
Abstract
Purpose
The authors reviewed chest radiographs (CXR) and thin-section computed tomography (CT) findings of pulmonary complications in a selected population of 50 consecutive patients with severe novel swine-origin influenza A (H1N1) virus (S-OIV) pneumonia who were seen at the Subintensive Respiratory Unit (UTSIR) and at the Intensive Care Unit (ICU) at Monaldi Hospital, Naples, Italy.
Materials and methods
CXR and CT findings of 50 patients who fulfilled the World Health Organisation (WHO) criteria for S-OIV infection were reviewed by four radiologists. The final study group of 50 patients was divided into two subgroups on the basis of clinical course: group 1 consisted of 42 patients requiring noninvasive mechanical ventilation and admitted to the UTSIR; group 2 consisted of eight patients who required ICU admission and extracorporeal membrane oxygenation or advanced mechanical ventilation from October 2009 to December 2009. All patients underwent CXR and thinsection multidetector CT (MDCT) scan; the initial and follow-up radiographs and CT scans were evaluated for the presentation and follow-up pattern (consolidation, groundglass opacities, nodules, reticulation), distribution and extent of abnormality.
Results
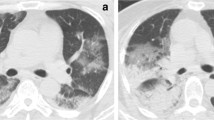
All patients had radiological signs of pulmonary involvement. Ground-glass opacity and consolidation, which was mainly peripheral, was the most frequent finding. In three patients, we report for the first time in viral pneumonia the reversed halo sign. Lesion extent was related to aggressiveness of the illness. More often, both lungs were involved (82%). Thoracic comorbidity was present in 18% of patients; 22% of patients was obese, and in this group, the clinical course was more aggressive than in the others with the same lesion extent at imaging. Furthermore, superinfection led to worsening of the clinical conditions.
Conclusions
The most common CXR and CT findings in patients with S-OIV infection were unilateral or bilateral ground-glass opacities with or without associated focal or multifocal areas of consolidation. On MDCT, ground-glass opacities and areas of consolidation had a predominant peribronchovascular and subpleural distribution, resembling organising pneumonia; they progressed to bilateral extensive airspace disease in severely ill patients.
Riassunto
Obiettivo
Lo scopo di questo lavoro è stato quello di definire il quadro radiologico (RX) e la semeiotica della tomografia computerizzata (TC) a strato sottile delle complicanze polmonari in una popolazione selezionata di 50 pazienti consecutivi affetti da influenza virale A (H1N1) di origine suina (S-OIV) ricoverati nell’unità di terapia respiratoria subintensiva (UTSIR) e nella terapia intensiva (ICU) dell’Azienda Ospedaliera Monaldi, Napoli, Italia.
Materiali e metodi
Quattro radiologi hanno retrospettivamente esaminato gli esami radiologici tradizionali (RX) e di tomografia computerizzata multidetettore (TCMD) di cinquanta pazienti che rispettavano i criteri della World Health Organization (WHO) per l’influenza A (H1N1) S-OIV. Il gruppo dei 50 pazienti in studio è stato suddiviso in due sottogruppi sulla base del decorso clinico: il gruppo 1, composto da 42 pazienti che hanno richiesto la ventilazione meccanica non invasiva e ricoverati all’UTSIR; il gruppo 2, costituito da 8 pazienti sottoposti a extra corporeal membrane oxygenation (ECMO) o a ventilazione meccanica convenzionale protetta, ricoverati in ICU da ottobre a dicembre 2009. Tutti i pazienti hanno eseguito esami RX e TCMD a strato sottile, di cui è stato valutato il pattern di ingresso e di follow-up (consolidazione, opacità groundglass, noduli e reticolazione interstiziale), la distribuzione e l’estensione delle alterazioni.
Risultati
Tutti i pazienti hanno mostrato segni di interessamento polmonare. L’opacità ground-glass (GGO) e la consolidazione, principalmente periferiche, sono stati i segni più frequenti. Segnaliamo per la prima volta in una polmonite virale in tre pazienti il segno dell’alone invertito (reversed halo sign). L’estensione delle lesioni è risultata correlata all’aggressività clinica della malattia. Nella nostra casistica sono stati spesso (82%) interessati entrambi i polmoni. Il 18% dei pazienti presentava una comorbidità toracica; il 22% di essi era obeso ed in questo gruppo, pur con la stessa estensione delle lesioni all’imaging rispetto ai non obesi, il decorso clinico è stato più aggressivo. Infine la sovra-infezione ha determinato un peggioramento delle condizioni cliniche.
