
Abstract
Purpose
Direct laryngoscopic tracheal intubation is a potentially lifesaving procedure, but a difficult skill to acquire and maintain. The consequences of poorly performed intubation attempts are potentially severe. The Pentax AWS® and the Glidescope® are indirect laryngoscopes that may require less skill to use. We therefore hypothesized that AWS® and Glidescope® would prove superior to the Macintosh laryngoscope when used by novices in the normal and simulated difficult airway.
Methods
In this prospective randomized crossover trial following standardized didactic instruction, medical students with no prior experience of laryngoscopy performed tracheal intubation using each device. Each student was allowed up to three attempts to intubate in a Laerdal® Intubation Trainer in two laryngoscopy scenarios and in a Laerdal® SimMan® manikin in one scenario. The students then performed tracheal intubation of the normal airway a second time to characterize the learning curve for each device.
Results
The Pentax AWS® provided better intubation conditions than the Glidescope® or the Macintosh, resulting in greater success of intubation, particularly in the difficult laryngoscopy scenarios. The Glidescope® demonstrated advantages over the Macintosh, particularly in the more difficult scenarios. Both the AWS® and the Glidescope® decreased the duration of intubation attempts, reduced the number of maneuvers required, and reduced the potential for dental trauma. In direct comparisons, the AWS® provided the best intubation conditions.
Conclusions
The Pentax AWS® appears to constitute a better alternative to the Macintosh for novice personnel to acquire the skills of tracheal intubation.
Résumé
Objectif
L’intubation trachéale par laryngoscopie directe est une procédure potentiellement salutaire, mais il s’agit également d’une compétence difficile à acquérir et à maintenir. Les conséquences de tentatives d’intubation mal réalisées sont potentiellement graves. Le Pentax AWS® et le Glidescope® sont des laryngoscopes indirects qui pourraient nécessiter une compétence moindre. Ainsi, nous avons émis l’hypothèse que l’AWS® et le Glidescope® donneraient de meilleurs résultats que le laryngoscope Macintosh lors de leur utilisation par du personnel inexpérimenté pour l’intubation de voies aériennes normales ou rendues difficiles par simulation.
Méthode
Dans cette étude croisée randomisée et prospective qui a été menée à la suite d’une formation didactique standard, des étudiants en médecine n’ayant pas d’expérience antérieure en matière de laryngoscopie ont réalisé une intubation trachéale à l’aide de chacun des appareils. Chaque étudiant avait droit à un maximum de trois tentatives d’intubation sur un simulateur d’intubation Laerdal® dans le cadre de deux scénarios de laryngoscopie, dont l’un sur un mannequin Laerdal® SimMan®. Les étudiants ont ensuite réalisé une seconde intubation trachéale dans une voie aérienne normale afin de déterminer la courbe d’apprentissage de chaque appareil.
Résultats
Le Pentax AWS® a procuré de meilleures conditions d’intubation que le Glidescope® ou le Macintosh, ce qui a eu pour résultat un taux de réussite de l’intubation plus élevé et ce, particulièrement dans les situations de laryngoscopie difficile. Le Glidescope® a démontré des avantages par rapport au Macintosh, notamment dans les situations de laryngoscopie plus difficile. L’AWS® et le Glidescope® ont permis de réduire la durée des tentatives d’intubation, le nombre de manœuvres nécessaires, ainsi que le potentiel d’un traumatisme dentaire. En comparaison directe, l’AWS® était le laryngoscope procurant les meilleures conditions d’intubation.
Conclusion
Le laryngoscope Pentax AWS® semble constituer une meilleure alternative au Macintosh pour permettre au personnel inexpérimenté d’acquérir les compétences nécessaires à l’intubation trachéale.
