Article Text

Abstract
There is no firm evidence from randomised controlled trials that routine monitoring of lung function improves asthma control in children. Guidelines for management of asthma consistently recommend routine home monitoring of peak expiratory flow (PEF) in each patient. However, changes in PEF poorly reflect changes in asthma activity, PEF diaries are kept very unreliably, and self management programmes including PEF monitoring are no more effective than programmes solely based on education and symptom monitoring. PEF diaries may still be useful in isolated cases of diagnostic uncertainty, in the identification of exacerbating factors, and in the rare case of children perceiving airways obstruction poorly and exacerbating frequently and severely. If a reliable assessment of airways obstruction in asthma is needed, forced expiratory flow-volume curves are the preferred method. Monitoring of hyperresponsiveness and nitric oxide cannot be recommended for routine use at present. Clinical judgement and expiratory flow-volume loops remain the cornerstone of monitoring asthma in secondary care.
- asthma
- lung function
- monitoring
- AH, airways hyperresponsiveness
- FEV, forced expiratory volume
- MEF, mean expiratory flow
- PEF, peak expiratory flow
Statistics from Altmetric.com
- AH, airways hyperresponsiveness
- FEV, forced expiratory volume
- MEF, mean expiratory flow
- PEF, peak expiratory flow
The most characteristic lung function abnormality in children with asthma is airways obstruction. Guidelines for the management of asthma in school age children and adolescents stress the importance of objective assessment of “lung function” (more specifically, airways obstruction), both in the initial assessment and in individual patient follow up.1,2 The rationale for this recommendation comes from two consistent research findings, namely that many patients (including children) with asthma are poor perceivers of (changes in) airway calibre, and that airways obstruction in childhood is a poor prognostic factor for the outcome of asthma into adulthood.
WHY MONITOR LUNG FUNCTION
Poor perception of airway calibre in asthma
Considerable airways obstruction may be present in asymptomatic patients with asthma.3 Children with long-standing airways obstruction are less likely to report dyspnoea than children with acute onset of airways obstruction.4 Such poor perceivers are more likely to present with hypoxia during an acute exacerbation,5 predisposing to severe or life threatening attacks. Thus, evidence supports the hypothesis that poor perception of airways obstruction is a clinically relevant problem in children with asthma.
Reduced lung function as a prognostic factor of outcome
A recent retrospective study of 13 482 children with asthma showed that children with significant airways obstruction (defined as a forced expiratory volume in one second (FEV1) <60% of predicted) were twice as likely to develop an asthmatic attack in the subsequent year than children with more or less normal lung function (FEV1 >80% of predicted).6 A large body of evidence shows that airways obstruction in children with asthma is associated with ongoing respiratory morbidity and a reduced FEV1 in adulthood, both in general population based cohorts of children with mild disease,7,8 and in hospital based cohorts of patients with more severe asthma.9,10 Thus, airways obstruction in children with asthma has both short term and long term prognostic significance.
MONITORING LUNG FUNCTION IN ASTHMA: CIRCUMSTANTIAL AND DIRECT EVIDENCE
The rationale for the recommendation to monitor lung function (airways obstruction) routinely in childhood asthma is apparently based on firm evidence: poor perception of airway calibre and reduced lung function are both associated with poor outcomes in asthmatic children, and both prognostic factors can only be identified by assessing lung function. This evidence, however, is circumstantial, and it only supports measuring lung function in the initial assessment, not routine monitoring of lung function in the follow up of outpatients. The best way to obtain direct evidence on the usefulness of monitoring lung function in childhood asthma is to perform a randomised controlled trial in which monitoring of symptoms only is compared to monitoring of symptoms plus lung function, and in which control of asthma is the primary outcome parameter (fig 1). Such a randomised controlled trial showing the usefulness of routine monitoring of lung function in children with asthma has not been published to date. Hence, so far the guidelines’ recommendation to monitor lung function routinely in asthmatic children is not substantiated by direct evidence from randomised trials (class I evidence in the terminology of evidence based medicine). In the remainder of this review, we will discuss the available evidence on the usefulness of monitoring lung function in asthma in a narrative fashion. We wish to stress that the practice points drawn from this evidence are largely based on class II (non-randomised trials) and III evidence (anecdotal findings and expert opinion), and on our own clinical experience, and are open for debate.
