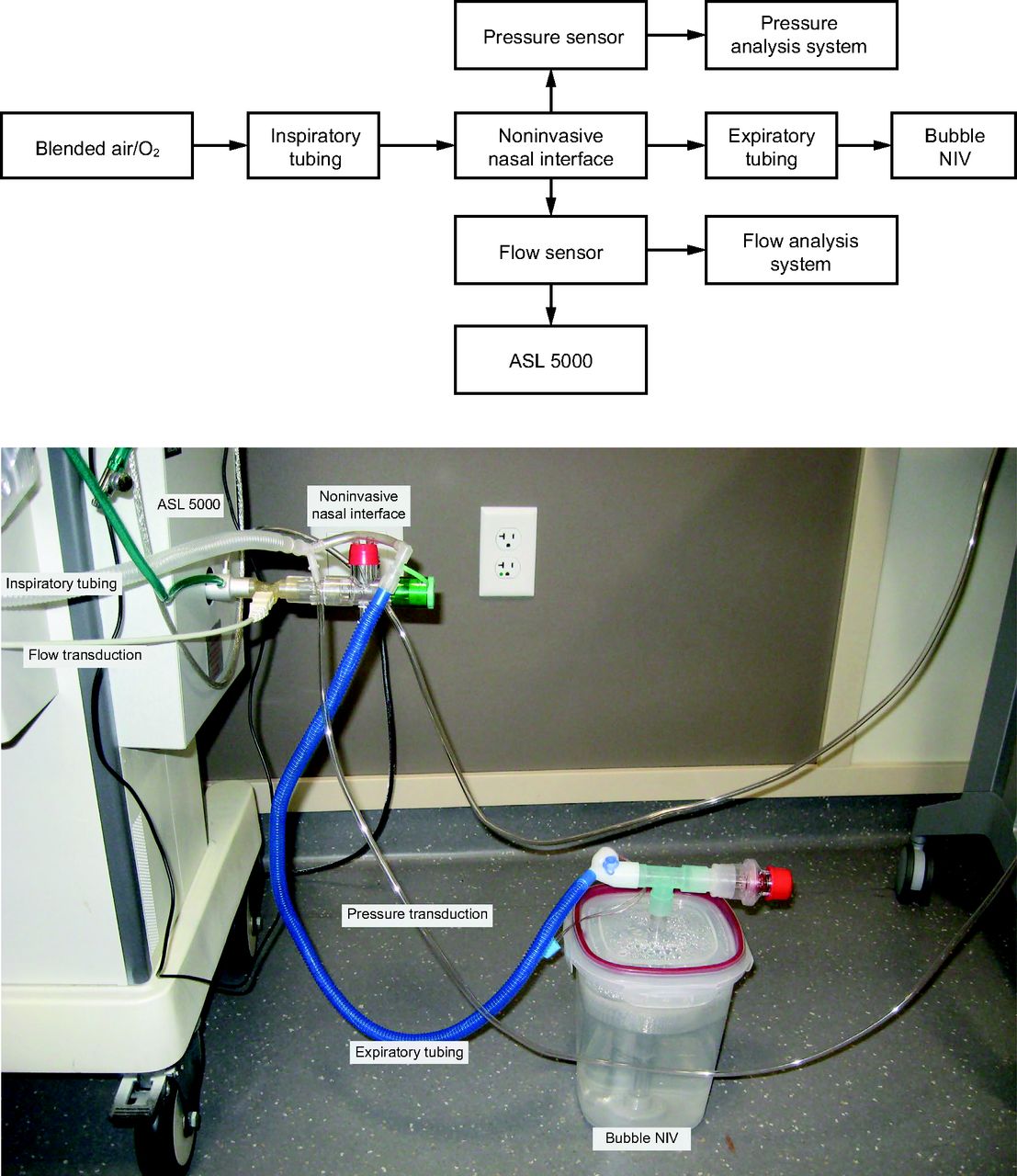
Compressed air from a flow meter was connected to a respiratory circuit, which was connected by a T tube connection to a test lung (Ingmar ASL 5000) through a nasal prong adapter. The inspiratory limb of the circuit was connected to a Dräger hot wire anemometer flow sensor and a digital pressure transducer (details below) placed proximal to the test lung. The expiratory limb was then connected to the bubble CPAP center tube, which had been modified to house the bubble NIV (Fig. 2). For subsequent tests with the Dräger and Hamilton ventilators, the inspiratory and expiratory limbs of the circuit were connected to the ventilator.

