
Abstract
Objective
To measure the effect of intense neuromuscular blockade (NMB) on oxygen consumption (VO2) in deeply sedated and mechanically ventilated children on the first day after complex congenital cardiac surgery.
Design
Prospective clinical interventional study.
Setting
Pediatric intensive care unit of an university medical centre.
Measurements and results
Nine mechanically ventilated and sedated children (weight 2.8–8.7 kg) were included. All children were treated with vasoactive drugs. The level of sedation was quantified using the comfort score, Ramsay score and bispectral index (BIS). The intensity of NMB was quantified using acceleromyography and VO2 was measured using indirect calorimetry. Analgo-sedation using various intravenous agents was targeted at a deep level (comfort score < 18, BIS < 60 and Ramsay score > 4). NMB was achieved by intravenous administration of rocuronium. All measurements were conducted before, during and after recovery from a period of intense NMB. Baseline values were VO2 6.1 ml/(kg min) (SD 1.3), comfort score 13 (SD 0.7), BIS 42.5 (SD 14.2), mean blood pressure 54.0 mmHg (SD 10.5), mean heart rate 129.9 bpm (SD 28.9) and mean core temperature 36.7°C (SD 0.5). There were no significant differences in VO2 or other parameters between baseline, during NMB and the recovery phase.
Conclusion
Neuromuscular blocking agents do not reduce oxygen consumption in deeply sedated and mechanically ventilated children after congenital cardiac surgery.
Similar content being viewed by others

Introduction
Following complex congenital cardiac surgery, a certain number of patients suffer from a low cardiac output syndrome leading to a distorted balance between oxygen delivery (DO2) and oxygen consumption (VO2) [1]. Besides sedation and mechanical ventilation, the use of neuromuscular blocking agents has been recommended in order to decrease VO2 [2].
To date, studies investigating the effect of neuromuscular blockade (NMB) on oxygen consumption show conflicting results, which may be explained by differences in study design [3–6].
We measured the effect of intense neuromuscular blockade on oxygen consumption in deeply sedated and mechanically ventilated children on the first day after complex congenital cardiac surgery.
Methods
This study was conducted in accordance with the Dutch national legislation concerning biomedical studies in children and was approved by the national and local ethics committees concerning medical research in humans. Oral and written informed consent was obtained from both parents.
We included children below 2 years of age on the first postoperative day following complex congenital cardiac surgery necessitating sedation and mechanical ventilation. Additional inclusion criteria were a body temperature between 36.0 and 38.0°C, FiO2 less than 0.6 and air leak less than 10%. Exclusion criteria were severe renal insufficiency, allergy to rocuronium, and the use of NMB on the same day prior to the study. Hemodynamic and respiratory monitoring was routinely performed using a HP Merlin monitoring system (HP, Irvine, USA). A rapidly changing blood pressure and/or heart rate were additional exclusion criteria.
All patients received analgo-sedation at the discretion of the treating physician (Table 1). Also, all children received inotropic agents consisting of a combination of dobutamine (mean dose 4.9 μg/kg/min) and/or nor-epinephrine (mean dose 0.4 μg/kg/min) combined with either enoximone of milrinone. Nutritional demands were met using either enteral feeding or intravenous dextrose as judged clinically necessary.
Oxygen consumption and carbon dioxide production were measured using the Deltatrac II metabolic monitor (GE healthcare, Chalfont St Giles, UK) as described previously [7]. This device provides a minute to minute VO2 value.
The bispectral index monitor (BIS, Aspect Medical Systems, USA) is based upon a one channel EEG recording at the frontal location. The device provides a value between 0 and 100. A level of 100 equals a fully awake state, while a level between 40 and 60 reflect deep sedation or anesthesia. In children the BIS value correlates well with the level of sedation [8]. For clinical evaluation of the level of sedation the comfort score (CS) was used which has been described elsewhere [9, 10]. A score below 17 points reflects deep sedation. Although not validated in children we also determined the Ramsay Score (RS) [11]. The sedation scores were always determined by one author (JL) at the beginning, half-way and at the end of a recording period.
The intensity of NMB was guided by acceleromyographic recording of the thumb adduction following train-of-four stimulation (TOF) of the ulnar nerve with a 1-min interval (TOF-watch, Organon, Boxtel, the Netherlands). This device has been validated in small children [12, 13]. A TOF count (TCNT) of zero was considered intense NMB. A TOF ratio > 0.8 and the first response in the train-of-four (T1) > 80% indicated sufficient clinical recovery from NMB.
We also collected PIM and PRISMII scores reflecting severity of illness [14, 15]. Furthermore, we collected data concerning length of stay (LOS), diagnosis, weight, height, and age. Mean blood pressure, heart rate, and core temperature were continuously measured.
