Article Text

Abstract
AIM To investigate the efficacy of nasal high frequency ventilation (nHFV) in newborn infants with moderate respiratory insufficiency.
METHOD Twenty one preterm and term neonates were treated with nHFV for respiratory insufficiency. Criteria for starting nHFV were: deterioration on nasal CPAP expressed by a median pH of 7.24 and pCO2 of 8.3 kPa, or increasing FIO2. nHFV was delivered using the Infant Star ventilator. Ventilator setting amplitude was 35 cm H2O; mean airway pressure 7 cm H2O; and frequency 10 Hz.
RESULTS pCO2decreased significantly from 8.3 kPa to 7.2 kPa after nHFV was started. In five patients nHFV was discontinued after a median period of 6½ hours due to CO2 retention and high oxygen need, and endotracheal mechanical ventilation was started.
CONCLUSIONS nHFV can reduce pCO2 in neonates with moderate respiratory insufficiency and, therefore, could be used to decrease the need for endotracheal mechanical ventilation.
- nasal high frequency ventilation
- idiopathic respiratory distress syndrome
Statistics from Altmetric.com
Over the past two decades assisted mechanical ventilation has been used to manage respiratory insufficiency in newborn infants. However, complications such as airleaks occur in 15 to 48% of the infants who need ventilator support,1 2 and 5 to 25% develop broncho-pulmonary dysplasia (BPD).3 Both these complications contribute substantially to morbidity in preterm infants. Therefore, a less invasive approach such as nasal continuous positive airway pressure (nCPAP) is frequently used in the initial management of respiratory insufficiency.4-6 But 43 to 80% of the neonates with moderate to severe respiratory insufficiency, initially treated with nasal CPAP, will need subsequent mechanical ventilation.7 Nasal CPAP has also been used after extubation to facilitate weaning from mechanical ventilation.8-11 However, extubation failed in 16 to 40% of cases. In both events subsequent endotracheal mechanical ventilation was needed because of CO2 retention or increased oxygen need and apnoea of prematurity.
High frequency ventilation (HFV) is a new method of mechanical ventilation based on the delivery of small tidal volumes at a supraphysiological respiratory frequency of 10 Hz.12 13This technique is very effective in eliminating carbon dioxide and is independent of dead space.
We hypothesised that HFV applied on a single nasopharyngeal tube (nHFV) might reduce pCO2 by augmenting CO2 diffusion in the pharynx and larynx area and, therefore, decreasing the need for subsequent mechanical ventilation. To test this hypothesis we performed a non-controlled observational study and tested the efficacy of nHFV in infants with moderate respiratory insufficiency.
Methods
Twenty one newborn infants were offered nHFV. All patients were initially treated with nasal CPAP applied via a single nasopharyngeal tube positioned at a depth of 3–4 cm. nHFV was started due to CO2 retention (median value 8.3 kPa), acidosis (median pH value 7.24), and/or increasing oxygen need (median FIO20.42) during nasal CPAP. We applied nHFV via the same nasopharyngeal tube by switching the ventilator (Infant Star HFV, Infrasonics, Inc. San Diego, CA, USA) to the HFV mode. This ventilator delivers HFV by flow interruption. NHFV was initiated with the following parameters: mean airway pressure (Pāw) was maintained or increased to a higher level; frequency of 10 Hz and amplitude was increased until the infant’s chest showed oscillations; FIO2 was regulated to achieve a peripheral oxygen saturation monitored by pulse oximetry of 86–93%.14-15 Arterial or capillary blood gases and ventilator settings were registered at a median time of 4¼ hours (3.28–6.25 hours) and of 0.57 hours (0.34–1.57 hours) before and 1½ hours (0.50–2 hours), 4.24 hours (3.20–5.20 hours), 7.38 hours (6.52–8 hours), and 11 hours (10–13 hours) after nHFV initiation. Endotracheal mechanical ventilation was considered when blood gases further deteriorated: pH < 7.20; pCO2 > 8.5 kPa; and FIO2 > 0.80 or apnoea.
All values are reported as median with 20th and 80th percentiles. A Wilcoxon signed rank sum test for paired data was used to estimate statistical difference for blood gases and ventilator settings. Differences were considered statistical significant when p < 0.05.