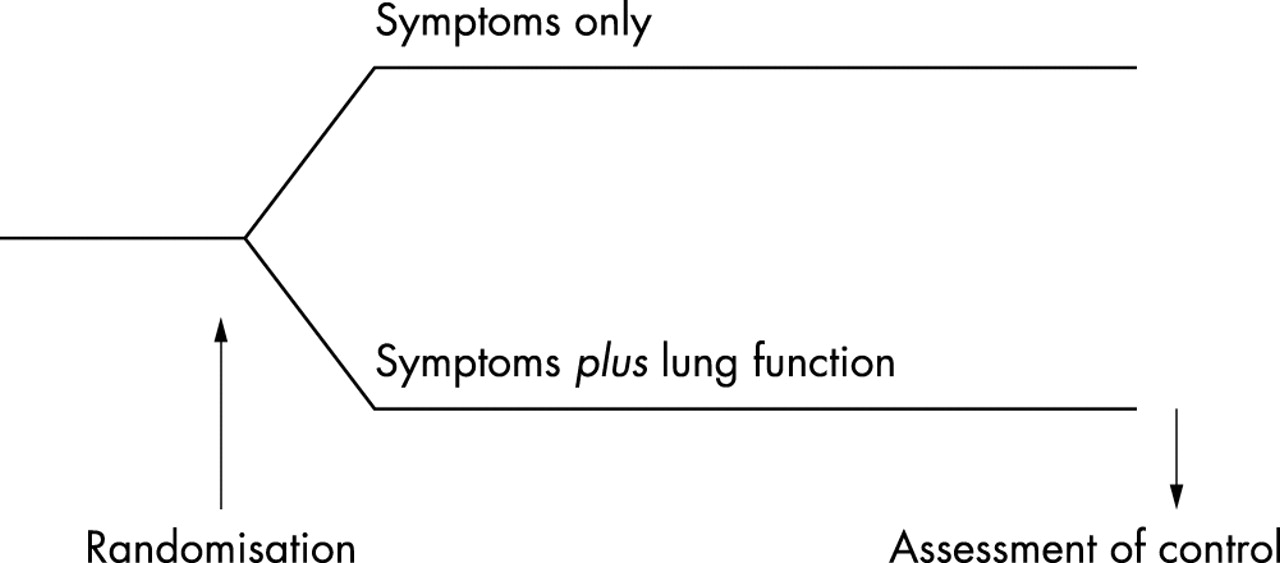
Design of the clinical trial needed to test the hypothesis that monitoring of lung function in childhood asthma is useful. Such studies are rare in children, and no such studies have been published showing usefulness of routine lung function monitoring.
PEAK EXPIRATORY FLOW
Peak expiratory flow (PEF) is the most commonly used method to monitor lung function in asthma, because it can be measured easily by simple, cheap, portable devices. It is, therefore, very popular in primary care. It is commonly applied as a quick screening method of assessing lung function in the clinic or at the bedside, but is most frequently used as a tool for home monitoring of changes in lung function.
Isolated PEF measurements in the clinic or at the bedside
PEF can be measured quickly and repeatably under supervision in the office or at the bedside on the ward.11 It should be noted, however, that PEF is primarily a measure of large airways calibre, while the obstruction in asthma is most pronounced in small airways. A normal PEF does not rule out significant airways obstruction (fig 2).12,13 The other drawback of isolated PEF measurements is that the variation of PEF values between healthy children is large.14 Comparison to reference values is, therefore, unlikely to be helpful; comparison to previous measurements in the same patient may be useful, but it should be stressed that isolated PEF measurements in the clinic are at best a very rough screening method for airways obstruction in asthma. If a reliable and accurate assessment of airways obstruction is needed, parameters such as FEV1 and the mean expiratory flow between 25% and 75% of expired vital capacity (MEF25–75) should be preferred.12,13 Eyeballing a complete expiratory flow-volume curve (fig 2) will provide similar information.15

Flow-volume curve of a child with asthma, showing the characteristic concave expiratory pattern with markedly reduced mid-expiratory flow rates. The reference values for peak expiratory flow (PEF), mid-expiratory flows at 25%, 50%, and 75% (MEF25–75) of forced vital capacity (FVC), and the FVC itself are represented by squares, and are connected by a dashed line representing a hypothetical “normal” expiratory flow-volume curve. The FEV1 can not be read directly from a flow-volume curve because there is no time axis, but the spirometer software will provide it. In this case, the FEV1 was 71% of the predicted value. Note that despite considerable airways obstruction, PEF is normal.
