

Abstract
BACKGROUND: This was a pilot study to analyze the effects of tracheostomy on patient-ventilator asynchronies and respiratory system mechanics. Data were extracted from an ongoing prospective, real-world database that stores continuous output from ventilators and bedside monitors. Twenty adult subjects were on mechanical ventilation and were tracheostomized during an ICU stay: 55% were admitted to the ICU for respiratory failure and 35% for neurologic conditions; the median duration of mechanical ventilation before tracheostomy was 12 d; and the median duration of mechanical ventilation was 16 d.
METHODS: We compared patient-ventilator asynchronies (the overall asynchrony index and the rates of specific asynchronies) and respiratory system mechanics (respiratory-system compliance and airway resistance) during the 24 h before tracheostomy versus the 24 h after tracheostomy. We analyzed possible differences in these variables among the subjects who underwent surgical versus percutaneous tracheostomy. To compare longitudinal changes in the variables, we used linear mixed-effects models for repeated measures along time in different observation periods. A total of 920 h of mechanical ventilation were analyzed.
RESULTS: Respiratory mechanics and asynchronies did not differ significantly between the 24-h periods before and after tracheostomy: compliance of the respiratory system median (IQR) (47.9 [41.3 – 54.6] mL/cm H2O vs 47.6 [40.9 – 54.3] mL/cm H2O; P = .94), airway resistance (9.3 [7.5 – 11.1] cm H2O/L/s vs 7.0 [5.2 – 8.8] cm H2O/L/s; P = .07), asynchrony index (2.0% [1.1 – 3.6%] vs 4.1% [2.3 – 7.6%]; P = .09), ineffective expiratory efforts (0.9% [0.4 – 1.8%] vs 2.2% [1.0 – 4.4%]; P = .08), double cycling (0.5% [0.3 – 1.0%] vs 0.9% [0.5 – 1.9%]; P = .24), and percentage of air trapping (7.6% [4.2 – 13.8%] vs 10.6% [5.9 – 19.2%]; P = .43). No differences in respiratory mechanics or patient-ventilator asynchronies were observed between percutaneous and surgical procedures.
CONCLUSIONS: Tracheostomy did not affect patient-ventilator asynchronies or respiratory mechanics within 24 h before and after the procedure
Introduction
Tracheostomy is performed in 10 to 15% of patients on mechanical ventilation in the ICU, and its prevalence has increased over the past 20 years.1,2 The main indications for tracheostomy are prolonged mechanical ventilation and difficult or prolonged weaning.3,4 The most common reasons for mechanical ventilation in patients who have been tracheostomized are acute respiratory failure, coma, COPD, neuromuscular disease, and trauma.5 Despite various studies about tracheostomy, the optimal timing and technique for the procedure in specific patient categories have yet to be established.5-12 Patient-ventilator asynchronies have been associated with muscle damage and increases in the duration of mechanical ventilation, ICU and hospital length of stay, and hospital mortality, as well as the need for tracheostomy.13-17
However, it is unknown whether tracheostomy influences patient-ventilator interactions and asynchronies.3 The potential benefits of tracheostomy on respiratory system mechanics are controversial. Some older studies found improvements in the work of breathing (WOB), pressure-time product (PTP), and auto-PEEP18,19; however, other studies did not confirm these findings.20 More recent studies measured respiratory mechanics in the operating room for a short period of time immediately after tracheostomy21 or WOB during spontaneous breathing under different scenarios but not in a before-and-after protocol.22 We aimed to assess and compare longitudinal changes in patient-ventilator asynchronies and respiratory system mechanics after tracheostomy in recordings of the 24-h periods before and after the procedure in subjects on mechanical ventilation connected to a system that allows the continuous monitoring of respiratory mechanics and the identification of various asynchronies.
Quick Look
Current Knowledge
The potential benefits of tracheostomy on respiratory system mechanics are controversial, and there are no current data that explored the role of the procedure on patient-ventilator interactions in a before-and-after protocol.