Similar content being viewed by others

Direct laryngoscopic tracheal intubation is a potentially lifesaving procedure in diverse clinical situations characterized by respiratory failure and/or loss of patient control of the airway. Several studies have demonstrated improved outcome in critically ill and injured patients if the airway is secured early by endotracheal intubation.1–3 Accordingly, this skill is taught to many healthcare professionals, both medical and paramedical, many of whom may be infrequently required to perform this maneuver. However, conventional direct laryngoscopy is a difficult skill to acquire,4–6 and proficiency deteriorates over time if not practiced.7 This issue is compounded by the fact that the consequences of poorly performed intubation attempts are potentially severe. Difficult or failed tracheal intubation in this context constitutes an important cause of morbidity arising from direct airway trauma and the systemic complications of hypoxia.8,9
The Airway Scope® (AWS®; Pentax Corporation, Tokyo, Japan) is a novel system for tracheal intubation that provides a view of the glottis without requiring alignment of oral, pharyngeal, and laryngeal axes (Fig. 1a).10 The curve-shaped blade has a side channel that acts as the housing for placement and insertion of the endotracheal tube (ETT). Once the target signal shown on the monitor has been aligned with the glottic opening, the ETT is advanced through the vocal cords and held in place, and the device is removed. The target signal on the monitor may be of particular benefit to novice laryngoscopists. The Glidescope® Cobalt (Verathon®, Bothell, WA, USA) is a similar indirect laryngoscope without incorporating a side-channel that also demonstrates considerable promise (Fig. 1b). 11,12

a Photograph of the Glidescope® laryngoscope. The device is held in the left hand and passed into the mouth over the tongue, and the tip is placed in the vallecula or under the epiglottis. b Photograph of the Pentax AWS® laryngoscope. The device is held in the left hand and passed into the mouth over the tongue, and the tip is placed in the vallecula or under the epiglottis
The AWS® and Glidescope® devices may require less operator skill to use. In direct comparison studies, advantages over the Macintosh have been demonstrated for both the Glidescope® 13 and the AWS®.10 The Pentax AWS® has shown to reduce the time to secure the airway and to decrease the incidence of failed tracheal intubation in novice laryngoscopists.14 In contrast, the efficacy of the Glidescope® in novice laryngoscopists is not clear. We hypothesized that the AWS® and the Glidescope® would prove superior to the Macintosh laryngoscope in the hands of novice laryngoscopists. Based on our earlier studies in manikins15 and in patients undergoing cervical immobilization,15,16 we also hypothesized that the AWS® would prove superior to the Glidescope® in this setting.
Methods
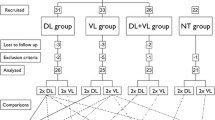
Following ethical committee approval and written informed consent, 53 medical students with no prior experience performing tracheal intubations consented to participate in this randomized crossover study. Each participant was given a standardized 5-min training period on each of the devices, i.e., the Macintosh, the Glidescope® and the AWS®, by one of the investigators. This training included a demonstration of the intubation technique for each device and oral instructions regarding the correct use of each device. For intubation attempts with the Glidescope® laryngoscope, a malleable stylet was inserted onto the ETT, and the ETT was bent into the “hockey-stick” curvature. The ETTs used during intubation attempts with the Macintosh and the AWS® devices did not have a stylet. Size 3 Glidescope® and Macintosh blades were used in these studies. Optimization maneuvers to facilitate intubation with these devices were also demonstrated, for example, the use of a bougie. Each participant was then allowed five practice intubations with each device, at which stage all students could successfully perform tracheal intubations using all three devices. All intubations were performed with a 7.5-gauge cuffed ETT. As there were three devices in the study, six possible device sequences existed. A randomization list was generated by one of the investigators (JGL) using the random number generator at www.random.org. Fifty-three random numbers, each with a value from 1 to 6 were generated, and the corresponding device order was concealed in a sequentially numbered sealed opaque envelope. Once the novice laryngoscopist had consented to participate in the study, the next envelope in the sequence was opened to reveal the device order. The participant then used the devices in the same order throughout the study.
The design of the study was a three-group three-period randomized crossover design. Each medical student first performed tracheal intubation with each device in a Laerdal® Airway Management Trainer (Laerdal®, Stavanger, Norway) in the following laryngoscopy scenarios: (1) normal airway in the supine position and (2) cervical immobilization. The participants then performed tracheal intubation in a SimMan® manikin (Laerdal®, Kent, UK) in the following scenario, (3) pharyngeal obstruction difficult laryngoscopy. In order to characterize the learning curve at the end of this protocol, each subject performed tracheal intubation of the normal airway a second time with each device in the Laerdal® Airway Management Trainer.
