Article Text

Abstract
AIM To determine if infants who had become dependent on inhaled nitric oxide treatment could be successfully weaned off it if FIO2 was increased briefly during withdrawal.
METHODS Sixteen infants admitted for conditions associated with increased pulmonary vascular resistance responded well to inhaled nitric oxide treatment with a significant increase in PaO2 (maximum inhaled nitric oxide given 25 ppm). Weaning from inhaled nitric oxide in 5 ppm decrements was initiated once the FIO2 requirement was less than 0.5. When patients were stable on 5 ppm of inhaled nitric oxide, the gas was then discontinued. If a patient showed inhaled nitric oxide dependence—that is, oxygen saturation fell by more than 10% or below 85%—inhaled nitric oxide was reinstated at 5 ppm and the patient allowed to stabilise for 30 minutes. At this time, FIO2 was increased by 0.40 and weaning from inhaled nitric oxide was attempted again.
RESULTS Nine infants were successfully weaned on the first attempt. The seven infants who failed the initial trial were all successfully weaned following the increase in FIO2. After successful weaning, FIO2 was returned to the pre-weaning level in mean 148(SD 51) minutes and inhaled nitric oxide was never reinstated.
CONCLUSION Infants showing inhaled nitric oxide dependency can be successfully weaned by increasing FIO2 transiently.
- inhaled nitric oxide
- weaning
- ECMO.
Statistics from Altmetric.com
A significant number of infants who respond favourably to inhaled nitric oxide treatment prove difficult to wean off it. This dependence necessitates prolonged use of inhaled nitric oxide or, on occasion, the use of alternative treatments, such as extracorporeal membrane oxygenation (ECMO).
Nitric oxide (NO), or endothelium derived relaxing factor, is an endogenously produced substance which helps regulate vascular smooth muscle tone in the circulation of many organs, including the perinatal lung.1-7 Therapeutic inhalation of NO in various pulmonary diseases is currently under evaluation in several neonatal intensive care units. On the basis of preliminary reports, there is little doubt that inhaled nitric oxide is effective in raising systemic arterial oxygen concentration in several clinical situations where pulmonary vascular resistance is raised.6-9 This change in oxygenation is presumed to result from a reduction in pulmonary vascular resistance and diminution in right to left shunting. The clinical subtleties of the use of inhaled nitric oxide are as yet undefined.10-16 In particular, many observers have reported difficulty in discontinuing treatment with inhaled nitric oxide, in both clinical and experimental settings.9 17-20 We recently observed that seven of 16 infants who failed initial attempts at discontinuation of inhaled nitric oxide treatment were successfully and quickly weaned when the inhaled FIO2 was increased briefly during the withdrawal of inhaled nitric oxide.
Methods
All newborn infants admitted to the neonatal intensive care unit between December 1994 and July 1995 with severe hypoxaemia and clinical and echocardiographic evidence of pulmonary hypertension were considered for this study. Infants whose hypoxaemia proved refractory to optimal ventilatory and cardiotonic support were offered treatment with inhaled nitric oxide; all parents opted for this treatment. The study was approved by the Institutional Review Board and parental informed consent was obtained for all patients.
Twelve of these 16 infants had been hyperventilated at the referring hospital and met otherwise generally accepted criteria for extracorporeal membrane oxygenation (ECMO) treatment.21The clinical characteristics of the study population are shown in table1.
Characteristics of study population
Nitric oxide was introduced into the afferent limb of the ventilator circuit via an adapter placed 18 inches upstream from the endotracheal tube. Nitric oxide treatment was initiated at a dose of 25 ppm. Continuous measurements were made of heart rate, systemic blood pressure, and pre-and post-ductal pulse oximetry before and after initiation of inhaled nitric oxide treatment. Frequent serial measurements of arterial pH, arterial carbon dioxide activity, and arterial oxygen activity were recorded as well. Data were collected and logged continuously using the VT 1000 Neonatal Workstation (Vitaltrends Technology, Inc, Hackensack, NJ).