What This Paper Contributes to Our Knowledge
In this pilot study of subjects who were critically ill and on mechanical ventilation, tracheostomy did not affect patient-ventilator asynchronies or respiratory system mechanics 24 h after the procedure.
Methods
Design and Setting
We compared patient-ventilator asynchronies and respiratory system mechanics in the 24-h period before tracheostomy versus in the 24-h period after the procedure. Data were extracted from an ongoing, real-world database that was prospectively constructed in 2 ICUs equipped with the Better Care platform. The database contains observational data on adult patients who were intubated and expected to undergo invasive ventilation > 24 h with ventilators: Evita 4 (Dräger, Lübeck, Germany), Puritan Bennet 840 (Covidien, Dublin, Ireland), or Servo-i (Maquet, Solna, Sweden). The Better Care platform integrates signals from different ventilators and monitors, and applies algorithms to detect several typologies of patient-ventilator asynchronies.
The Comitè d’Ètica d’Investigació ambmedicaments at the Corporació Sanitària Parc Taulí and the clinical research ethics committee of Fundació Unió Catalana d’Hospitals approved the database and the study protocol. The need for informed consent was waived because the current study was noninterventional, posed no added risk to the subjects, did not interfere with usual care, and used anonymized data. The guidelines followed in this study were according to the applicable Spanish regulations (Biomedical Research Law 14/2007). This work was funded by projects PI09/91074, PI13/02204, and PI16/01606; integrated in the Plan Nacional de R+D+I; and co-funded by the ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER), RTC-2017-6193-1 (AEI/FEDER UE), CIBER Enfermedades Respiratorias, and Fundació Parc Taulí (Spain).
Participants
We studied 20 adult subjects who were tracheostomized during their ICU stay for prolonged intubation or for airway protection and who were expected to require mechanical ventilation > 24 h after tracheostomy. We excluded pregnant patients and those with do-not-resuscitate orders or with chest tubes with suspected bronchopleural fistulas. Demographics, clinical diagnosis, ventilator settings, endotracheal tube characteristics, type of tracheostomy, and outcome were retrieved from medical records. We also retrieved the dose of sedatives (mg/kg) administered hourly (expressed as midazolam dose-equivalents)23 and sedation levels with the Sedation-Agitation Scale.24
Measurements
The Better Care platform was used to capture the digital output from bedside monitors and ventilators, and to determine heart rate,  and respiratory variables.15,25 We analyzed breathing frequency, inspiratory time (TI), total PEEP, end-expiratory flow, peak expiratory flow, and the ratio of inspiratory time to duty cycle (TI/Ttot). To automatically and continuously assess respiratory-system compliance and airway resistance, impedance, and elastance through different ventilator modes, we used the least-squares fitting method breath by breath.26,27 Variables were averaged for each hour in the 24-h periods before and after tracheostomy. The Better Care platform analyzes respiratory signals breath by breath to identify asynchronous cycles by classifying them into 4 categories (ineffective expiratory effort, double triggering, short cycling, or prolonged cycling) and computes a global asynchrony index, expressed as a percentage, by dividing the number of asynchrony events by the total respiratory cycles (ie, ventilator cycles and wasted efforts) and multiplying by 100.13 The platform also estimates the percentage of air trapping. All these data are stored in a PostgreSQL database for further analyses. To avoid bias induced by airway manipulation and neuromuscular blocking during manipulation, we excluded from the analyses the time periods in which the airways were manipulated as well as the hour immediately before the procedure and the hour immediately after it.
and respiratory variables.15,25 We analyzed breathing frequency, inspiratory time (TI), total PEEP, end-expiratory flow, peak expiratory flow, and the ratio of inspiratory time to duty cycle (TI/Ttot). To automatically and continuously assess respiratory-system compliance and airway resistance, impedance, and elastance through different ventilator modes, we used the least-squares fitting method breath by breath.26,27 Variables were averaged for each hour in the 24-h periods before and after tracheostomy. The Better Care platform analyzes respiratory signals breath by breath to identify asynchronous cycles by classifying them into 4 categories (ineffective expiratory effort, double triggering, short cycling, or prolonged cycling) and computes a global asynchrony index, expressed as a percentage, by dividing the number of asynchrony events by the total respiratory cycles (ie, ventilator cycles and wasted efforts) and multiplying by 100.13 The platform also estimates the percentage of air trapping. All these data are stored in a PostgreSQL database for further analyses. To avoid bias induced by airway manipulation and neuromuscular blocking during manipulation, we excluded from the analyses the time periods in which the airways were manipulated as well as the hour immediately before the procedure and the hour immediately after it.