The primary endpoint was the duration of the successful tracheal intubation attempt. The duration of each tracheal intubation attempt was defined as the time taken from insertion of the blade between the teeth until the ETT was connected to an Ambu® bag and lungs were inflated. After each intubation attempt, an investigator verified the position of the ETT tip. A failed intubation attempt was defined as an attempt in which the trachea was not intubated, or where intubation of the trachea required >120 s to perform.
Additional endpoints included the rate of successful placement of the ETT in the trachea, the duration of the first tracheal intubation attempt (whether successful or not), the number of intubation attempts, the number of maneuvers required (readjustment of head position, use of a bougie, second assistant) to aid tracheal intubation, and the severity of dental trauma. The severity of dental trauma was calculated based on the number of audible teeth clicks (0, 1, or ≥2) with the Laerdal® Airway Management Trainer and based on a grading of pressure on the teeth (none = 0, mild = 1, moderate/severe ≥2) in the SimMan® manikin. At the end of each scenario, each participant scored the ease of use of each device on a visual analogue scale (VAS) (i.e., a 10 cm line anchored by the two descriptors, “Extremely Easy” and “Extremely Difficult”).
We based our sample size estimation on the duration of the successful tracheal intubation attempt. Based on a prior study from our group in novice laryngoscopists,17 we projected that the duration of tracheal intubation would be 40 s for the Macintosh laryngoscope, with a standard deviation of 15 s in the easy laryngoscopy scenario with the Macintosh laryngoscope. We considered that an important change in the duration of tracheal intubation would be a 25% absolute change, i.e., a reduction to 30 s or an increase to 50 s. Based on these figures, using α = 0.05 and β = 0.2, for an experimental design incorporating three equal-sized groups, we estimated that 44 participants would be required for a three-group one-way analysis of variance (ANOVA). We therefore aimed to enrol a minimum of 44 students to the study.
We used the statistical package Sigmastat® 3.5 (Systat Software, Inc, Chicago, IL, USA) for these analyses. The distribution of all data was tested for normality using the Kolmogorov–Smirnov test. The data for the duration of the first and the successful tracheal intubation attempts and the VAS device difficulty score were analyzed using the one-way repeated measures ANOVA with device as the repeated measure where the data was normally distributed. Where the data was not normally distributed, a Friedman Repeated Measures ANOVA on ranks was performed with device as the repeated measure. The data for the number of intubation attempts, number of additional maneuvers, and severity of dental compression were analyzed using a Friedman Repeated Measures ANOVA on ranks with device as the repeated measure. Where the ANOVA analysis demonstrated an effect of group, post hoc analyses were carried out using the Student–Newman–Keuls test. Underlying model assumptions were deemed appropriate on the basis of suitable residual plots.
Normally distributed data are presented as means (SD); non-normally distributed data are presented as medians [interquartile range], while ordinal data and categorical data are presented as raw numbers and frequencies. The α level for all analyses was set as P < 0.05.
Results
Fifty-three medical students consented to participate in the study, which was conducted over a 3-month period from October to December 2008. All students were in their final medical year, and no participant had previously performed tracheal intubation.
Scenario 1: Normal airway at start of protocol
Fifty-one (96%) students successfully intubated the trachea with the Macintosh, compared with 52 students with the Glidescope® and all 53 students with the AWS® devices. The duration of both the first and the successful tracheal intubation attempts was shortest with the AWS®, followed by the Glidescope®, and lastly the Macintosh laryngoscope (Table 1, Fig. 2). The number of tracheal intubation attempts was not significantly different between the laryngoscopes (Table 1). The number of optimization maneuvers required was not significantly different between the laryngoscopes. The severity of dental trauma was lowest with the AWS®, of intermediate severity with the Glidescope®, and most severe with the Macintosh laryngoscope (Table 1). The participants found the AWS® easiest to use, the Glidescope® an intermediate level of difficulty, and the Macintosh laryngoscope the most difficult device to use in this scenario (Fig. 3). The point and interval estimates for the mean difference between the devices for the duration of intubation attempts and device difficulty scores are given in Table 2.