Bubble noninvasive ventilation (NIV) experimental setup.
Experimental Procedure
To compare the performance of the bubble NIV device with the performance of the 2 reference ventilators (Dräger Evita Infinity V500, Hamilton G5), the following experiments were performed on the ASL 5000 Lung Simulator. To simulate 3 patient profiles, the following settings for compliance were used: 0.5, 1.0, and 2.0 mL/cm H2O. The compliance setting of 0.5 mL/cm H2O was selected to represent an infant with respiratory distress syndrome.5 The compliance setting of 1.0 mL/cm H2O was selected to represent an infant with pneumonia.5 The compliance setting of 2.0 mL/cm H2O was selected to represent an infant with transient tachypnea of the newborn (ie, relatively healthy lungs).5 Airway resistance was fixed at 100 cm H2O/L/s.
For each compliance setting, performance was studied at 3 pressure settings: 8/5, 12/5, and 15/5 cm H2O at a cycling rate of 30 cycles/minute. Each experiment was initially completed on the bubble NIV device and subsequently repeated on the Dräger and Hamilton ventilators, for a total of 3 ventilators with 3 compliance settings at 3 pressure settings for a total of 27 experiments. A minimum of 30 s of data were acquired for each experiment, corresponding to at least 11 stabilized breaths; this time duration was selected based on preliminary tests, which showed minimal changes in the delivered pressures and volumes waveforms for each ventilator over time. Delivered tidal volumes and pressure waveforms, including average high and low pressures, time at high pressure, and cycling frequency, were measured.
Tidal volume was measured using the ASL 5000, with values from the Dräger flow sensor providing confirmation. Pressures were measured at 50 Hz with a digital pressure transducer (MS4515DO, TE Connectivity, Schaffhausen, Switzerland) and in-house data acquisition software. Prior to the start of the experiment, the in-house pressure measurement system was verified with a water manometer.
Statistical Analysis
The start of a pressure cycle, as well as high and low pressure designations for the cycle, were identified by tracking when the pressure trace crossed the mean pressure. For that purpose, a 3-Hz low-pass digital Butterworth filter was applied to the raw pressure signal. Filtering ensured that signal noise did not misidentify the time. Means, maximums, and minimums were computed for each phase on the filtered pressure signal. Statistical analyses were completed with R 3.6.0 software (Vienna, Austria).
Results
The waveforms of delivered pressure for each ventilator at each pressure setting and level of lung compliance are displayed in Figures 3–5. Each figure shows 10 s of the delivered pressure waveform. The times are shifted to align at the start of the first plotted cycle.
The compliance setting of 0.5 mL/cm H2O represented an infant with respiratory distress syndrome. The delivered pressure waveforms at pressure settings of 8/5, 12/5, and 15/5 cm H2O are shown in Figure 3. The compliance setting of 1.0 mL/cm H2O represented an infant with pneumonia. The delivered pressure waveforms at pressure settings of 8/5, 12/5, and 15/5 cm H2O are shown in Figure 4. The compliance setting of 2.0 mL/cm H2O represented an infant with transient tachypnea of the newborn. The delivered pressure waveforms at pressure settings of 8/5, 12/5, and 15/5 cm H2O are shown in Figure 5.

Delivered pressure waveform to the IngMar ASL 5000 Lung simulator (compliance = 0.5 mL/cm H2O, resistance = 100 cm H2O/L/s) by bubble NIV versus Dräger versus Hamilton at various pressure settings: (A) 8/5 cm H2O, (B) 12/5 cm H2O, (C) 15/5 cm H2O.

Delivered pressure waveform to the IngMar ASL 5000 Lung simulator (compliance = 1.0 mL/cm H2O, resistance = 100 cm H2O/L/s) by bubble NIV versus Dräger versus Hamilton at various pressure settings: (A) 8/5 cm H2O, (B) 12/5 cm H2O, (C) 15/5 cm H2O.

Delivered pressure waveform to the IngMar ASL 5000 Lung simulator (compliance = 2.0 mL/cm H2O, resistance = 100 cm H2O/L/s) by bubble NIV versus Dräger versus Hamilton at various pressure settings: (A) 8/5 cm H2O, (B) 12/5 cm H2O, (C) 15/5 cm H2O.
The mean ± SD differences between delivered versus set pressure gradient = (Pdelivered high – Pdelivered low)/(Pset high – Pset low) for each treatment modality across the 3 values of compliance and 3 settings of pressure were −2 ± 8% for the bubble NIV device, 3 ± 4% for the Dräger ventilator, and 7 ± 10% for the Hamilton ventilator.
Volume Exchange
Comparable volume exchange was achieved at each level of volume as evidenced by the compliance curves at 15/5 cm H2O (Fig. 6) and 12/5 cm H2O (Fig. 7). Note that at 8/5 cm H2O the delivered volumes were inconsistent across each ventilation device due to the small pressure gradient.