Home monitoring of PEF
Repeated measurements at home allow assessment of diurnal and day-to-day variation of airway calibre, which is one of the cardinal features of asthma.1,2 Studies showing improved outcomes of asthma when patients completed a self management programme including home monitoring of PEF have been viewed as supporting the usefulness of home PEF monitoring.16–19 However, the interventions in these studies included not only home PEF monitoring, but also comprehensive patient education. There is accumulating evidence that patient education is one of the key factors determining good asthma control.20 In fact, a randomised controlled trial showed that education alone was associated with a significant reduction in emergency room visits in the subsequent year,21 comparable to that observed in studies using more comprehensive self management plans including home PEF monitoring.18,19 This suggests that it is the education rather than the PEF monitoring that determines the success of asthma self management plans. In direct comparisons of symptom based and PEF based self management plans of adult asthmatics, both approaches have been found to be comparable in terms of asthma control.22,23 In a report on a similar study in children it was stated that children using a PEF meter had better asthma control after three months of follow up than children who did not use a PEF meter.24 This difference, however, was not statistically significant (p ⩾ 0.07) and was not maintained during further follow up (fig 3).
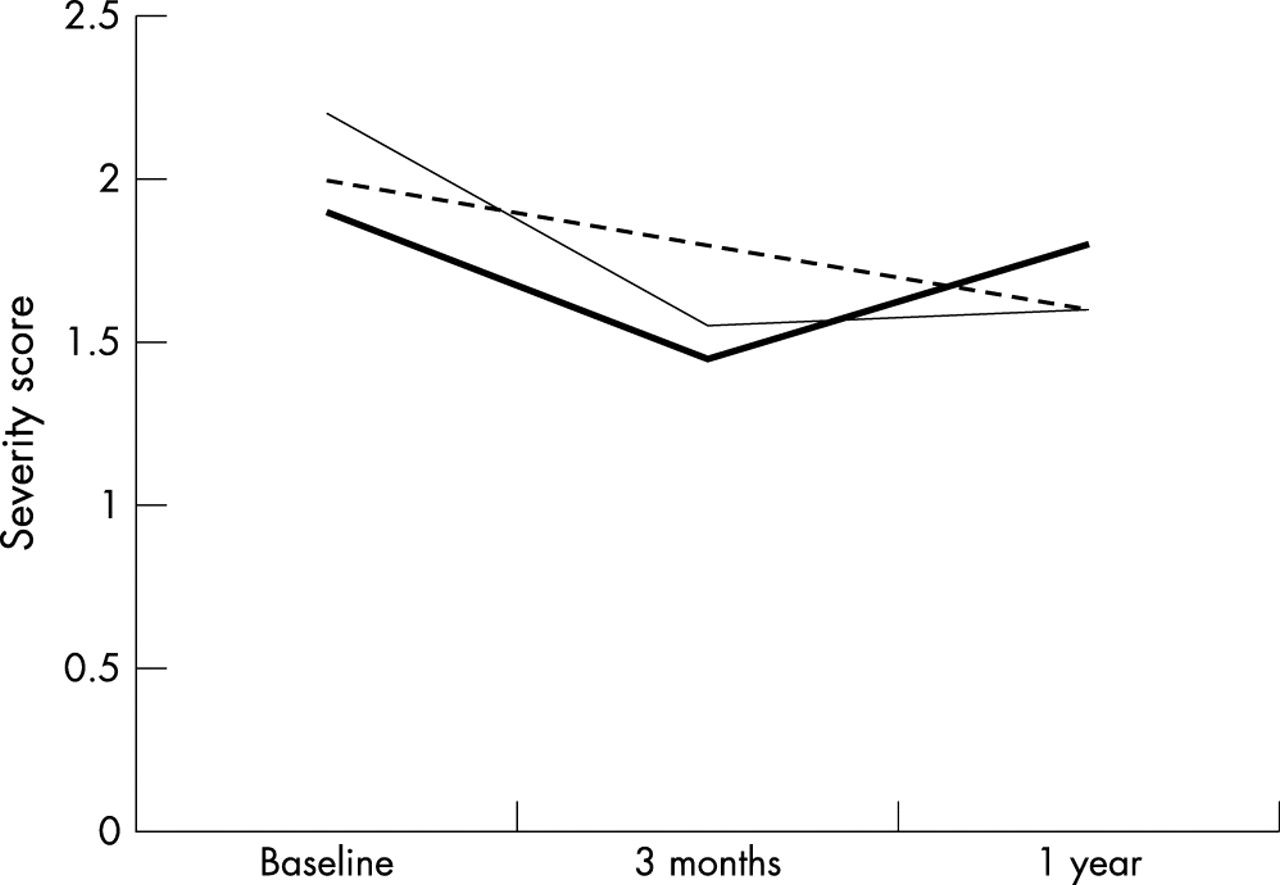
Asthma severity scores in three groups of asthmatic children, one monitoring symptoms only (dashed line), one monitoring peak expiratory flow (PEF) at home on a daily basis (thin solid line), and one monitoring PEF at home only when symptomatic for one year. Although there was a trend towards a difference in asthma severity between symptom only monitoring and PEF monitoring after three months (p = 0.07) this difference disappeared during further follow up (after Yoos et al24).
The unreliability of PEF diaries is probably one of the main reasons why PEF monitoring does not contribute as much to the success of asthma self management as one would assume intuitively.25 Recently, we showed that up to 50% of entries in PEF diaries of affluent white asthmatic children whom we considered to be “model patients” were either invented or falsified.26 In clinical practice, therefore, patients are unlikely to use their PEF meters routinely on a daily basis,27 and will probably not provide reliable and meaningful PEF diaries.