At the start of the experiment, care was taken to provide a deep level of sedation with a CS less than or equal to 17, a RS higher than 4 and a BIS value less than 60. When this level of sedation was reached (but before NMB was instituted) a baseline registration was performed. Hereafter intense NMB was achieved by administering rocuronium in a dose of 0.3 mg/kg. If the TCNT did not decrease to 0 additional doses of rocuronium 0.15 mg/kg were given until the required TCNT was reached. At that point the registration of the NMB phase was started. During this phase, additional rocuronium (0.15 mg/kg) was administered if the TCNT value increased >0. After recording of the NMB phase time was taken to let the muscle relaxant ware off. When the TOF value exceeded 0.8 and T1 > 80% recording of the recovery phase was performed.
A registration period in which all variables were collected lasted 20 min. The mean value of these 20 min was taken for further calculation.
The coefficient of variation of the VO2 measurement was calculated by dividing the standard deviation of measurements with 1-min interval by the mean value of the 20-min episode. Sample size calculation was performed using an expected variation of VO2 measurement of 7%, a clinically significant change in VO2 of at least 5%, a power of 80% and P value of 0.05. This resulted in a sample size of 13. Potential differences between various parameters during baseline, NMB and recovery were analyzed using ANOVA. Statistical calculations were performed using MedCalc version 9 (MedCalc Software, Mariakerke, Belgium).
Results
The coefficient of variation of the VO2 measurements was 3.7% at baseline, 3.3% during NMB and 3.5% after recovery from NMB (mean 3.5%). Because the coefficient of variation was lower than anticipated (3.6 vs. 7%), we stopped the study after the inclusion of nine patients while maintaining the previously mentioned power.
Patient details are depicted in Table 1. The mean dose of rocuronium needed to achieve intense NMB was 0.7 mg/kg (range 0.3–1.2 mg/kg).
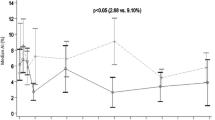
Figure 1 shows the individual changes in VO2 for the nine patients during the experiment. Table 2 shows the mean values for several parameters before, during, and after neuromuscular blockade. Using ANOVA no changes in VO2 or any of the other parameters were detected between baseline, during neuromuscular blockade, and the recovery phase except for intensity of NMB.

Individual course of oxygen consumption during the baseline, NMB and recovery phase (n = 9)
Discussion
This study shows that neuromuscular blocking agents do not reduce metabolic needs in deeply sedated and mechanically ventilated children after cardiac surgery.
In critically ill children one other study also observed a lack of difference between children with or without NMB [16]. However, most studies found a reduction in VO2 after application of NMB [3–6, 17], although in some studies the effect was smaller or absent in patients without spontaneous movements before NMB was instituted [6]. One study in deeply sedated adults found similar results compared to our study [18]. We believe the level of sedation explains these differences. All children in our study were on controlled mechanical ventilation and had a documented deep level of sedation. Since NMB only affects skeletal muscle activity it seems logical to assume that, when muscle activity is already very low, a further reduction in VO2 is not to be expected.
We made several precautions to optimize the validity of the recorded data. All measurements were recorded automatically; sedation scores were recorded by the same person and were supplemented by a measured BIS value. Also we observed a small variation in the VO2 measurement. Furthermore the intensity of the neuromuscular blockade was recorded using an established technique validated in (young) children. Using this technique we could actually demonstrate an intense level of NMB during the study and on the other hand a sufficient level of recovery at the end of the study.
The study is limited by several factors. With oxygen fractions in excess of 0.4 the accuracy of VO2 measurement may decrease [7]. Although three children in our study were ventilated with a FiO2 in excess of 0.4 (Table 1) the goal of this study was to detect changes in VO2 within a relatively small time interval and because each patient acted as his or her own control we consider this to be of minor influence. The reliability of BIS and sedation scores might be questionable. It is therefore possible that several children reached a sedation level which was equivalent to an anesthesia level. Caution is advised to extrapolate these results to other critically ill children, for example, with sepsis, trauma, or respiratory failure. Furthermore in our study only one child had a SaO2 below 90% and our results may therefore not apply to children with a severe cyanosis. Lastly we only measured the effect of NMB on the first postoperative day. Results could differ when NMB is instituted in a later clinical phase.
While the level of sedation seems to be very important in the reduction of VO2, the use of high dose sedatives seems attractive with the need for a reduction in VO2. However these agents are associated with many side effects or complications [19] and might even reduce cardiac output. On the other hand, prolonged NMB is also associated with various possible side effects. The most feared complication is the critical illness neuromuscular disease [20].
Conclusion
Neuromuscular blocking agents do not reduce oxygen consumption and therefore do not reduce energy expenditure in well-sedated children following complex congenital cardiac surgery.