Results
Twenty one patients were treated with nHFV. Table 1 summarises the clinical data. In five (23%) patients, nHFV was discontinued after a median time of 6½ hours (2–8½ hours), and endotracheal mechanical ventilation was started. Table 2 shows blood gas values and ventilator settings before and after initiating nHFV. NHFV was started in 16 infants because of CO2 retention (pCO2 value > 7.5 kPa) and in five infants because of increasing oxygen need (FIO2 > 0.55). A small but significant reduction in pCO2 was found (p = 0.0012; p = 0.0033) after initiation of nHFV compared with the two last blood gases taken before nHFV (figs 1and 2). Pāw pressure was significantly higher after the initiation of nHFV.
Summary of clinical data of 21 infants studied
Values (median with 20th and 80th percentiles) of blood gases and ventilator settings before and after initiation of nHFV

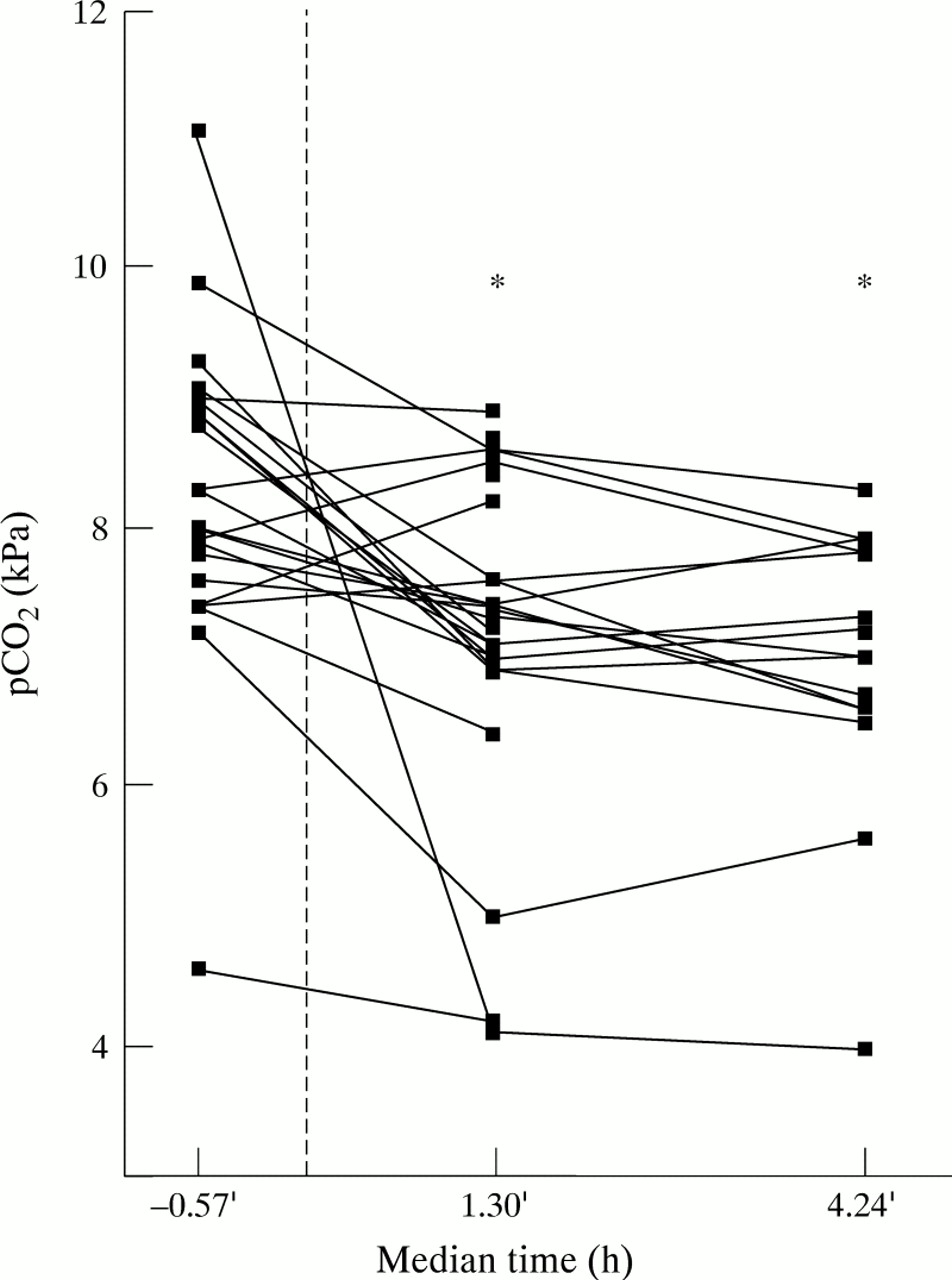
Course of pCO 2 in blood gas before and two blood gases after start of nHFV. PCO 2 decreased significantly in both samples taken at a median time of 1½ hours (0.50–2)hours and at 4.24 (3.2–5.2) hours after the start of nHFV compared with that in the sample taken at 0.57 (1.57–0.34) hours before nHFV was started. p = 0.0012 and 0.0033, respectively.