Conclusioni
I segni RX e TCMD più comuni nei pazienti con influenza virale A di origine suina sono rappresentati da opacità GGO uni- o bilaterali con o senza aree di consolidazione focali o multifocali associate. Alla TC le aree GGO e consolidative hanno presentato una distribuzione prevalente subpleurica e peribroncovasale, rassomigliando alla polmonite in organizzazione; in pazienti gravemente malati esse progrediscono ad una malattia consolidativa degli spazi aerei bilaterale ed estesa.
Article PDF
Similar content being viewed by others


References/Bibliografia
Taubenberger JK, Morens DM (2008) The pathology of influenza virus infections. Annu Rev Pathol 3:499–522
Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S et al (2009) Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med 361:680–689
Chan M (2009) World now at start of 2009 influenza pandemic. http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html. Last access August 2011
Fiore AE, Shay DK, Broder K et al (2008) Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 57:1–60
Kim EA, Lee KS, Primack SL et al (2002) Viral pneumonias in adults: radiologic and pathologic findings. Radiographics 22:S137–S149
Lee CW, Seo JB, Song JW et al (2009) Pulmonary complication of novel influenza A (H1N1) infection: imaging features in two patients. Korean J Radiol 10:531–534
Ajlan AM, Quiney B, Nicolaou S, Müller NL (2009) Swine-origin influenza A (H1N1) viral infection: radiographic and CT findings. AJR Am J Roentgenol 193:1494–1499
Agarwal PP, Cinti S, Kazerooni EA (2009) Chest radiographic and CT findings in novel swine-origin influenza A (H1N1) virus (S-OIV) infection. AJR Am J Roentgenol 193:1488–1493
Mollura DJ, Asnis DS, Crupi RS et al (2009) Imaging findings in a fatal case of pandemic swine-origin influenza A (H1N1). AJR Am J Roentgenol 193:1500–1503
Lee EY, McAdam AJ, Chaudry G et al (2010) Swine-origin influenza A (H1N1) viral infection in children: initial chest radiographic findings. Radiology 254:934–941
Guo HH, Sweeney RT, Regula D, Leung AN (2010) Best cases from the AFIP: fatal 2009 influenza A (H1N1) infection, complicated by acute respiratory distress syndrome and pulmonary interstitial emphysema. Radiographics 30:327–333
Hansell DM, Bankier AA, MacMahon H et al (2008) Fleischner Society: glossary of terms for thoracic imaging. Radiology 246:697–722
Zerhouni EA, Naidich DP, Stitik FP et al (1985) Computed tomography of the pulmonary parenchyma. II. Interstitial disease. J Thorac Imaging 1:54–64
Westcott JL, Cole SR (1986) Traction bronchiectasis in end-stage pulmonary fibrosis. Radiology 161:665–669
Webb WR, Muller NL, Naidich DP (2001) High-resolution CT of the lung. Lippincott Williams & Wilkins, New York
Antonio GE, Wong KT, Hui DS et al (2003) Thin-section CT in patients with severe acute respiratory syndrome following hospital discharge: preliminary experience. Radiology 28:810–815
Bernard GR, Artigas A, Brigham KL et al (1994) The American-European Consensus Conference on ARDS: definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149:818–824
Gattinoni L, Caironi P, Pelosi P, Goodman LR (2001) What has computed tomography taught us about the acute respiratory distress syndrome? Am J Respir Crit Care Med 164:1701–1711
Desai SR, Wells AU, Rubens MB et al (1999) Acute respiratory distress syndrome: CT abnormalities at longterm follow-up. Radiology 210:29–35
Dawood FS, Jain S, Finelli L et al (2009) Emergence of a novel swineorigin influenza a (H1N1) virus in humans. N Engl J Med 360:2605–2615
Hancock K, Veguilla V, Lu X et al (2009) Cross-reactive antibody responses to the 2009 pandemic H1N1 influenza virus. N Engl J Med 361:1945–1952