If an infant responded to inhaled nitric oxide with a significant increase in arterial saturation to above 85%, the treatment was continued at the same dose. If an infant failed to respond to inhaled nitric oxide, management with ECMO was started and the medication discontinued.
As the oxygenation improved, FIO2, ventilatory pressure and rate were decreased while the concentration of inhaled nitric oxide remained at therapeutic levels—greater than 5 ppm. Once the pre- and post-ductal oxygen saturation gradient was insignificant on modest FIO2 (usually 0.40-0.45) and mean airway pressure was less than 10 cm H2O, weaning of inhaled nitric oxide started. Weaning was attempted in 5 ppm decrements every 4 hours, as tolerated by the infant. The FIO2 was kept constant during the weaning phase. Heart rate, systemic blood pressure, and oxygen saturations were carefully monitored and arterial blood gases were obtained every 4 hours. If the infant tolerated weaning by 5 ppm for 4 hours, further weaning in 5 ppm decrements continued until a concentration of 5 ppm of inhaled nitric oxide was reached. Once the infant was stable on 5 ppm, inhaled nitric oxide treatment was discontinued. Heart rate, systemic blood pressure, and oxygen saturations continued to be closely monitored. If the saturation dropped by 10% or below 85% it was considered a weaning failure and inhaled nitric oxide was reinstated at 5 ppm. A second attempt at weaning from inhaled nitric oxide was made 30 minutes later when the infant’s heart rate, blood pressure, and saturation were stable. However, before the second attempt, the FIO2 was increased by 0.4. If the infant remained stable during this attempt at weaning, the FIO2 was then decreased over the next few hours, as tolerated.
DATA ANALYSIS
Mean values for all variables for each infant were computed every 60 seconds and stored on the hard disc of the VT 1000. The data were subsequently analysed using commercial statistical software (Systat, Inc, Evanston, IL, USA). Depending on the response to weaning, infants were classified into two groups: group I infants were successfully weaned from inhaled nitric oxide without the need for additional oxygen; and group II infants did not tolerate weaning (as evidenced by decreasing oxygen saturation by 10% or less than 85%) and required reinstitution of inhaled nitric oxide. Group II infants subsequently underwent weaning while receiving higher concentrations of oxygen. Table 2 shows that there were no differences in birthweight, gestational age, duration of inhaled nitric oxide treatment, PaO2 at time of introduction of inhaled nitric oxide, or PaO2 at initial inhaled nitric oxide weaning between group I and II infants.
Clinical characteristics of group I infants compared with those of group II infants (mean (SD))
For purposes of analysis, the experimental protocol was divided into five phases: phase 1, baseline period; phase 2, weaning without incremental FIO2; phase 3, restabilisation; phase 4, weaning from inhaled nitric oxide with supplemental oxygen; and phase 5, weaned from inhaled nitric oxide and back to the pre-weaning concentration of oxygen. The averages of all minute means of heart rate, blood pressure, and oxygen saturation for each phase of the study were computed. In addition to measurements of mean heart rate, mean blood pressure, and mean oxygen saturation during phases 1, 3, and 5, the maximum and minimum measurements during phases 2 and 4 (times of weaning) were also determined. Statistical comparisons between various phases within and between the two groups were made using pairedt tests. Differences were considered significant at P <0.05.