{kind=link}
{kind=link}
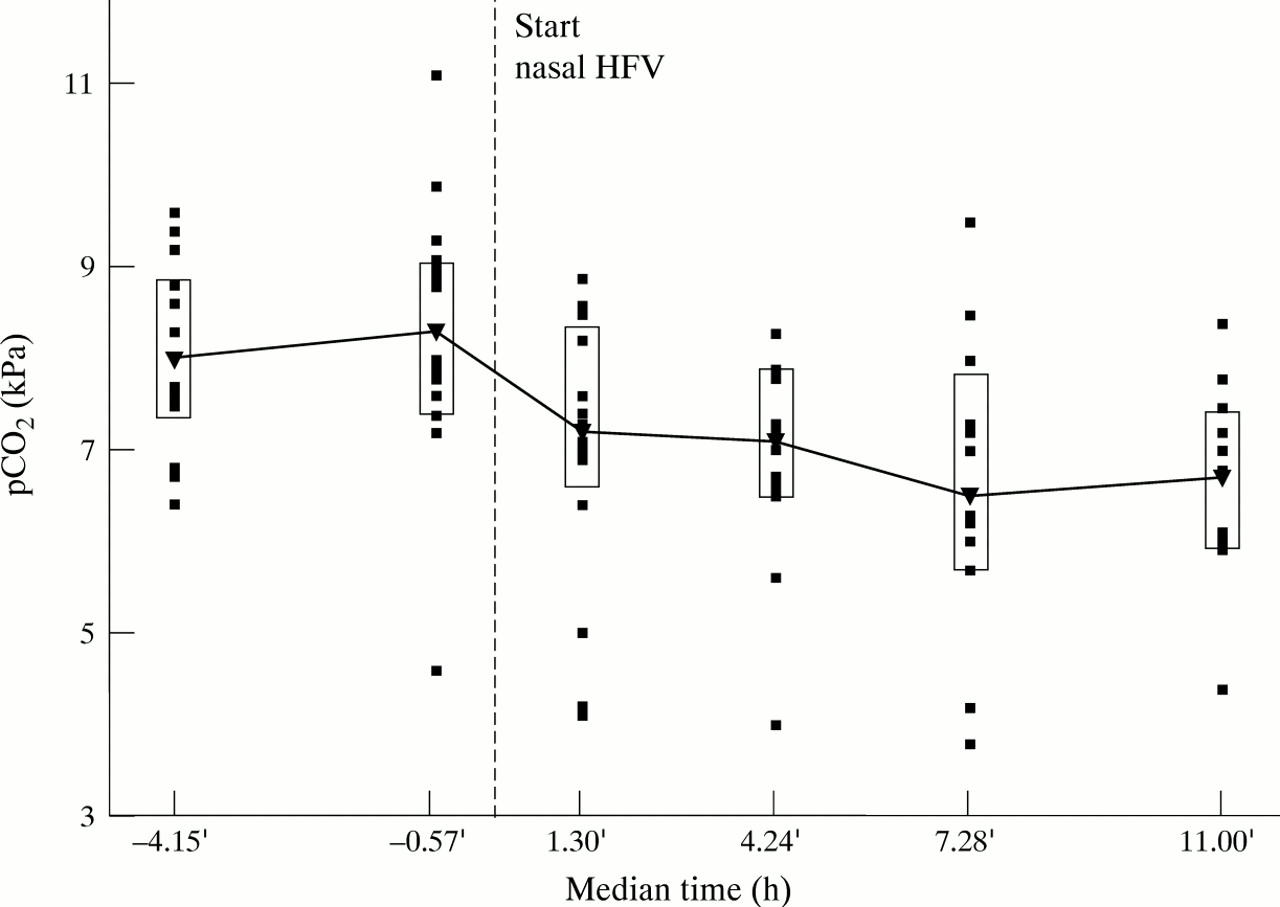
Course of pCO 2 in two blood gases measured before (4.15 and 0.57 hours) and four blood gases measured after (1.3, 4.24, 7.38 and 11 hours) the start of nHFV. Median and 20th and 80th percentiles are shown together.