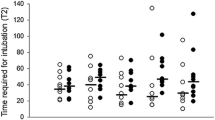
Box plot representing the duration required to successfully intubate the trachea with each device in each scenario tested. The line within the box, represented in grey for the Macintosh laryngoscope, represents the median value, while the outer margins of the boxes represent the interquartile range. * Indicates significantly different (P < 0.05) compared with all other laryngoscopes. Labels: Normal—Start protocol: intubation of the normal airway at the start of the protocol, Left lateral—intubation of the normal airway in the left lateral position, Cervical immobilization—SimMan® cervical spine rigidity scenario; Pharyngeal obstruction—SimMan® pharyngeal obstruction scenario; Normal—End Protocol: intubation of the normal airway at the end of the protocol

Box plot representing the user rated degree of difficulty of use of each instrument in each scenario tested. The line within the box, represented in grey for the Macintosh laryngoscope, represents the median value, while the outer margins of the boxes represent the interquartile range. * Indicates significantly different (P < 0.05) compared with all other laryngoscopes. Labels: Normal—Start protocol: Intubation of the normal airway at the start of the protocol; Left lateral—intubation of the normal airway in the left lateral position; Cervical immobilization—SimMan cervical spine rigidity scenario; Pharyngeal obstruction—SimMan® pharyngeal obstruction scenario; Normal—End protocol: Intubation of the normal airway at the end of the protocol
Scenario 2: Cervical spine immobilization
Forty-seven (89%) students successfully intubated the trachea with the Macintosh, compared with all 53 students with both the Glidescope® and AWS® devices. The duration of both the first and the successful tracheal intubation attempts was shortest with the AWS®, followed by the Glidescope®, and lastly the Macintosh laryngoscope (Table 3, Fig. 2). The number of tracheal intubation attempts was not significantly different between the laryngoscopes (Table 3). The number of optimization maneuvers was significantly different between the devices, with fewer maneuvers required with the AWS® device (Table 3). The severity of dental trauma was lowest with the AWS®, of intermediate severity with the Glidescope®, and most severe with the Macintosh laryngoscope (Table 3). The participants found the AWS® easiest to use, the Glidescope® an intermediate level of difficulty, and the Macintosh laryngoscope the most difficult device to use in this scenario (Fig. 3). The point and interval estimates for the mean difference between the devices for the duration of intubation attempts and device difficulty scores are given in Table 2.
Scenario 3: Pharyngeal obstruction
Forty-five (85%) students successfully intubated the trachea with the Macintosh, compared with all 53 with both the Glidescope® and AWS® devices. The duration of both the first and the successful tracheal intubation attempts was shortest with the AWS®, followed by the Glidescope®, and lastly the Macintosh laryngoscope (Table 4, Fig. 2). Compared with both other laryngoscopes, the number of tracheal intubation attempts was significantly greater with the Macintosh (Table 4). The number of optimization maneuvers was significantly higher with the Macintosh compared with both other devices (Table 4). The severity of dental trauma was found to be lowest with the AWS®, of intermediate severity with the Glidescope®, and most severe with the Macintosh laryngoscope (Table 4). The participants found the AWS® easiest to use, the Glidescope® an intermediate level of difficulty, and the Macintosh laryngoscope the most difficult device to use in this scenario (Fig. 3). The point and interval estimates for the mean difference between the devices for the duration of intubation attempts and device difficulty scores are given in Table 2.
Scenario 4: Normal airway at end of protocol
Fifty-two (98%) students successfully intubated the trachea with the Macintosh, compared with all 53 students with the Glidescope® and the AWS® devices. The duration of both the first and the successful tracheal intubation attempts was shortest with the AWS®, followed by the Glidescope®, and lastly the Macintosh laryngoscope (Table 5, Fig. 2). The number of intubation attempts and the number of maneuvers were not significantly different between the laryngoscopes (Table 5). The severity of dental trauma was lowest with the AWS®, of intermediate severity with the Glidescope®, and most severe with the Macintosh Laryngoscope (Table 5). The participants found the AWS® easiest to use, the Glidescope® an intermediate level of difficulty, and the Macintosh laryngoscope the most difficult device to use in this scenario (Fig. 3). The point and interval estimates for the mean difference between the devices for the duration of intubation attempts and device difficulty scores are given in Table 2.