Statistical Analysis
Subjects’ characteristics are summarized as medians (25th–75th percentiles [interquartile range {IQR}) or percentages. Respiratory variables are summarized as means (95% CIs). The Kolmogorov-Smirnov test for normality was applied to assess for normality. To accurately describe the repeated measures over time by the period of observations (ie, hours), we used linear mixed-effects models.28 The fixed-effects part of the model allowed separate fits over time by period (ie, a period-by-hours interaction term) for the population mean. The random-effects part included an intercept for the subjects by the period to take into account inter- and intrasubject variability. To investigate the rate of patient-ventilator asynchronies, the model assumed a negative binomial distribution because the response variable (number of occurrences of asynchrony events) was limited to non-negative values and was positively skewed, with most observations having values near zero, and included an exposure term (the total number of respiratory cycles per hour), which indicates the number of times a particular event could have happened.
Negative binomial distributions have often been used in regression models with count data.29 We did not estimate the sample size needed to achieve a specific power. No general and well-established sample size methodology exists for mixed models in longitudinal studies with specific correlations among observations from the same individual. Simulation methods are recommended, but this approach is beyond the scope of our study. In this observational study, we analyzed all the data available from 20 subjects on mechanical ventilation. We used R 3.3.1 (R Core Team, Vienna, Austria) for all statistical analyses, building the mixed-effects models with the lme4 package and summarizing the mean (95% CI) hourly values by periods with the lsmeans package.30 Two-tailed significance was set at P < .05.
Results
The demographic and clinical characteristics of the 20 subjects with a tracheostomy included in the study (11 admitted for acute respiratory failure, 7 for neurologic conditions, and 2 for trauma) are reported in Table 1. The median (IQR) APACHE II score on ICU admission was 16 (13.8 – 20.3). The median (IQR) duration of mechanical ventilation before tracheostomy was 12 (9 – 15) d, and the median (IQR) total duration of mechanical ventilation was 16 (9 – 27) d. Tracheostomy was done percutaneously in 60% and surgically in 40% of the subjects. The mean (95% CI) endotracheal tube diameter was 7.7 (7.5 – 8.0) mm, and mean (95% CI) tracheostomy cannula diameter was 8.4 (8 – 9) mm (P < .05). The endotracheal tube diameters were 6.5, 7, 7.5, 8, and 8.5 mm in 1, 2, 5, 10, and 2 subjects, respectively. After the procedure, the tracheostomy cannula diameters were 8 mm and 9 mm in 10 subjects each. There were no significant differences in the use of ventilator modes before and after tracheostomy; the most common ventilator modes applied were volume assist-control ventilation (50% before vs 53% after tracheostomy), pressure-support ventilation (44% before vs 41% after tracheostomy), and airway pressure-release ventilation (6% before vs 6% after tracheostomy). The median (IQR) length of stay was 16 (18 – 35) d in the ICU and 47 (28 - 75) d in the hospital. Three subjects died during the hospital stay.