Tillett HE, Smith JW, Clifford RE (1980) Excess morbidity and mortality associated with influenza in England and Wales. Lancet 1:793–795
Busi Rizzi E, Schininà V, Ferraro F et al (2010) Radiological findings of pneumonia in patients with swineorigin influenza A virus (H1N1). Radiol Med 115:507–515
Cheah FK, Sheppard MN, Hansell DM (1993) Computed tomography of diffuse pulmonary hemorrhage with pathological correlation. Clin Radiol 48:89–93
Gill JR, Sheng ZM, Ely SF et al (2010) Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch Pathol Lab Med 134:235–243
Wysocki M, Antonelli M (2001) Noninvasive mechanical ventilation in acute hypoxaemic respiratory failure. Eur. Respir J 18:209–220
Shieh WJ, Blau DM, Denison AM et al (2010) 2009 pandemic influenza A (H1N1): pathology and pathogenesis of 100 fatal cases in the United States. Am J Pathol 177(1):166–175
Abella HA (2009) X-rays and CT offer predictive power for swine flu diagnosis. www.diagnosticimaging.com/news/display/article/113619/1425699#
Ketai LH (2009) Conventional wisdom: unconventional virus. AJR Am J Roentgenol 193:1486–1487
Wong KT, Antonio GE, Hui DSC et al (2003) Thin-section CT of severe acute respiratory syndrome: evaluation of 73 patients exposed to or with the disease. Radiology 228:395–400
Zompatori M, Poletti V, Battista G et al (1999) Bronchiolitis obliterans with organizing pneumonia (BOOP), presenting as a ring-shaped opacity at HRCT (the atoll sign): a case report. Radiol Med 97:308–310
Voloudaki AE, Bouros DE, Froudarakis ME et al (1996) Crescentic and ring-shaped opacities: CT features in two cases of bronchiolitis organizing pneumonia (BOOP). Acta Radiol 37:889–892
Kim SJ, Lee KS, Ryu YH et al (2003) Reversed halo sign on high-resolution CT of cryptogenic organizing pneumonia: diagnostic implications. AJR Am J Roentgenol 180:1251–1254
Hsu A, Stark P, Friedman PJ (2007) Focal organizing pneumonia with reversed halo sign. Applied Radiology 36. http://www.appliedradiology.com/Issues/2007/08/Cases/Focal-organizingpneumonia-with-reversed-halo-sign.aspx. Last access August 2011
Maimon N (2010) A 47-year-old female with shortness of breath and “reversed halo sign”. Eur Respir Rev 19:83–85
Gasparetto EL, Escuissato DL, Davaus T et al (2005) Reversed halo sign in pulmonary paracoccidioidomycosis. AJR Am J Roentgenol 184:1932–1934
Geronemus A, Coppage L, Hazelton T (2004) The reversed halo sign: a nonspecific finding on CT of the thorax. RSNA 2441EP-CH-e
Choi YH, Im J-G, Park CK (2002) Notes from the 2001 Annual Meeting of the Korean Society of Thoracic Radiology. J Thorac Imaging 17:170–175
Agarwal R, Aggarwal AN, Gupta D (2007) Another cause of reverse halo sign: Wegener’s granulomatosis. Br J Radiol 80:849–850
Benamore RE, Weisbrod GL, Hwang DM et al (2007) Reversed halo sign in lymphomatoid granulomatosis. Br J Radiol 80:e162–e166
Kumazoe H, Matsunaga K, Nagata N et al (2009) “Reversed Halo Sign” of high-resolution computed tomography in pulmonary sarcoidosis. J Thorac Imaging 24:66–68
Marchiori E, Zanetti G, Mano CM et al (2010) The reversed halo sign: another atypical manifestation of sarcoidosis. Korean J Radiol 11:251–252
Ahuja A, Gothi D, Joshi JM (2007) A 15-year-old boy with “reversed halo”. Indian J Chest Dis Allied Sci 49:99–101
Marchiori E, Grando RD, Simoes Dos Santos CE et al (2010) Pulmonary tuberculosis associated with the reversed halo sign on high resolution CT. Br J Radiol 83:e58–e60
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Valente, T., Lassandro, F., Marino, M. et al. H1N1 pneumonia: our experience in 50 patients with a severe clinical course of novel swine-origin influenza A (H1N1) virus (S-OIV). Radiol med 117, 165–184 (2012). https://doi.org/10.1007/s11547-011-0734-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-011-0734-1