Compliance curves of bubble noninvasive ventilation (NIV) versus Dräger Infinity V500 versus Hamilton G5 at 15/5 cm H2O.

Compliance curves of bubble noninvasive ventilation (NIV) versus Dräger Infinity V500 versus Hamilton G5 at 12/5 cm H2O.
Discussion
Modes of Noninvasive Ventilation
Widely used methods of noninvasive respiratory support for infants in respiratory distress include CPAP and NIV. CPAP consists of delivering a constant pressure, typically 5–8 cm H2O, to recruit and stabilize the alveoli and to improve ventilation and perfusion mismatch. NIV provides additional respiratory support with intermittent mandatory ventilation over the constant baseline pressure, eg, 15 cm H2O over 5 cm H2O. This additional respiratory support reduces the work of breathing.4 In comparison with CPAP, NIV has been shown to decrease the need for ventilation of preterm infants,6 decrease postextubation failure,7 and may further decrease the frequency of apneic episodes.8
Common interfaces for NIV modalities include nasal masks or occlusive prongs. NIV has become more prevalent in the past decade because it is associated with lower rates of bronchopulmonary dysplasia than invasive modes of ventilation.2 An additional benefit of noninvasive ventilation, particularly for settings with limited resources, is that it does not require all the staff and equipment necessary for invasive ventilation. To deliver safe invasive ventilation, requirements include regular arterial blood gas analysis; round-the-clock clinical coverage by intensive care specialists, including someone always present to address any alarms or tubing leaks; and continuous measurement of vital signs and oxygen saturation. Without these critical supporting elements, invasive ventilation can be dangerous and may cause more harm than good. A spontaneously breathing infant on noninvasive support also requires well-trained staff, but it may not require the same level of monitoring and support as an intubated patient.
Simple Methods of NIV
Barriers such as high cost, inconsistent electrical power, and complex equipment prevent many resource-limited settings from implementing ventilator-driven CPAP and NIV. In contrast, bubble CPAP is a simple mechanical system that is exclusively powered by blended compressed air and oxygen. Bubble CPAP utilizes the hydrostatic principle in which the partially submerged expiratory limb sets and displays the pressure in the circuit. This is intuitive to use and to troubleshoot: if there are no bubbles, the clinician knows to look for a leak. Bubble CPAP is safe and effective, and it is used worldwide.3 It is our hope that the development of a bubble NIV treatment can help deliver the benefits of NIV to many settings, including those with limited resources.
Results of the Present Experiments
In this study, comparable pressure waveform and tidal volume delivery was achieved with the bubble NIV, Hamilton, and Dräger ventilators across 3 different models of infant respiratory distress (ie, respiratory distress syndrome, pneumonia, and transient tachypnea of the newborn) at commonly used pressure settings. However, the bubble NIV system is nonelectric and is projected to cost much less than a typical ventilator.
Limitations
The simulated nasal prong interface in these studies had an occlusive fit, so the effects of a leak were not quantified. Further, these were passive studies, so the effects of an infant actively breathing were not assessed. Although the present iteration of the bubble NIV device does not have the ability to synchronize, there is some question as to a therapeutic benefit of synchronized NIV versus nonsynchronized NIV in infants.4 Additionally, the ability of synchronized NIV equipment to synchronize effectively is not well established due to the small inspiratory efforts of an infant.9 Finally, it is important to note that the Dräger and Hamilton ventilators used in these experiments can deliver many additional modes beyond NIV. In contrast, the bubble NIV system can only deliver bubble CPAP (without the float) and bubble NIV (with the float). Thus, the results of this study are only applicable for the noninvasive modes of CPAP and NIV.
Conclusions
The similarities of pressure waveforms and delivered tidal volumes in this simulated clinical scenario suggest that bubble NIV may provide efficacy comparable with that of traditional ventilator treatment for a range of patients. This may provide clinicians in resource-limited settings with an additional, simple, nonelectric treatment modality for the management of infant respiratory distress.
Footnotes
- Correspondence: Stephen C John BSE, University of Michigan Medical School, 1301 Catherine St, Ann Arbor, MI 41809. E-mail: scjres{at}gmail.com
Mr John presented a version of this paper at the 2019 Doctors Without Borders/Medecins Sans Frontieres Pediatric Days, held April 5–6, 2019, in Stockholm, Sweden.
This work was supported in part by the American Society of Mechanical Engineers. Dr Gustafson, Mr John, and Ms John have filed for international patent protection for a bubble NIV device; they have launched a startup company to develop this technology. The other authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}