Article Text

Abstract
Objective: To study the effect of different levels of pressure support ventilation (PSV) on respiratory parameters in preterm infants during the weaning phase of mechanical ventilation.
Design/methods: In this quasi-experimental crossover study, a total of 19 154 breaths were analysed from 10 ventilated infants of <32 weeks’ gestation. Breath-to-breath data on minute ventilation, tidal volume, respiratory rate, peak inspiratory pressure and mean airway pressure were collected during three study epochs: synchronised intermittent mandatory ventilation (SIMV) alone, SIMV with partial PSV (PSmin), and SIMV with full PSV (PSmax). PSmin was set to provide an exhaled tidal volume (VTe) between 2.5–4 ml/kg and PSmax 5–8 ml/kg VTe. Statistical analyses were performed using analysis of variance (ANOVA) for repeated measures.
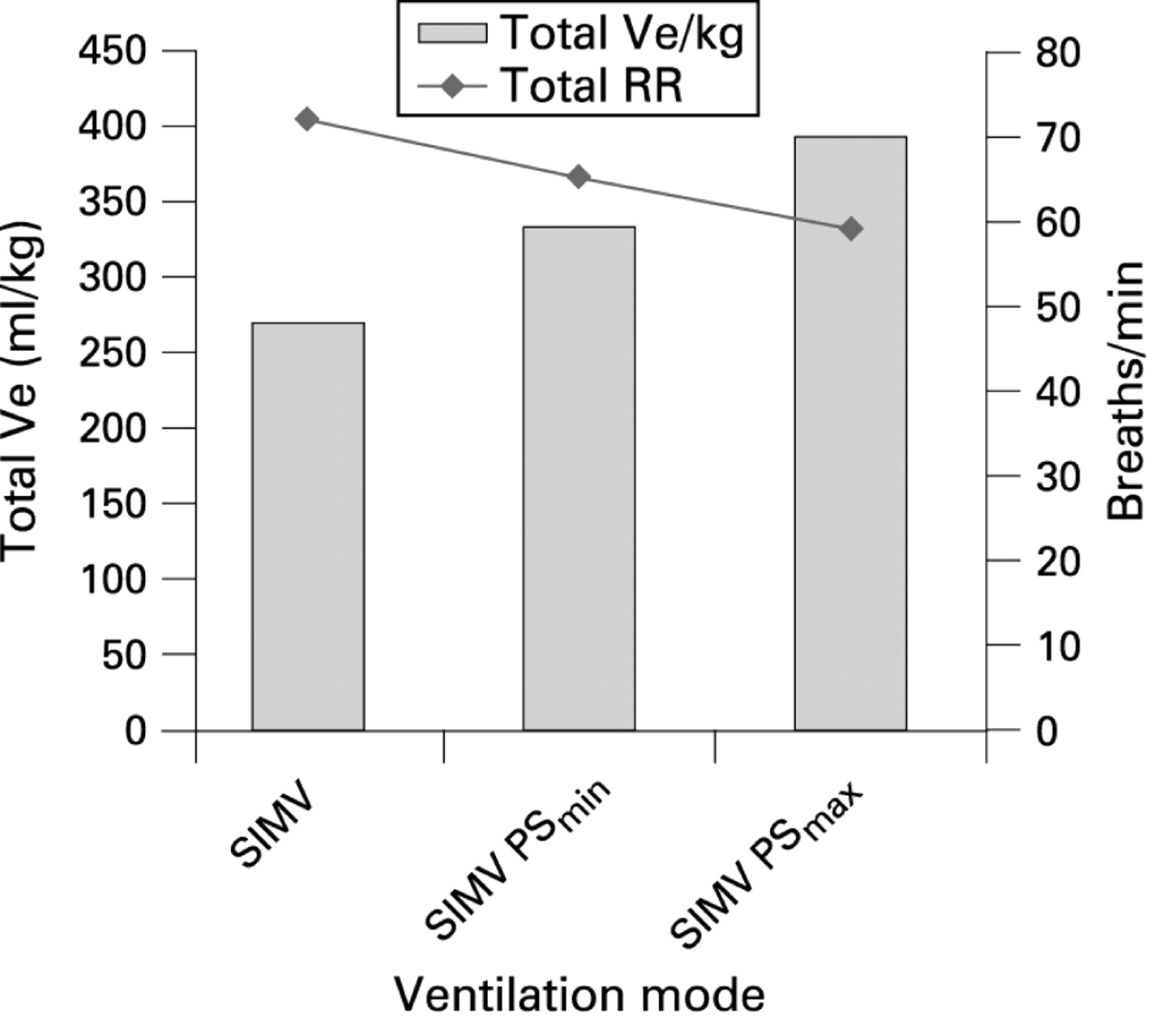
Results: The addition of full PSV (PSmax) was associated with a significant increase in total minute ventilation as compared with SIMV alone (392 ml/kg/min vs 270 ml/kg/min, respectively; p<0.05). This difference in minute ventilation was still present when PSmin was used (332 ml/kg/min as compared with 270 ml/kg/min in SIMV; p<0.05). There was also a concomitant decrease in the respiratory rate with both PSmax (59 breaths per minute) and PSmin (65 breaths per minute) compared with SIMV alone (72 breaths per min) (p<0.05).