In 15/21 (72%) patients, nHFV was initiated early in the course of their respiratory disease (median age of 17 hours; 2–36). Respiratory insufficiency was due to idiopathic respiratory distress syndrome (n =10), transient tachypnoea of the newborn (TTN) (n = 3), and hypoventilation (n = 2). NHFV was continued for a median (range) period of 35 (2–144) hours. In three patients with severe idiopathic RDS, nHFV was discontinued and endotracheal mechanical ventilation with surfactant replacement was started within 2 to 6 hours because of further deterioration in blood gases or increased oxygen need.
In 6/21 (28%) patients, nHFV was initiated at a median age 9 days (6–21), after a period of endotracheal mechanical ventilation. The diagnoses included air leak syndrome (n = 2) and apnoea associated with sepsis or necrotising enterocolitis (n = 4). NHFV in this group was continued for a median period of 40 hours (17–126). In two patients in this group with apnoea and sepsis, nHFV was discontinued and endotracheal mechanical ventilation was started because of further deterioration in blood gases and apnoea.
Discussion
This study has shown that nHFV can reduce pCO2 in patients with nasal CPAP with different respiratory problems. Whether nHFV can be recommended as a valuable mode of respiratory support must be determined in a prospective randomised study. We showed that nHFV was effective in reducing pCO2 from 8.3 kPa to 7.2 kPa within 2 hours.
The mechanism of CO2 reduction during HFV is complex and is not completely understood.13 16 As oscillations of the chest are visible during nHFV, direct ventilation of the lung is less important; the larynges are a significant factor in resistance.17 Gas transport during nHFV is probably largely improved by the interaction of convective and diffusive gas flux (also called augmented diffusion) in the pharyngeal and laryngeal area, as has been reported during HFV in the larger and medium airways.16 18
Nasal CPAP has been proposed as a less invasive approach for the management of respiratory distress in very low birthweight infants.4-6 After the introduction of nasal CPAP, a significant decrease in the incidence of intubation was reported.19 Another report showed that the incidence of BPD was decreased in association with the use of early nasal CPAP and permissive hypercapnia.20 However, the use of nasal CPAP seemed to be limited to a small group of infants, as 43 to 80% of the infants with moderate to severe idiopathic RDS went on to require mechanical ventilation due to CO2 retention, increased oxygen need, and apnoea of prematurity.7 The level of CPAP pressure is associated with an increase in paO2, indicating an increased functional residual capacity and/or alveolar recruitment.21-22 But high CPAP pressure was also associated with an increase in paCO2 due to an increase in dead space, alveolar overdistension, and a decrease in alveolar ventilation.21-23 nHFV could be used to control CO2 retention and to permit the use of a higher Pāw pressure so as to reduce oxygen need.
Gaseous distension of the bowel has been mentioned as a disadvantage of the use of nasal CPAP in premature infants. This so-called CPAP belly syndrome has not been associated with necrotising enterocolitis or bowel obstruction and had a benign development.24
In our study some infants who were breathing room air still had clinically significant CO2 retention. In the alveolar air equation alveolar pO2 is determined by the inspiratory oxygen concentration minus the alveolar pCO2, divided by the respiratory exchange ratio. When an alveolar pCO2 is increased to, for example, 10 kPa and the infant is breathing room air and has a respiratory exchange ratio of 0.8, the alveolar pO2 will be 8.5 kPa. Assuming that the gradient between alveolar and arterial pO2 is not severely increased by atelectasis, scatter of ventilation perfusion ratios, or by the presence of a right to left shunt, a clinically significant hypercapnia can exist in association with a low but still normal and acceptable arterial pO2. In addition, as the P90 (the paO2required for 90% oxygen saturation of haemoglobin) in preterm infants was reported to be 5.4 (0.5) kPa,25 there is no clinical or physiological basis to increase the PO2 value when almost all haemoglobin is bound with oxygen.
In a heterogeneous group of infants with moderate respiratory diseases, nHFV was effective in reducing pCO2. nHFV might, therefore, be a valuable addition to the ventilatory management of the newborn infant, and might reduce the need for subsequent mechanical ventilation.