Results
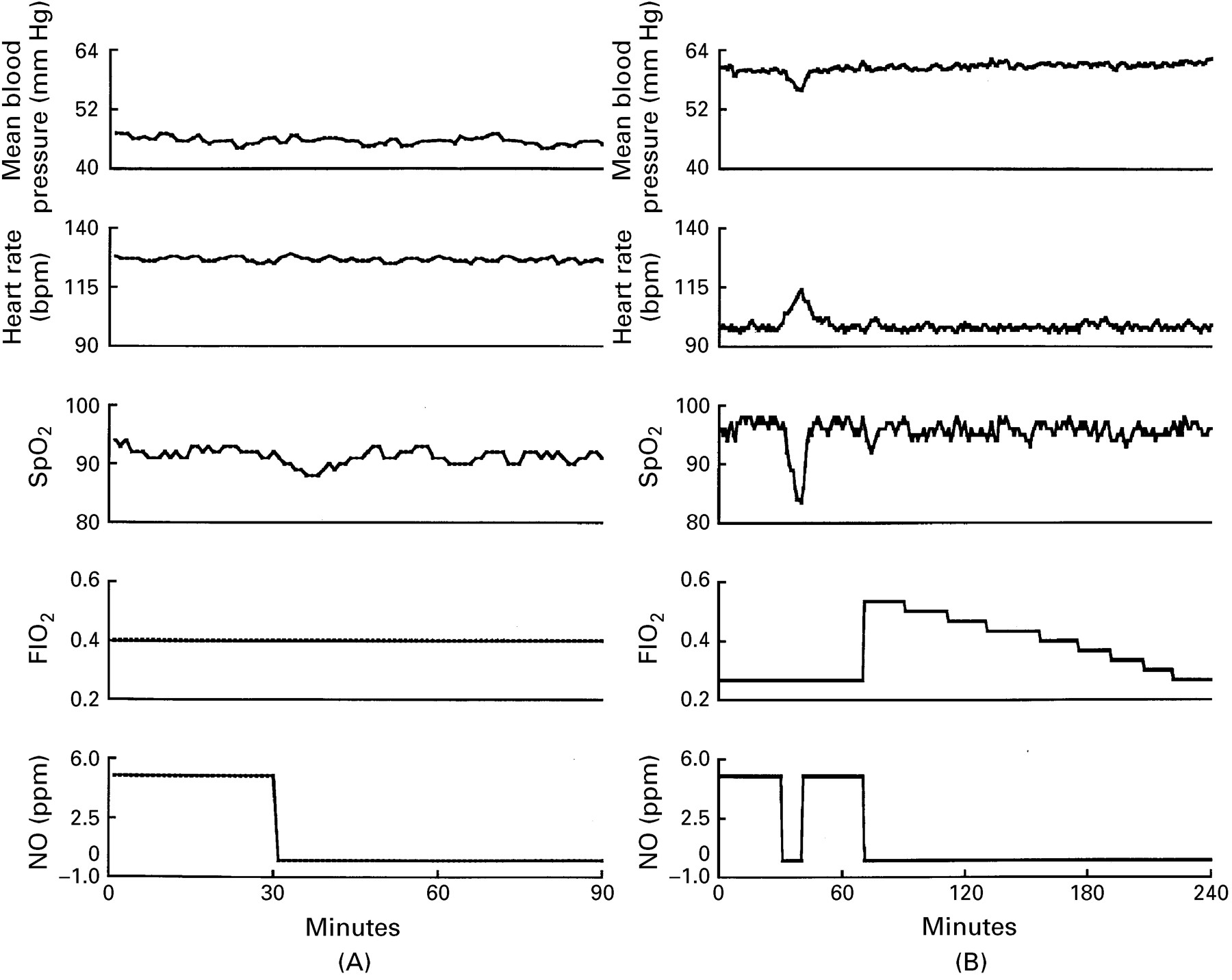
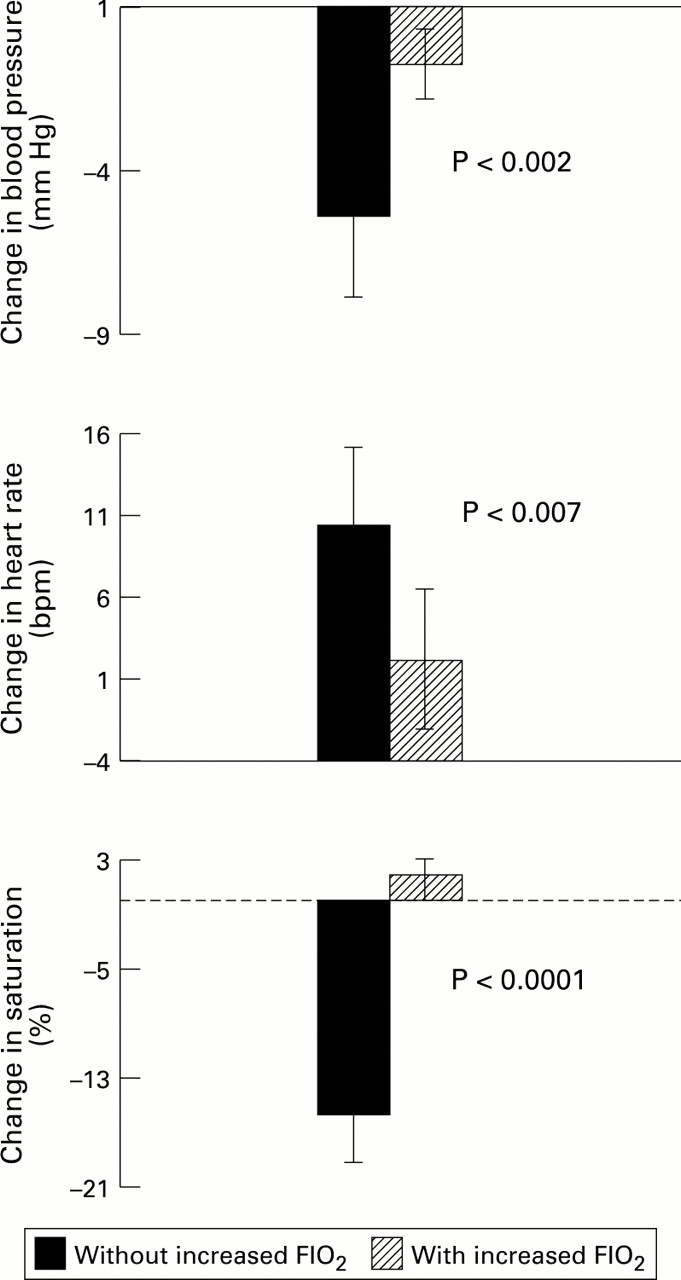
Nine of the 16 patients were weaned successfully from inhaled nitric oxide without an increase in oxygen concentration. The other seven infants required reinstitution of inhaled nitric oxide because of unfavourable changes in oxygen saturation. The data from two infants, one from group I and another from group II, are shown in fig 1. These plots show the differences in physiological measurements during initial successful and unsuccessful weaning. All seven infants who failed initial weaning attempts were successfully weaned from inhaled nitric oxide when the FIO2 was increased. Comparison of the means and standard deviations of the changes in blood pressure, heart rate, and oxygen saturation during weaning attempts in group II with and without increasing FIO2, are shown in fig 2. In group II (n=7) the differences in all variables during the initial weaning attempt without oxygen and the second attempt with additional oxygen were highly significant. As evidence of successful weaning, measurements of the same variables at the onset of weaning (phase 1), and when the concentration of inhaled oxygen was returned to preweaning levels (phase 5), were not significantly different (n=16). The duration required for inhaled oxygen to be returned to its preweaning level in group II infants (mean (SD)) was 148 (51) minutes.