Subjects’ Clinical Characteristics, Type of Tracheostomy Performed, and Ventilatory Modes Used Before and After The Procedure
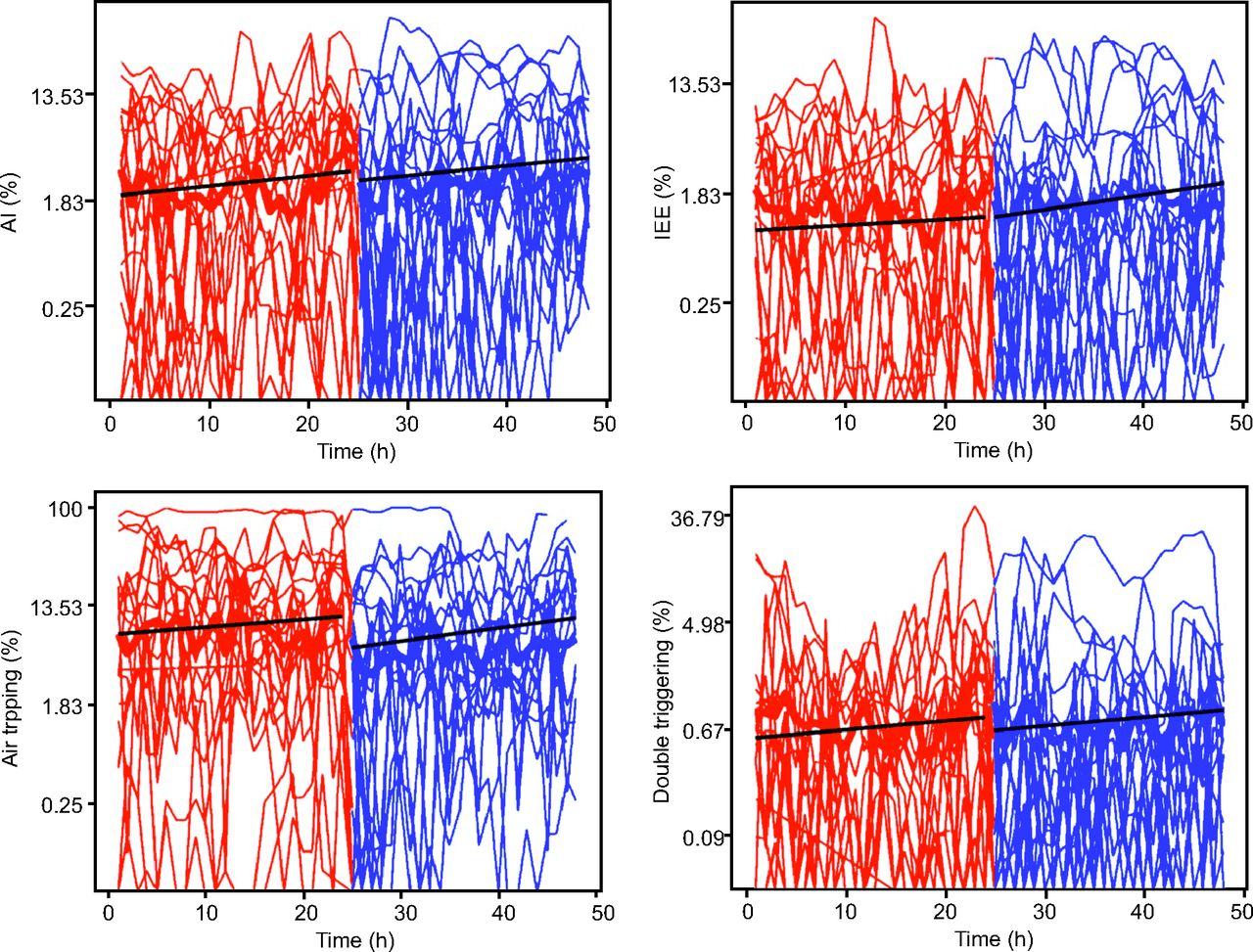
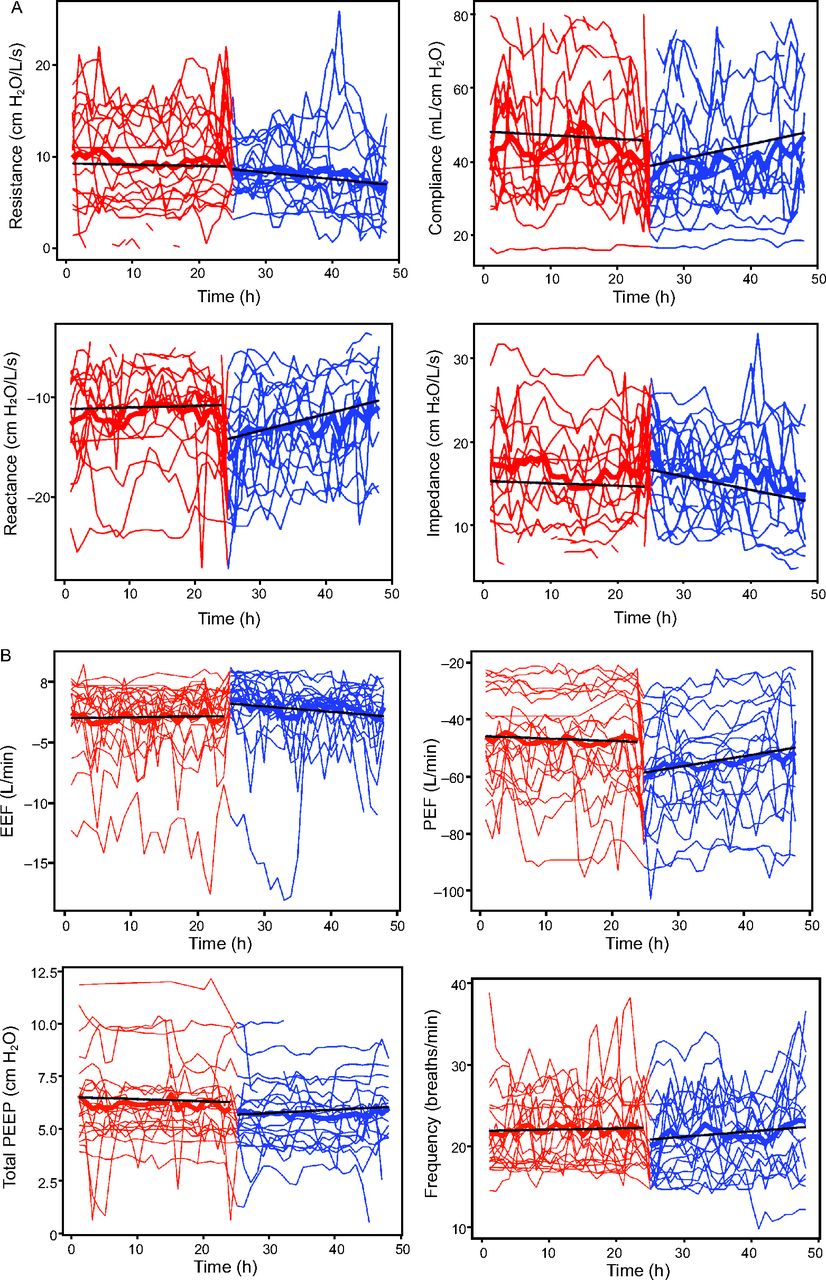
A total of 920 h of mechanical ventilation, 460 h before tracheostomy and 460 h after, were analyzed. The overall rate of asynchronies did not differ between the 24-h periods before and after tracheostomy (asynchrony index: 2.0% [1.1 - 3.6%] vs 4.1% [2.3 – 7.5%]; P = .09); likewise, the rates of specific asynchronies did not differ between the two periods (ineffective expiratory effort: 0.9% [0.5 – 1.8%] vs 2.2% [1.0 – 4.4%], P = .08; double cycling: 0.5% [0.3 - 1.0%] vs 0.9% [0.5 – 1.9%], P = .24; and air trapping: 7%4-13 vs 10%,5-19 P = .43). The evolution of these variables in the 24 h before and after the tracheostomy procedure is shown in Figure 1. The changes in respiratory variables, sedatives administered, and asynchronies between the 2 periods are summarized in Table 2. Overall, respiratory system mechanics, ventilator settings, use of sedatives, and sedation level (Sedation-Agitation Scale) did not change over time in the period studied (Fig. 2).