Conclusions: Pressure support ventilation increases total minute ventilation and stabilises breathing in proportion to the level of pressure support used. This may be advantageous and provide a useful ventilation strategy for use during weaning stages of mechanical ventilation in preterm infants.
Statistics from Altmetric.com
Pressure support ventilation (PSV) is a ventilatory modality in which patients’ spontaneous breaths are supported by an inspiratory pressure “boost” above the baseline pressure. This is designed to decrease the imposed work of breathing created by the narrow lumen endotracheal tube and ventilator circuit, and to facilitate weaning. It is a form of patient-triggered ventilation, which can be used either alone in patients with reliable respiratory drive or in conjunction with other modes of ventilation in patients who have poor or unreliable respiratory drive. When used in conjunction with synchronised intermittent mandatory ventilation (SIMV) either in pressure- or volume-targeted modalities, PSV augments the tidal volume generated by a patient's own spontaneous breathing.
What is already known on this topic
Pressure support ventilation (PSV) supports spontaneous breaths by providing pressure boost and thus should decrease the work of breathing.
Patients have control on how much to breath and for how long to breathe.
PSV has been described in adult and paediatric intensive care but the data regarding its use in the neonatal population are limited.
What this study adds
Pressure support ventilation increases total minute ventilation and stabilises the breathing pattern in preterm infants.
The increase in respiratory efficiency is proportional to the level of pressure support-provided ventilation.
The three distinct characteristics of PSV are: (1) triggering; (2) pressurisation; and (3) cycling, which are accomplished using changes in airway flow (fig 1).1 There are important differences between PSV and traditional time-cycled, pressure-limited (TCPL) ventilation. In TCPL, circuit gas flow is fixed and the inspiratory time is set by the clinician, whereas in PSV, inspiratory gas flow is variable and is proportional to patient demand. The inspiratory phase in PSV is flow-cycled, and inspiration ends when flow has decelerated to a small percentage of peak. Because of the ability to control inspiratory time and rate, synchronisation occurs during both the inspiratory and expiratory phases. Thus, patients have control of how much to breathe (inspiratory flow and tidal volume) and for how long to breathe (inspiratory time), thus mimicking physiological breathing.2

PSV has been shown to reduce the work of breathing and oxygen requirement in intubated adult and paediatric patients.3 4 There is no consensus as to what the most appropriate level of PSV is in neonatal patients. A recent study by Osorio et al5 reported the effect of two levels of pressure support as an adjunct to SIMV in ventilated premature infants. They chose arbitrary levels of pressure support (3 and 6 cm H2O) and weaned babies by decreasing the SIMV rate. As tidal volume delivery was not targeted in this study, the interpretation about the effectiveness of pressure support becomes difficult, especially at the lower level, which might not have been sufficient to generate effective tidal volume delivery. In another published study, Migliori et al6 targeted the exhaled tidal volume (VTe) delivery only at 6 ml/kg and did not study the effect of different levels of PSV.
In the present study, we assessed the effects of two different levels of pressure support: full pressure support or partial pressure support (PSmax and PSmin, respectively) on respiratory parameters, and compared their effectiveness in relation to SIMV during weaning from mechanical ventilation in preterm infants.
PATIENTS AND METHODS
This was a quasi-experimental study design, crossover trial, carried on the Neonatal Unit at James Cook University Hospital, Middlesbrough, UK. The study was part of an ongoing, randomised, controlled trial, which was approved by the Institutional Review Board, and written informed consent was obtained from each parent prior to study entry. Babies <32 weeks’ gestation and receiving assisted ventilation for respiratory distress syndrome (RDS) were eligible for enrolment during the recovery phase. To meet entry criteria, the mean airway pressure (mean Paw) had to be <10 cm H2O, and fraction of inspired oxygen (FiO2) <0.4. All infants received caffeine citrate (20 mg/kg loading, 5 mg/kg/day maintenance dose) at entry into the study, and demonstrated reliable respiratory drive, defined as a spontaneous respiratory rate at least 25% higher than the ventilator rate.6 Newborns with systemic or thoracic malformations, neuromuscular diseases, or thoracic air leaks were not eligible for inclusion.