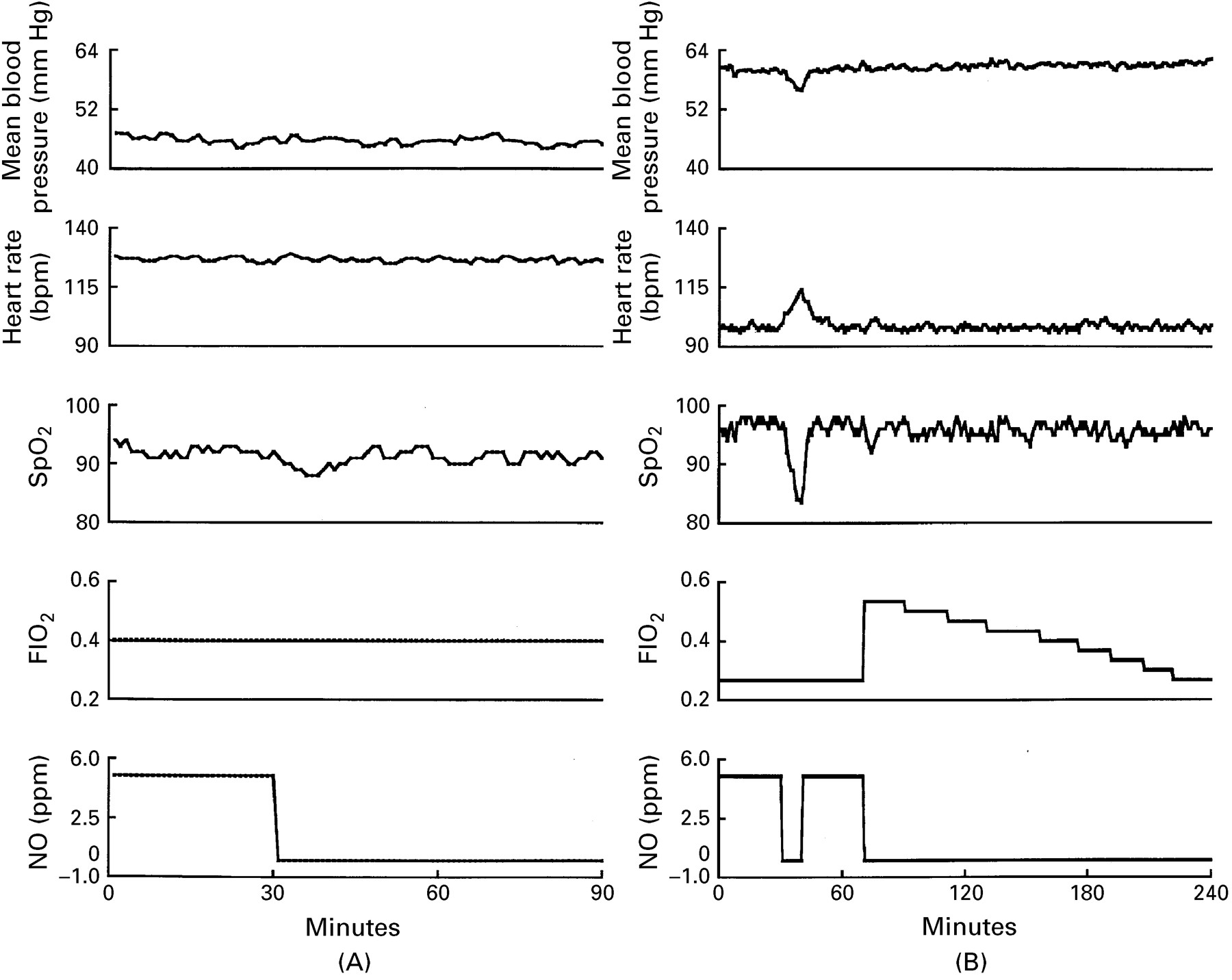
In panel (A) measurements of mean blood pressure, heart rate, arterial oxygen saturation (SPO2), FIO2 and NO concentrations obtained from an infant in group I are plotted against time in minutes. Note stability of measurements as INO is withdrawn. In panel (B) the same measurements are plotted for an infant in group II. Acute deterioration in all variables followed the initial attempt at weaning. FIO2 was increased and the weaning was successful. Note, in particular, how quickly FIO2 was reduced following successful weaning.

{kind=link}
{kind=link}
Changes in mean blood pressure, heart rate, and arterial oxygen saturation following weaning without oxygen (trial I) and with oxygen (trial II) for the seven infants who failed trial I.
Discussion
Endogenously produced NO is now recognised as an important modulator of fetal and neonatal pulmonary vascular tone.1-7 It is produced by the normal human lung22 and can be found in exhaled gas.24Inhaled NO diffuses from the alveolar space through the alveolar wall and reaches the vascular smooth muscles of the small pulmonary arteries, where, in combination with endogenous NO, it enhances vasodilatation. Some NO traverses the endothelial cell and enters the vessel lumen, where it is rapidly inactivated by haemoglobin and, therefore, does not reach the systemic circulation.8 19 25 Therapeutic inhalation of NO (20 to 80 ppm) to supplement endogenous NO production seems to be an effective treatment for increased pulmonary vascular resistance due to a variety of underlying pathologies.