End of protocol device assessment
The novice laryngoscopists found the AWS® the easiest device to use overall (mean VAS score 2.3 [1.3], P < 0.001), the Glidescope® an intermediate level of difficulty (mean VAS score 3.5 [1.4]), and the Macintosh laryngoscope the most difficult device to use overall (mean VAS score 5.2 [1.6], P < 0.001). The point and interval estimates for the mean difference between the devices are given in Table 2.
Discussion
Securing the airway by inserting an ETT remains the optimal method for assisting ventilation while protecting the airway from the risks of aspiration in unconscious patients. Several studies have demonstrated improved outcome in critically ill and/or injured patients if the airway is secured early by tracheal intubation.1–3 Medical and paramedical personnel may therefore be required to perform tracheal intubation as a lifesaving maneuver in the emergency room or in the prehospital arena. Accordingly, this skill is taught to many healthcare professionals, both medical and paramedical, many of whom may be infrequently required to perform this maneuver.
Part of the difficulty in acquiring the skill of tracheal intubation arises from the limitations of conventional approaches to tracheal intubation. These approaches require the use of direct laryngoscopes, such as the Macintosh laryngoscope, which require the alignment of the oral, pharyngeal, and tracheal axes in order to view the glottic opening. This is a difficult skill to acquire4–6 and maintain successfully,7 particularly if the opportunities to practice this skill are limited, such as in the case of a non-anesthesiologist required to perform tracheal intubation in emergency situations. A slow learning curve for intubation with the Macintosh blade has been well documented among paramedical personnel.4,7 This difficulty is further compounded by the fact that emergent tracheal intubation, e.g., in the prehospital setting, is more difficult to perform with a lower success rate, particularly if performed by inexperienced personnel.18 The occurrence of difficulties and/or failure to intubate the trachea successfully in these situations constitutes an important cause of complications, such as airway trauma, esophageal intubation, hypoxia, pulmonary aspiration, and adverse hemodynamic events.8,9,19
In recent years, advances in optical technologies have facilitated the development of multiple novel indirect laryngoscopes. A common feature of these devices is that they visualize the glottis by indirect mechanisms, obviating the need to align the oral, pharyngeal, and tracheal axes and thereby potentially making laryngeal visualization and subsequent tracheal intubation easier to perform. The Glidescope® 13 and the AWS® device10 are two indirect laryngoscopes each with features that may make them likely to require less operator skill to use compared with the Macintosh laryngoscope. The AWS® has been shown to reduce the time to secure the airway and to decrease the incidence of failed tracheal intubation by novice laryngoscopists.14 In contrast, the efficacy of the Glidescope® in novice laryngoscopists is not clear. Furthermore, the relative efficacies of these devices when used by novice personnel have not been compared in a single study. We wanted to evaluate the relative efficacies of these novel laryngoscopes when used by novice laryngoscopists in a series of progressively more difficult tracheal intubation scenarios and to compare these devices with the gold standard Macintosh laryngoscope. In this study, we utilized medical students for this purpose, as we could be certain they had not received prior training in the use of any of the devices, including the Macintosh laryngoscope.
Our previous studies have demonstrated that the Glidescope® reduces the difficulty of tracheal intubation in direct comparisons with the Macintosh laryngoscope when used by experienced anesthesiologists.16,20 This study extends these findings to novice laryngoscopists and demonstrates that the Glidescope® increased tracheal intubation success rates, reduced the time required to perform tracheal intubation, reduced the need for additional maneuvers, reduced the potential for dental trauma, and was considered easier to use compared with the Macintosh laryngoscope in both normal and difficult intubation scenarios. However, the Glidescope® performed less favourably in comparison with the AWS® device in all scenarios tested in this study. The less favourable performance of the Glidescope® in comparison with the AWS® device appears to be due to difficulties encountered in advancing the tracheal tube toward the view of the video-monitor with the Glidescope®, a finding previously reported by other investigators.13 As described by Sun et al., we utilized a “hockey-stick” J-curvature of the stylet at the end of the tube and passed the tube from the lateral side of the patient’s mouth,13 and we found that this approach worked well. Despite this approach, these difficulties appeared to be the principal reason for the increased duration of tracheal intubation in comparison with the AWS® device.