According to a standardised unit protocol, all babies were ventilated with the Avea® ventilator (Viasys Healthcare, Yorba Linda, California, USA) using either TCPL or volume-controlled (VC) ventilation. At entry into the trial, they were on low-rate SIMV (20 breaths/min), combined with PSV. The peak inspiratory pressure for SIMV breaths was set between 12 and 16 cm H2O to provide a VTe of 5–8 ml/kg.
Both the mechanical and spontaneous respiratory parameters were displayed on the digital interface graphic monitor. The Medical Information Bus (MIB) interface from the monitor was used to download continuous breath-to-breath data to a secure computer using a proprietary “GSP Interface Kit” and research tool software (Viasys Healthcare, Yorba Linda, California, USA). These data were then exported to a spreadsheet (Microsoft Excel, Microsoft Corp., Redmond, Washington) for further analyses.
Babies were randomly assigned to one of the three study modes for 30-minute epochs — SIMV, SIMV with partial PSV (PSmin) or SIMV with full PSV (PSmax), and then switched to another study mode in a random order. PSmax was targeted to deliver a VTe of 5–8 ml/kg to match the SIMV breaths, and PSmin was adjusted to deliver 2.5–4 ml/kg VTe. The mandatory machine breaths in all three study modes were kept at 20 breaths per minute. The spontaneous breaths in babies receiving SIMV alone were supported only with PEEP. When pressure support was added the same spontaneous breaths were either half or fully supported to become partial PSV or full PSV, respectively. This allowed us to compare the effect of different levels of pressure support by augmenting the spontaneous breaths and comparing across the study groups.
Real-time breath-to-breath pulmonary mechanics data were collected during each study epoch. This included inspired tidal volume (VTi) and VTe, spontaneous and total minute ventilation (Ve), total respiratory rate (spontaneous plus mechanical breaths, RR), FiO2, and peak inspiratory pressure (PIP). A re-equilibration period of 15 minutes was used between the epochs. In order to avoid spill-over from the previous mode, 10 minutes of artefact-free data were extracted from the latter half of each epoch, and subsequently integrated for analysis. The demographic data for gender, gestational age, postnatal age, and weight at birth and at study entry were recorded for each subject. During the recording of data, handling of babies was not permitted; however, FiO2 was adjusted to maintain the pulse oximeter reading in a target range of 88%–92%. The rapid shallow breathing index (RSBI) was used as a measure of the efficiency of breathing. This was calculated by taking the ratio of respiratory rate to tidal volume (RR/VTe) and expressed as breaths/min/ml/kg and compared across the epochs. Using the RSBI, the lower the ratio, the better is the efficiency of spontaneous breathing.
The mean value for each outcome measure was calculated on each ventilation mode for every baby and then compared between the study epochs. This was then utilised for the statistical analyses and compared between the groups. Statistical analyses were performed using analysis of variance (ANOVA) for repeated measures and the post hoc Bonferroni test, to evaluate differences in respiratory parameters between the three study groups. Outcome comparisons between the groups were also carried out using the two-sided t test for parametric data and the Mann–Whitney U test for non-parametric data. All statistical analyses were performed using SPSS Inc., version 12 for Windows™ (Chicago, Illinois, USA).
RESULTS
Ten ventilated babies were enrolled in the study. Their mean gestational age and birth weight were 28 weeks and 1190 g, respectively. The mean age at entry into the study was 16 days. All babies successfully completed the study and provided a total of 19 154 breaths for analyses. There were equal numbers of babies receiving TCPL and VC ventilation.
The ventilator parameters were adjusted to achieve the desired VTe and the data for partial pressure of CO2 (pCO2) were collected before and after the cross-over study period on all infants. There were no differences in the pCO2 levels and clinical status before or after the study period. There were no major episodes of desaturation during the study period.
There was a significant increase in minute ventilation during PSmin compared with SIMV alone. This was associated with a concomitant decrease in the total respiratory rate (table 1). These differences in minute ventilation and total respiratory rate were even more marked when full pressure support was applied (fig 2). There was also a statistically significant difference in the observed parameters when PSmax was compared with PSmin (total minute ventilation 392 ml/kg/min in PSmax vs 332 ml/kg/min in PSmin; p<0.05; and total respiratory rate 59 breaths per min in PSmax vs 65 breaths per min in PSmin; p<0.05). There was also a significant decrease in the mean (SD) RSBI during PSmin (17.4 (0.31) breaths/min/ml/kg) and PSmax (10.2 (0.24) breaths/min/ml/kg) compared with SIMV alone (42.9 (1.00) breaths/min/ml/kg). Both of these differences were statistically significant (p<0.05).