Thus, there is good evidence (class I to II) that the guidelines’ recommendation of routine home monitoring of PEF in each patient with asthma is not justified. Does this mean that we should abandon home PEF monitoring altogether? We don’t think so. Both clinical experience and published anecdotal evidence suggest a role for targeted, short term PEF monitoring in the diagnosis of asthma,28,29 and in identifying triggers of asthma.15 In our practice, we only use home PEF monitoring in rare cases of diagnostic uncertainty and unstable asthma when exacerbating factors remain unclear. Such diagnostic PEF monitoring is always applied for a short term period, and only after careful instruction by the asthma nurse who demonstrates and checks PEF technique, and who stresses that the diary should only contain truly blown and carefully recorded values.
In our practice of hundreds of asthmatic children, we only have one patient on long term home PEF monitoring. This is a patient with poor perception of airways obstruction who exacerbates frequently and rather severely. This child appears to benefit from home PEF monitoring in that, during an exacerbation, she now tends to present at an earlier stage.
In primary care, when lung function apparatus for obtaining expiratory flow-volume loops is not available, repeated isolated PEF measurements in the same patient may be used to screen for airways obstruction. As outlined above, this provides only a rough estimate, which should be interpreted with caution.
FEV1 AND FLOW-VOLUME CURVES
The FEV1 is considered to be the “gold standard” of measuring airways obstruction, because its measurement has been well standardised,30 the measurement can be performed repeatably, and reliable reference values are available (FEV1 is usually expressed as a percentage of the “predicted” reference values: FEV1%pred). These attributes make the FEV1 very popular as an outcome parameter in clinical studies, and practitioners feel confident in interpreting FEV1 values as an assessment of the degree of airways obstruction in clinical practice. However, the FEV1 only reflects limited information on the complex process of forced expiration through obstructed airways.31 Experienced clinicians will prefer to “eyeball” a flow-volume curve in their assessment of the severity of airways obstruction in asthma (fig 2). A detailed description of this process, along with numerous practical examples, has been published previously.15 In our practice, we both eyeball the flow-volume curve and record numerical values for FEV1%pred (which may be normal despite a concave pattern in the flow-volume curve).