Early reports illustrate that there may be difficulty in weaning inhaled nitric oxide due to a “rebound” phenomenon—that is, a sudden deterioration in oxygenation after withdrawal of inhaled nitric oxide treatment. This rebound has been observed in both clinical and experimental settings.9 17-21 Heretofore, it has often been necessary to reinstate the inhaled nitric oxide treatment before subsequently repeating the weaning process. Occasionally, weaning has been delayed for as long as three weeks because of rebound hypoxaemia.17 The results of this study indicate that infants can be successfully weaned from inhaled nitric oxide by simply increasing the inhaled concentration of oxygen while inhaled nitric oxide is being withdrawn. In fact, early weaning from inhaled nitric oxide during the recovery phase of persistent pulmonary hypertension of the newborn was possible in all 16 infants described above. Despite major signs of deterioration during the initial attempt, all seven of the infants who failed the first attempt at weaning were subsequently weaned quickly with increased supplemental oxygen.
This study does not allow us to rule out the possibility that the second attempt at weaning was successful because of spontaneous improvement in the patients’ underlying disease. However, the fact that weaning was successful within hours of the original weaning failure makes this explanation unlikely. Meanwhile, testing of this hypothesis by randomly assigning infants who fail initial attempts at weaning to treatment with and without incremental oxygen is recommended.
There are several possible explanations for this effect of supplemental oxygen. Nitric oxide and NO donor agents are known to inhibit endothelium dependent relaxation of arterial rings and endogenous NO generation from intact endothelial cells, without diminishing the sensitivity of the vascular smooth muscle cells to the relaxing effect of exogenous NO.26 This observation suggests that inhaled nitric oxide inhibits the endothelial NO synthase enzyme by a direct feedback mechanism. A simple feedback mechanism could explain the acute clinical deterioration of infants on withdrawal of inhaled nitric oxide treatment as endogenous NO might not be produced at a sufficient rate to replace the exogenous supply.
The fact that oxygen was able to prevent weaning failures could have been due to a direct vasodilatory effect of increased arterial oxygen activity in the alveolus and/or pulmonary circulation, at a time when synthesis of NO was recovering from earlier suppression. On the other hand, the effect of additional oxygen may be explained by enhanced NO production due to improved oxygenation. Dollberg et al 27 demonstrated that increasing oxygenation after initiation of ECMO does seem to be associated with increased NO synthesis, as evidenced by increased urinary nitrate and nitrate concentration in patients with persistent pulmonary hypertension of the newborn following institution of ECMO. Furthermore, it is well established that NO mediates pulmonary vascular tone via guanosine-3’,5’-cyclic monophosphate (cGMP).28-30 In vivo animal studies have shown that inhibitors of cGMP-specific phosphodiesterase potentiate and substantially prolong the duration of the pulmonary vasodilating action of NO.29 Animals pre-treated with one of these agents, Zaprinast, did not show the acute withdrawal reaction on discontinuation of inhaled nitric oxide treatment.31 This prevention of the rebound response, similar to what we observed with increased FIO2, suggests that inhibition of cGMP-specific phosphodiesterase by oxygen may be another mechanism to account for the beneficial effects of oxygen during inhaled nitric oxide withdrawal. Finally, oxygen may be helpful in clearing N-nitro L-arginine, a competitive inhibitor of NO that increases pulmonary artery pressure and is cleared in the blood by oxidation.32 These data suggest that a second attempt at weaning infants from inhaled nitric oxide should be made with increased supplemental oxygen, whenever the overall clinical condition of the infant indicates weaning is appropriate.
Acknowledgments
This work was supported by United States Public Health Service Grants RR00645 and HD13063.
References
Linked Articles
- Original article