Longitudinal changes in patient-ventilator asynchronies before and after tracheostomy. Spaghetti plots, showing longitudinal changes of asynchronies over time before (red) and after tracheostomy (blue). Black lines show medians. Visualization of flow over time periods of the asynchrony index (AI), ineffective expiratory efforts (IEE), percentage of air trapping, and double cycling (DC).
Lung Mechanics and Asynchronies Before and After Tracheostomy

Longitudinal changes in respiratory mechanics before and after tracheostomy. Spaghetti plots, showing longitudinal changes of mechanical properties of the respiratory system over time before (red) and after tracheostomy (blue). Black lines show medians. A: Visualization of flow over time periods of dynamic resistance, compliance of the respiratory system, elastance, and impedance of the respiratory system. B: Visualization over time of end-expiratory flow (EEF), peak-expiratory flow (PEF), total PEEP, and breathing frequency.
We also analyzed whether there were differences in patient-ventilator asynchronies and in respiratory mechanics in the 24 h after tracheostomy between the subgroups of subjects who underwent surgical versus percutaneous procedures (see the supplementary materials at http://www.rcjournal.com). Tidal volume and Sedation-Agitation Scale scores after the procedure were lower in the surgical group, but they were also significantly lower before the tracheostomy; hence, these differences cannot be attributed to the technique. We also analyzed possible differences in these variables in relation to the reason for mechanical ventilation by comparing the subjects ventilated for acute respiratory failure (n = 11) versus those ventilated for neurologic conditions (n = 7) (see the supplementary materials at http://www.rcjournal.com). Overall, the subjects with acute respiratory failure already had significantly higher asynchrony index and rates of double cycling before tracheostomy, and these differences remained after the procedure. Moreover, after tracheostomy, ineffective expiratory effort, breathing frequency, and peak inspiratory flow increased in the subjects ventilated for acute respiratory failure but not in those ventilated for neurologic conditions.
Discussion
In the current pilot study, tracheostomy did not affect the rates of patient-ventilator asynchronies or the mechanical properties of the respiratory system in the 24 h after the procedure, regardless of the technique performed. Unlike previous studies, we used Better Care platform software validated to detect and quantify various patient-ventilator asynchronies and respiratory system mechanics in continuous recordings of ventilator waveforms from 24 h before tracheostomy to 24 h after the procedure, which enabled us to appreciate fluctuations in any parameter at any time during the period analyzed.16,25 To obtain dynamic and automated measurements of compliance of the respiratory system and airway resistance during volume assist-control and pressure-support ventilation, we used the least-squares fitting method,26,27 which weights the compliance and resistance of the respiratory system over the entire respiratory cycle and can be applied in patients who are receiving partial or full ventilatory support without any constraints with concern to the ventilatory pattern. Most studies about changes in the mechanical properties of the respiratory system after tracheostomy were done ∼20 years ago and included only surgical procedures, so our population likely better reflects contemporary ICU practice.18-21
The clinical indications for tracheostomy include attempts to increase patient comfort and to facilitate weaning.2 Patient-ventilator asynchronies are associated with increases in the duration of mechanical ventilation, in ICU and hospital length of stays, and in the rate of tracheostomies as well as with anxiety, discomfort, and negative outcomes, so various studies in the past decade aimed to optimize patient-ventilator interaction.16,17,31-33 We found that the rate of asynchronies did not change in the 24 h after tracheostomy. There were no differences in double cycling, ineffective expiratory effort, or asynchrony index; accordingly, the percentage of air trapping did not change. One possible explanation is that the low rates of asynchronies in the 24 h before tracheostomy (eg, the asynchrony index was only 2.0%) reduced the likelihood of finding effects. Moreover, because the respiratory system mechanics and Sedation-Agitation Scale did not change, it would seem logical that patient-ventilator asynchronies would remain unchanged under similar conditions.