The Pentax AWS® laryngoscope has recently been introduced into clinical practice. Recent manikin15 and clinical studies10,16 indicate that this device may have advantages over the Macintosh. This device also appears to cause less cervical spine movements during tracheal intubation when compared with the Macintosh or McCoy® laryngoscopes.21 In this study in novice laryngoscopists, the Pentax AWS® performed most favourably of the devices studied. In all airway scenarios, the Pentax AWS® reduced the duration required to perform tracheal intubation, reduced the need for maneuvers, and possessed the least potential for dental compression compared with the other laryngoscopes studied. The potential for the Pentax AWS® laryngoscope to cause less dental compression has been previously reported when this device is used by nonanesthesiologist physicians.14 Our finding that the Pentax AWS® reduced tracheal intubation times agrees with one14 but does not agree with a second22 prior study in novice users. Of particular interest, the duration of intubation attempts with the AWS® compared well with that recorded by experienced anesthesiologists in our recent study.23 This finding highlights the ease of use and the short learning curve associated with this device for both experienced and inexperienced laryngoscopists. The medical students also found the AWS® easier to use than the Glidescope® and Macintosh laryngoscopes. The Pentax AWS® may also have advantages for other personnel who are infrequently required to perform tracheal intubation, such as emergency room staff. While this study does not directly examine this issue, the fact that the device exhibits a rapid learning curve, despite a deliberately brief instruction period, supports this contention.
A key difference between the Pentax AWS® laryngoscope and the Glidescope® is the fact that it possesses a side channel through which the ETT is placed prior to commencing the intubation attempt. Once the device is inserted, the glottis is visualized and centered on the target mark on the screen, and the ETT is then passed through the glottis. This channel, also a feature in the Airtraq® laryngoscope (which has been shown to perform favourably in comparison with other novel indirect laryngoscopes in similar studies), facilitates the passage of the ETT into the glottis.17,23–26 This relative ease of advancing the ETT via the channel through the glottis contrasts with difficulties reported with the Glidescope® in advancing the tracheal tube toward the view seen in the monitor.13 It should be noted, however, that there are disadvantages to incorporating a side channel into the laryngoscope blade, particularly the inability to independently manipulate the laryngoscope and the ETT and its relative bulkiness compared with blades that do not incorporate a side channel.
The Pentax AWS® and the Glidescope® have single-use disposable blades, removing the potential for transmission of prions that are thought to be responsible for causing variant Creutzfeldt-Jakob disease.27,28 This complies with the guidelines of the Association of Anaesthetists of Great Britain and Ireland, which state that “single use intubation aids” should be used where possible29 due to difficulties in ensuring that all proteinaceous material has been removed during cleaning and sterilization.27,30
A number of important limitations exist regarding this study. First, we acknowledge that some potential for bias exists, as it is impossible to blind the novice laryngoscopists to the device being used. Second, our focus in this study was to determine the utility of these novel laryngoscopes compared with the Macintosh for the novice user, rather than for the occasional or inexperienced user. As novices have not received prior training with any laryngoscope, there is no risk of bias of the study findings as a result of prior learning and experience with the Macintosh laryngoscope. However, the findings may differ in studies carried out in occasional and/or inexperienced laryngoscopists, an important group of healthcare providers, particularly in the emergency setting. Third, there exists the potential for a period of carryover effects, whereby learning from the use of one device or earlier scenario might impact on performance with another device or later laryngoscopy scenario. We consider the risk of period effects to be low because we used a randomization procedure that ensured that similar numbers of participants used the devices in each of the six possible sequences. We would expect that any such effects would be evenly dispersed across the devices. In any case, the three devices tested are sufficiently different in design that it would not be expected that any one sequence order would be advantageous over another. Lastly, this is a manikin study and may not adequately mimic clinical conditions. An issue of particular relevance is the risk, which is not seen in manikins, of fogging and contamination of the lens of indirect laryngoscopes by secretions in the clinical setting. Therefore, these findings need to be confirmed and extended in clinical studies before definitive conclusions can be drawn. Finally, the relative efficacies of these devices in comparison with other promising devices, such as the McCoy®,31 McGrath®,25 or Bonfils®,32 have not been determined.