{kind=link}
{kind=link}
There was also an incremental effect on mean Paw, PIP and FiO2 according to the level of pressure support. The mean Paw increased significantly with the addition of PSV compared with SIMV alone. The increase in mean Paw and PIP was greater with full PSV compared with partial PSV. The FiO2 decreased significantly and proportionally with the addition of PSV (table 2).
DISCUSSION
Pressure support ventilation is a ventilatory mode in which spontaneous breaths are partially or fully supported by an inspiratory pressure assist above the baseline pressure. During weaning of mechanical ventilation, spontaneous breathing must overcome the work imposed by the presence of a high-resistance endotracheal tube, ventilatory circuit and the disease-induced respiratory load. Pressure support can be used as an adjunct to SIMV to partially or fully unload the spontaneous breaths.5 PSV increases the tidal volume proportionally to the chosen pressure support level, achieves synchrony during both inspiration and expiration, and enhances the efficiency of breathing.7 PSV has been shown to reduce the work of breathing and oxygen requirement in intubated adult and paediatric patients3 4 and appears to accelerate weaning from mechanical ventilation and to reduce ventilatory dependency.8 9 PSV with SIMV has been compared with SIMV alone in a randomised controlled trial and was reported to have advantages as compared with SIMV alone for weaning. This study, however, only used pressure support of 30%–50%.10 PSV has been reported to be beneficial but there are not yet sufficient data to compare its effectiveness at different levels. This is important to know, as PSV can be used for both full and partial support and may offer advantages over other modalities of ventilation, especially during weaning, as it resembles physiological breaths.
In the present study, each baby served as his/her own control. The mandatory SIMV rate was kept constant at 20 breaths per minute throughout the study period to enable assessment of the effects of two levels of pressure support, which were aimed to maintain a desired range of VTe. This enabled us to standardise the level of PS across the study epochs.
Data from this study suggest that the use of PSV increases total minute ventilation and stabilises the breathing pattern, while enabling the baby to decrease the total respiratory rate. The significantly lower RSBI observed in this study when PSmax was used (compared with PSmin), suggests that there is an incremental increase in respiratory efficiency by providing more pressure support, perhaps by augmenting the unloading of respiratory muscles. This has not been reported before in newborns but mirrors the observations made in paediatric and adult patients.11 There are limited data comparing various levels of PSV,12–14 but these studies suggest that the addition of PSV during weaning augments spontaneous breathing with better thoraco-abdominal synchrony, increase in minute ventilation, and reduction in the total respiratory rate compared with SIMV alone.15
Addition of PSV in the present study increased mean Paw and PIP. This has been observed before.6 While this may be a source of anxiety, it should be realised that PSV is flow-cycled, and inspiratory gas flow delivery is variable according to the patient effort. This, in fact, makes PSV more physiological than the mechanically delivered mandatory breaths, which are set by the operator and are thus more prone to result in patient–ventilator asynchrony. The effect of PSV in improving minute ventilation with a better RSBI through reduction in the spontaneous respiratory rate may be explained by the optimisation of tidal volume delivery and patient–ventilator synchrony.
The decrease in FiO2 observed with the addition of PSV may have resulted from better alveolar recruitment. Another possibility is the opportunity for the infant to sigh during PSV through voluntary extension of the inspiratory time, which could also contribute to improved oxygenation. This observation of a decrease in the oxygen requirement with increasing pressure support is important while weaning preterm babies who require prolonged ventilatory support.
Because of lack of availability of continuous blood gases monitoring devices, we were limited in our ability to collect continuous data on pCO2. Nonetheless, our data suggest that the infants probably adjust spontaneous breathing, and thus minute ventilation, as a way to maintain normocapnia, and that higher PSV levels provide a higher tidal volume, requiring fewer spontaneous breaths. The previous study by Osorio also did not show any changes in pCO2.5
In summary, the findings of this study confirm that PSV enhances the efficiency of spontaneous breathing during weaning of preterm infants from mechanical ventilation. The increase is proportional to the level of pressure support used. Based on our findings, different levels of pressure support can be used to facilitate a gradual shift of work of breathing from the ventilator to the baby, and conditioning the respiratory muscles for successful extubation. Further clinical trials are needed to fully explore the safety and efficacy of different levels of pressure support in newborn infants requiring mechanical ventilation.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Written informed consent was obtained from each parent prior to study entry.