Comparing subgroups of the subjects also provided interesting information. We found no differences in patient-ventilator asynchronies or respiratory system mechanics after the procedure between the subjects who underwent percutaneous versus surgical tracheostomy. Analysis of these results suggested that less-invasive methods led to similar outcomes and reinforced previous findings34 supported in current recent guidelines.35-37 With regard to the reason for mechanical ventilation, the rate of double cycling and the asynchrony index before tracheostomy was significantly higher in the subjects ventilated for acute respiratory failure than in those ventilated for neurologic conditions; after tracheostomy, in addition to maintaining this difference, those ventilated for respiratory failure also developed a higher rate of ineffective expiratory efforts, with associated higher breathing frequency and peak inspiratory flow 24 h after.
These results differed from previous findings that showed potential benefits of tracheostomy to reduce ineffective expiratory efforts and likely attributed to individual subject’s clinical conditions.18 In our study, the subjects in the acute respiratory failure subgroup were ventilated mainly for infections and/or inflammation and tracheostomy performed on day 12, whereas in the previous study, the subjects were ventilated mainly for diaphragmatic dysfunction, COPD, and coma, and were tracheostomized on day 31.18 This suggested that our subjects were still recovering from the initial insult at the time of tracheostomy and that some degree of dynamic hyperinflation developed during the 24 h after the procedure as a consequence of a higher breathing frequency resulted in a higher incidence of ineffective inspiratory efforts.38 Because tracheostomy did not change the respiratory mechanics in the subjects ventilated for acute respiratory failure who had asynchronies before tracheostomy, it is not surprising that the procedure did not decrease the rate of asynchronies and could even increase the rate of ineffective expiratory efforts.
With concern to the effects of tracheostomy on respiratory system mechanics, a previous study found that surgical tracheostomy decreased auto-PEEP, which led to reductions in the WOB and occlusion pressure, with a reduction in ineffective expiratory efforts.18 Similarly, another study found that airway resistance decreased and elastance increased immediately after surgical tracheostomy in the operating room, but they did not examine the evolution of respiratory mechanics thereafter.21 In contrast, one study found that tracheostomy decreased peak inspiratory pressure but did not affect WOB, airway resistance, or PTP in a cohort mainly composed of subjects with bronchiectasis or COPD.20 Similarly, other investigators reported no differences in tidal volume, breathing frequency, or auto-PEEP in the 12 h after tracheostomy; whereas they found that WOB decreased but only when expressed as J/min.19 The different results obtained in these studies are probably at least partly due to differences in the time points when the variables were measured.
We found that the mechanical properties of the respiratory system remained unchanged 24 h after the procedure, irrespective of the technique used, even though the diameter of the tracheostomy cannula was larger than that of the endotracheal tube. These findings differed from those of other studies, in which WOB and PTP changed after a tracheostomy, possibly because we found no differences in variables, such as auto-PEEP, tidal volume, compliance of the respiratory system, and airway resistance, which are directly related to WOB and PTP.18-21 It is also possible that these differences could be due to the time when the measurements were taken. Our study reported the results 24 h after the procedure, which provided a longer period of time for stabilization than previous studies in which the measurements were done at 6 h18 or 12 h.19 Moreover, unlike in other studies, our population comprised mainly subjects with acute respiratory failure of inflammatory or infectious origin and neurologic patients, which more accurately reflected the case mix in mixed ICUs nowadays. It should be emphasized that possible confounding effects of midazolam-dose equivalent and Sedation-Agitation Scale were negligible, given that they also remained invariable during the period studied.
Our study had some limitations. First, our cohort (20 subjects) was small, although continuous monitoring of various physiologic parameters over 48 h enabled us to analyze 920 h of patient-ventilator interactions. Second, the fact that the incidence of asynchronies was low before the tracheostomy and remained low after the procedure made it difficult to find significant differences. Third, we did not measure esophageal pressure, so we could not estimate WOB and the PTP; nevertheless, it is not unreasonable to assume that WOB and PTP should not vary when breathing frequency, tidal volume, and total PEEP remain constant, and when mechanical properties of the respiratory system are similar. Fourth, we did not evaluate the effects of tracheostomy in the subjects ventilated with proportional modes; thus, our findings should not be generalized to those modes. Fifth, tracheostomy could theoretically reduce the WOB and patient-ventilator asynchronies by reducing the inspiratory and expiratory resistive loads and improving expiratory flow3; nevertheless, although the increment of the inner diameter of the endotracheal tube increased (from 7.7 to 8.4 mm), this enlargement may be insufficient to observe a clinically relevant effect; hence, we could not exclude the hypothesis that a greater increase could favor patient-ventilator asynchronies.