In conclusion, the AWS® and the Glidescope® laryngoscopes both possess advantages over the conventional Macintosh laryngoscope when used by novice laryngoscopists. In this manikin study, the AWS® laryngoscope performed remarkably in both the normal and difficult airway scenarios. Further clinical studies are necessary to confirm these initial positive findings.
References
Winchell RJ, Hoyt DB. Endotracheal intubation in the field improves survival in patients with severe head injury. Trauma Research and Education Foundation of San Diego. Arch Surg 1997; 132: 592–7.
Garner A, Rashford S, Lee A, Bartolacci R. Addition of physicians to paramedic helicopter services decreases blunt trauma mortality. Aust N Z J Surg 1999; 69: 697–701.
Sanson G, Di Bartolomeo S, Nardi G, et al. Road traffic accidents with vehicular entrapment: incidence of major injuries and need for advanced life support. Eur J Emerg Med 1999; 6: 285–91.
Wang HE, Seitz SR, Hostler D, Yealy DM. Defining the learning curve for paramedic student endotracheal intubation. Prehosp Emerg Care 2005; 9: 156–62.
Gerbeaux P. Should emergency medical service rescuers be trained to practice endotracheal intubation? Crit Care Med 2005; 33: 1864–5.
Mulcaster JT, Mills J, Hung OR, et al. Laryngoscopic intubation: learning and performance. Anesthesiology 2003; 98: 23–7.
Garza AG, Gratton MC, Coontz D, Noble E, Ma OJ. Effect of paramedic experience on orotracheal intubation success rates. J Emerg Med 2003; 25: 251–6.
Mort TC. Esophageal intubation with indirect clinical tests during emergency tracheal intubation: a report on patient morbidity. J Clin Anesth 2005; 17: 255–62.
Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg 2004; 99: 607–13.
Enomoto Y, Asai T, Arai T, Kamishima K, Okuda Y. Pentax-AWS, a new videolaryngoscope, is more effective than the Macintosh laryngoscope for tracheal intubation in patients with restricted neck movements: a randomized comparative study. Br J Anaesth 2008; 100: 544–8.
Cooper RM. Use of a new videolaryngoscope (GlideScope) in the management of a difficult airway. Can J Anesth 2003; 50: 611–3.
Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new videolaryngoscope (GlideScope) in 728 patients. Can J Anesth. 2005; 52: 191–8.
Sun DA, Warriner CB, Parsons DG, Klein R, Umedaly HS, Moult M. The GlideScope Video Laryngoscope: randomized clinical trial in 200 patients. Br J Anaesth 2005; 94: 381–4.
Hirabayashi Y, Seo N. Tracheal intubation by non-anaesthetist physicians using the Airway Scope. Emerg Med J 2007; 24: 572–3.
Malik MA, O’Donoghue C, Carney J, Maharaj CH, Harte BH, Laffey JG. Comparison of the Glidescope, the Pentax AWS, and the Truview EVO2 with the Macintosh laryngoscope in experienced anaesthetists: a manikin study. Br J Anaesth 2009; 102: 128–34.
Malik MA, Subramaniam R, Churasia S, Maharaj CH, Harte BH, Laffey JG. Tracheal intubation in patients with cervical spine immobilization: a comparison of the Airwayscope®, LMA CTrach® and the Macintosh laryngoscopes. Br J Anaesth 2009; 102: 654–61.
Maharaj CH, Costello JF, Higgins BD, Harte BH, Laffey JG. Learning and performance of tracheal intubation by novice personnel: a comparison of the Airtraq® and Macintosh laryngoscope. Anaesthesia 2006; 61: 671–7.