There is no evidence from randomised controlled trials (fig 1) that monitoring FEV1 in childhood asthma helps in improving asthma control. In contrast to PEF, there is also no evidence that it is not. Abundant published anecdotal evidence underscores the usefulness of measuring FEV1 or obtaining flow-volume curves in the initial diagnostic work-up of asthma, in particular when it is repeated after administration of a bronchodilator.15,32,33 In our experience, explanation of the results of flow-volume curves before and after bronchodilator to patients and parents has considerable educational value, both during the initial work-up and during long term follow up. This is one of the reasons why children with chronic persistent asthma under our care will perform flow-volume curves before and after bronchodilator at least once yearly. Computer incentives in modern spirometry software allow reproducible flow-volume curves to be obtained in the majority of children from the age of 4 onwards.34,35
AIRWAYS HYPERRESPONSIVENESS
Airways hyperresponsiveness (AH), the exaggerated constriction of airways in response to exogenous stimuli, is one of the hallmarks of asthma. It can be measured in the laboratory either by direct (such as histamine or methacholine, which cause airway smooth muscle contraction directly) or indirect stimuli (such as exercise or adenosine, which cause bronchoconstriction via inflammatory or neuronal pathways). The latter are more specific for asthma than the former.36 The response is usually measured by repeated FEV1 measurements, and expressed as the dose (PD20) or concentration (PC20) of the stimulus required to decrease FEV1 by 20%.
Although there is considerable overlap in AH between healthy and asthmatic children,37 measurement of AH can be quite helpful in the initial diagnostic work-up of children with asthma, in particular in secondary care.15,36 Indirect evidence to support a role for monitoring of AH in asthma comes from two observations. Firstly, during treatment with inhaled corticosteroids, symptoms and airways obstruction usually resolve completely within weeks, while improvements in AH continue for many months.38 Secondly, the degree of AH correlates strongly with inflammatory cell counts in bronchoalveolar lavage fluid, suggesting that AH can be viewed as an indrect measure of airways inflammation.39
A randomised controlled trial (fig 1) in 75 adult asthmatics showed that patients in whom the degree of AH was used to guide anti-inflammatory treatment had fewer exacerbations and a more pronounced improvement of inflammatory changes in bronchial biopsy specimens than patients in whom the dose of (inhaled) corticosteroids was only guided by symptoms and FEV1.40 This strongly suggests that monitoring AH in the long term management of asthma in adults is useful. Whether this also applies to children is currently under investigation in a multicentre trial in the Netherlands. Drawbacks of repeated AH measurements are that they are quite a burden to patients (a methacholine challenge takes approximately 45–60 minutes to perform and may cause temporary discomfort to the child) and to human resources in the lung function laboratory (an exercise test requires the presence of up to two technicians for 30–60 minutes).
OTHER MEASUREMENTS OF LUNG FUNCTION: VITAL CAPACITY, RESIDUAL VOLUME, INTERRUPTER RESISTANCE, AND NITRIC OXIDE
A detailed description of the various other techniques to assess pulmonary function is beyond the scope of this paper. No studies have formally examined the usefulness of any of these techniques in the long term management of asthma.
Vital capacity and residual volume
Studies have shown that many asthmatics have increased residual volumes and air trapping with normal FEV1 values.41 Although this suggests ongoing disease even in the absence of manifest airways obstruction, it has never been established that treating these abnormalities with aggressive anti-inflammatory therapy is clinically useful. Hence, it appears that monitoring static lung volumes such as vital capacity and residual volume is not needed. We tend to measure residual volumes by helium dilution and body plethysmography only in severe asthmatics, and no more often than biannually.