Furthermore, our reported asynchrony index before the procedure was low (median [IQR] 2% [1.1 – 3.6%], which makes any significant change difficult to notice with the given studied population. Sixth, the accuracy of dynamic measurements obtained by using least-squares fitting can be limited in patients with severe flow limitation and in those who actively and vigorously use their respiratory muscles; however, this circumstance was not clinically observed and our population included only 2 subjects with COPD and these subjects did not have severe flow limitation. Moreover, we found no negative values of airway resistance that would suggest low pressure support level associated with spontaneous breathing activity,26 which further supported the use of least-squares fitting in our population.
Conclusions
In our pilot study of subjects who were critically ill and on mechanical ventilation, tracheostomy did not affect patient-ventilator asynchronies or respiratory system mechanics in the 24 h after the procedure. This hypothesis should be tested in a larger population study.
Data Availability
The datasets generated and analyzed in the current study are available from the corresponding author on reasonable request.
ACKNOWLEDGMENTS
The authors dedicate this work to the memory of Dr Kacmarek.
ASYNICU group: Candelaria de Haro, Josefina López-Aguilar, José Aquino Esperanza, Leonardo Sarlabous, Julia Estela, Sol Fernández-Gonzalo, Guillem Navarra-Ventura, Gemma Gomà, Ana Ochagavia, Lluís Blanch (Critical Care Center, Hospital Universitari Parc Taulí, Institut d’Investigació i Innovació Parc Taulí I3PT, Universitat Autònoma de Barcelona, Sabadell, Spain); Jaume Montanyà, Bernat Sales, Rudys Magrans (Better Care, Barcelona, Spain); Enrico Lena, Umberto Lucangelo (Department of Perioperative Medicine, Intensive Care and Emergency, Cattinara Hospital, Trieste University, Trieste, Italy); Rafael Fernández, Carles, Subirà (ICU, Fundació Althaia, Universitat Internacional de Catalunya, Manresa, Spain); Guillermo M. Albaiceta (Unidad de Cuidados Intensivos Cardiológicos, Hospital Universitario Central 1de Asturias, Oviedo, and Departamento de Biología Funcional, Instituto Universitario de Oncología del Principado de Asturias, Universidad de Oviedo. Oviedo, and CIBERES, Instituto de Salúd Carlos III, Madrid, Spain); Gastón Murias (Critical Care Department, Hospital Británico, Buenos Aires, Argentina); Robert M. Kacmarek (Department of Respiratory Care, Department of Anesthesiology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts).
Footnotes
- Correspondence: José Aquino-Esperanza MD, Critical Care Center, Parc Taulí Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí I3PT, Centro de Investigaciones Biomedicas en Red Enfermedades Respiratorias, Instituto de Salúd Carlos III, Facultat de Medicina, Universitat de Barcelona, Parc Taulí, 1, 08208 Sabadell, Spain. E-mail: jaquino{at}tauli.cat
See the Related Editorial on Page 1501
Drs Blanch, Montanyà, and Lucangelo are the inventors of a US patent owned by the Corporació Sanitària Parc Taulí: “Method and system for managing related patient parameters provided by a monitoring device,” US Patent No. 12/538,940. Drs Blanch, Montanyà, and Lucangelo own stock options in Better Care S.L., a research and development spinoff of Corporació Sanitària Parc Taulí (Spain). The remaining authors have no conflicts of interest to disclose.
Drs Lena and Aquino-Esperanza contributed equally to this work.
Additional investigators from the Asynchronies in the Intensive Care Unit (ASYNICU) Group are listed in the acknowledgments.
↵† Deceased.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}