Adnet F, Jouriles NJ, Le Toumelin P, et al. Survey of out-of-hospital emergency intubations in the French prehospital medical system: a multicenter study. Ann Emerg Med 1998; 32: 454–60.
Schlossmacher P, Martinet O, Testud R, Agesilas F, Benhamou L, Gauzere BA. Emergency percutaneous tracheostomy in a severely burned patient with upper airway obstruction and circulatory arrest. Resuscitation 2006; 68: 301–5.
Malik MA, Maharaj CH, Harte BH, Laffey JG. Comparison of Macintosh, Truview EVO2, Glidescope, and Airwayscope laryngoscope use in patients with cervical spine immobilization. Br J Anaesth 2008; 101: 723–30.
Maruyama K, Yamada T, Kawakami R, Kamata T, Yokochi M, Hara K. Upper cervical spine movement during intubation: fluoroscopic comparison of the AirWay Scope, McCoy laryngoscope, and Macintosh laryngoscope. Br J Anaesth 2008; 100: 120–4.
Miki T, Inagawa G, Kikuchi T, Koyama Y, Goto T. Evaluation of the Airway Scope, a new video laryngoscope, in tracheal intubation by naive operators: a manikin study. Acta Anaesthesiol Scand 2007; 51: 1378–81.
Maharaj CH, Higgins BD, Harte BH, Laffey JG. Evaluation of intubation using the Airtraq® or Macintosh laryngoscope by anaesthetists in easy and simulated difficult laryngoscopy—a manikin study. Anaesthesia 2006; 61: 469–77.
Maharaj CH, Costello J, Higgins BD, Harte BH, Laffey JG. Retention of tracheal intubation skills by novice personnel: a comparison of the Airtraq® and Macintosh laryngoscopes. Anaesthesia 2007; 62: 272–8.
Maharaj CH, McDonnell JG, Harte BH, Laffey JG. A comparison of direct and indirect laryngoscopes and the ILMA in novice users: a manikin study. Anaesthesia 2007; 62: 1161–6.
Maharaj CH, Ni Chonghaile M, Higgins BD, Harte BH, Laffey JG. Tracheal intubation by inexperienced medical residents using the Airtraq® and Macintosh laryngoscope—a manikin study. Am J Emerg Med 2006; 24: 769–74.
Lowe PR, Engelhardt T. Prion-related diseases and anaesthesia. Anaesthesia 2001; 56: 485.
Will RG, Ironside JW, Zeidler M, et al. A new variant of Creutzfeldt-Jakob disease in the UK. Lancet 1996; 347: 921–5.
Infection control in Anaesthesia. London: The Association of Anaesthetists of Great Britain and Ireland; 2002.
Miller DM, Youkhana I, Karunaratne WU, Pearce A. Presence of protein deposits on ‘cleaned’ re-usable anaesthetic equipment. Anaesthesia 2001; 56: 1069–72.
Uchida T, Hikawa Y, Saito Y, Yasuda K. The McCoy levering laryngoscope in patients with limited neck extension. Can J Anaesth 1997; 44: 674–6.
Rudolph C, Schneider JP, Wallenborn J, Schaffranietz L. Movement of the upper cervical spine during laryngoscopy: a comparison of the Bonfils intubation fibrescope and the Macintosh laryngoscope. Anaesthesia 2005; 60: 668–72.
Acknowledgments
We sincerely thank Pentax Ltd. for the provision of the AWS® device.
Funding
Pentax Ltd provided the AWS® device and disposable blades free of charge. All other support was derived solely from institutional and/or departmental sources.
Conflicts of interest
The authors have no conflict of interest regarding the AWS® and Glidescope® devices.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Malik, M.A., Hassett, P., Carney, J. et al. A comparison of the Glidescope®, Pentax AWS®, and Macintosh laryngoscopes when used by novice personnel: a manikin study. Can J Anesth/J Can Anesth 56, 802–811 (2009). https://doi.org/10.1007/s12630-009-9165-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-009-9165-z