Interrupter resistance
Over the past few years, a novel technique to assess respiratory resistance (an indirect measure of airways obstruction) in preschool children with a simple portable interrupter device has become available.42 Reference values from the UK and the Netherlands have recently been published.43,44 The technique appears to be reproducible, and results are sensitive to change induced by treatment.42 It appears promising, therefore, as a method to assess airways obstruction in preschool children. Its usefulness as a tool to monitor asthma in these young children has not been shown in studies or in clinical practice to date.
Nitric oxide
Perhaps one of the most promising developments is measurement of nitric oxide in exhaled air (eNO), because this appears to reflect lower airways inflammation.45 The technique is now well standardised for use in school aged children,46 and reference values for healthy children are available.47,48
Values of eNO in untreated asthmatics are much higher than those of healthy children. Because of these highly significant differences and because the association between eNO values and direct assessments of airways inflammation in adults, it has been claimed that monitoring of eNO in asthma is useful (“inflammometry”).45 Until now, no direct evidence to substantiate this claim (fig 1) is available, however.
PRACTICE POINTS
Peak expiratory flow
-
Isolated measurements of PEF provide an insensitive and, therefore, not very useful assessment of airway obstruction
-
There is good evidence that routine home monitoring of peak flow in each asthmatic child is not justified and not useful
-
Home peak flow monitoring may be useful in rare isolated cases of diagnostic uncertainty (is this asthma?) or when exacerbating factors remain unclear, and in poor perceivers with severe or frequent exacerbations
-
Only apply home PEF monitoring after careful instruction by an asthma nurse, stressing the importance of honest and careful diary keeping
FEV1
-
Isolated measurements of FEV1 provide a well standardised and sensitive assessment of airways obstruction and response to bronchodilators
-
Monitoring FEV1 repeatably during scheduled follow up visits has educational value
Airways hyperresponsiveness
-
Evidence suggests that monitoring airways hyperresponsiveness in asthma is useful, but the burden of repeated testing limits its applicability in practice
Vital capacity, residual volume, interrupter resistance, and exhaled nitric oxide
-
There is insufficient evidence to recommend monitoring in clinical practice
During treatment with inhaled corticosteroids, eNO values return to normal rapidly. In almost all studies, eNO values of asthmatics treated with inhaled corticosteroids are indistinguishable from those of healthy subjects.45 Although there is some evidence that in adults the response of eNO to inhaled corticosteroids may be dose dependent,49 this does not appear to be the case in children (fig 4).50 Therefore, monitoring of eNO in childhood asthma cannot yet be recommended for clinical practice.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Nitric oxide levels in exhaled air (eNO) in asthmatic children, treated for one year with a constant dose of fluticasone (thin line, open squares) or a stepdown schedule with a high starting dose tapering off to a low maintenance dose (thick line, solid circles). Run-in: six week period during which all patients inhaled 200 μg/day fluticasone by dry powder inhaler. No ICS: wash-out period of 2–4 weeks during which no inhaled corticosteroids were used. The results show no effect of the dose of fluticasone on eNO levels. After Visser et al.50
CONCLUSIONS
Although consistently recommended in asthma guidelines and widely used in practice, we feel that home peak flow monitoring is not needed or justified in the management of the large majority of children with asthma. Changes in peak flow are a poor indicator of changes in disease activity, diaries are not kept reliably, and peak flow based self management plans are not superior to self management plans based on education and symptoms. At present, the best way to assess and follow airways obstruction in asthmatic children is by eyeballing flow-volume loops and measuring FEV1 in the lung function laboratory. Although monitoring of airways hyperresponsiveness and nitric oxide look promising in clinical studies, these measurements cannot be recommended for use in clinical practice at present. Future studies are needed to evaluate whether home monitoring of FEV1 and PEF by electronic devices, which do not require fraud prone diary keeping, contribute to obtaining optimal control. Until then, clinical judgement, common sense, and flow-volume loops remain the most important tools in monitoring asthma.
Acknowledgments
The authors wish to thank professor Johan de Jongste for allowing us to use his scheme (fig 1) in this paper.