Abbreviations
- VO2:
-
Oxygen consumption (ml/kg/min)
- NMB:
-
Neuromuscular blockade
- PEEP:
-
Positive end expiratory pressure (cmH2O)
- TOF:
-
Train-of-four (ratio)
- T1:
-
First response in the train-of-four (%)
- TCNT:
-
TOF count
- FiO2 :
-
Inspiratory oxygen fraction
- PA:
-
Pulmonary atresia
- PDA:
-
Patent ductusarteriosus
- TPGV:
-
Transposition great vessels
- Fallot:
-
Tetralogy of Fallot
- AVSD:
-
Atrioventricularseptal defect
- VSD:
-
Ventricular septal defect
- MAPCA:
-
Major aorto-pulmonary collateral arteries
- LOS:
-
Length of stay
- BIS:
-
Bispectral index
- SaO2 :
-
Arterial oxygen saturation (%)
- MAP:
-
Mean arterial pressure (mmHg)
References
Parr GV, Blackstone EH, Kirklin JW (1975) Cardiac performance and mortality early after intracardiac surgery in infants and young children. Circulation 51:867–874
Martin LD, Bratton SL, O’Rourke PP (1999) Clinical uses and controversies of neuromuscular blocking agents in infants and children. Crit Care Med 27:1358–1368
Vernon DD, Witte MK (2000) Effect of neuromuscular blockade on oxygen consumption and energy expenditure in sedated, mechanically ventilated children. Crit Care Med 28:1569–1571
Barton RG, Craft WB, Mone MC, Saffle JR (1997) Chemical paralysis reduces energy expenditure in patients with burns and severe respiratory failure treated with mechanical ventilation. J Burn Care Rehabil 18:461–468
Marik PE, Kaufman D (1996) The effects of neuromuscular paralysis on systemic and splanchnic oxygen utilization in mechanically ventilated patients. Chest 109:1038–1042
Palmisano BW, Fisher DM, Willis M, Gregory GA, Ebert PA (1984) The effect of paralysis on oxygen consumption in normoxic children after cardiac surgery. Anesthesiology 61:518–522
Joosten KF, Jacobs FI, van Klaarwater E, Baartmans MG, Hop WC, Meriläinen PT, Hazelzet JA (2000) Accuracy of an indirect calorimeter for mechanically ventilated infants and children: the influence of low rates of gas exchange and varying FIO2. Crit Care Med 28:3014–3018
Lamas A, Lopez-Herce J, Sancho L, Mencía S, Carrillo A, Santiago MJ, Martínez V (2008) Assessing sedation in critically ill children by bispectral index, auditory-evoked potentials and clinical scales. Intensive Care Med. doi:10.1007/s00134-008-1198-1
Triltsch AE, Nestmann G, Orawa H, Moshirzadeh M, Sander M, Grosse J, Genähr A, Konertz W, Spies CD (2005) Bispectral index versus COMFORT score to determine the level of sedation in paediatric intensive care unit patients: a prospective study. Crit Care 9:R9–R17
Marx CM, Smith PG, Lowrie LH, Hamlett KW, Ambuel B, Yamashita TS, Blumer JL (1994) Optimal sedation of mechanically ventilated pediatric critical care patients. Crit Care Med 22:163–170
Ramsay MA, Savege TM, Simpson BR, Goodwin R (1974) Controlled sedation with alphaxalone–alphadolone. Br Med J 2:656–659
Driessen JJ, Robertson EN, Booij LH (2005) Acceleromyography in neonates and small infants: baseline calibration and recovery of the responses after neuromuscular blockade with rocuronium. Eur J Anaesthesiol 22:11–15
Driessen JJ, Robertson EN, Van Egmond J, Booij LH (2002) Time-course of action of rocuronium 0.3 mg kg−1 in children with and without end stage renal failure. Paediatr Anaesth 12:507–510
Shann F, Pearson G, Slater A, Wilkinson K (1997) Paediatric index of mortality (PIM): a mortality prediction model for children in intensive care. Intensive Care Med 23:201–207
Pollack MM, Ruttimann UE, Getson PR (1988) Pediatric risk of mortality (PRISM) score. Crit Care Med 16:1110–1116
Briassoulis G, Venkataraman S, Thompson AE (2000) Energy expenditure in critically ill children. Crit Care Med 28:1166–1172
Manthous CA, Hall JB, Kushner R, Schmidt GA, Russo G, Wood LD (1995) The effect of mechanical ventilation on oxygen consumption in critically ill patients. Am J Respir Crit Care Med 151:210–214
Freebairn RC, Derrick J, Gomersall CD, Young RJ, Joynt GM (1997) Oxygen delivery, oxygen consumption, and gastric intramucosal pH are not improved by a computer-controlled, closed-loop, vecuronium infusion in severe sepsis and septic shock. Crit Care Med 25:72–77
Terao Y, Miura K, Saito M, Sekino M, Fukusaki M, Sumikawa K (2003) Quantitative analysis of the relationship between sedation and resting energy expenditure in postoperative patients. Crit Care Med 31:830–833
Tabarki B, Coffinieres A, Van Den BP, Huault G, Landrieu P, Sebire G (2002) Critical illness neuromuscular disease: clinical, electrophysiological, and prognostic aspects. Arch Dis Child 86:103–107
Conflict of interest statement
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Lemson, J., Driessen, J.J. & van der Hoeven, J.G. The effect of neuromuscular blockade on oxygen consumption in sedated and mechanically ventilated pediatric patients after cardiac surgery. Intensive Care Med 34, 2268–2272 (2008). https://doi.org/10.1007/s00134-008-1252-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1252-z