Article Text

Abstract
Objective: To compare the incidence of nasal trauma associated with the use of prong or mask during nasal continuous positive airway pressure (nCPAP) support in very low birthweight (<1501 g) infants.
Design: Randomised controlled clinical trial.
Setting: Tertiary care university hospital, Department of Paediatrics, Kuala Lumpur, Malaysia.
Methods: All very low birthweight infants admitted to the neonatal intensive care unit between July 2001 and December 2003 who received nCPAP through the Infant Flow Driver were randomised to the use of either nasal prong or mask. The nasal cavity of these infants was inspected daily during the first week and then weekly until they were weaned off nCPAP.
Results: Of the 89 infants recruited, 41 were randomised to the mask group and 48 to the prong group. There was no significant difference in the incidence of nasal trauma between the two groups (p = 0.5). The primary site of trauma was at the junction between the nasal septum and the philtrum in infants in the mask group and the walls of the nasal septum in the prong group. Logistic regression analysis showed that duration of nCPAP was the only significant risk factor associated with development of nasal injury, after birth weight, gestational age, and nasal device used had been controlled for (adjusted odds ratio 1.04; 95% confidence interval 1.01 to 1.07; p = 0.003).
Conclusion: Irrespective of the type of nasal device used, nasal trauma is common during nCPAP treatment, which should therefore be terminated as soon as possible.
- IFD, Infant Flow Driver
- nCPAP, nasal continuous positive airway pressure
- VLBW, very low birth weight
- continuous positive airway pressure
- mask
- nasal prong
- trauma
- very low birthweight infants
Statistics from Altmetric.com
Nasal continuous positive airway pressure (nCPAP) is a common mode of respiratory support used in many neonatal intensive care units for preterm infants. Several studies including a Cochrane Database of Systematic Reviews reported a reduction in the incidence of failed extubation in infants given elective nCPAP after extubation.1–3 A variety of methods of delivery are available. The Infant Flow Driver System (IFD; Electro Medical Equipment Ltd, Brighton, Sussex, UK) is commonly used world wide. The system consists of a generator, a driver, and fixation accessories. nCPAP by the IFD is provided by application of a set of soft silicon nasal prong to the nose or a nasal mask covering the nose with appropriate strapping and fixation. Although nasal trauma associated with the use of nasal prong with the IFD has been reported by Robertson et al,4 there are no studies in the literature in which the incidence of nasal trauma caused by nasal prong is compared with that caused by nasal mask. Neither are there any studies confirming the efficacy of nasal mask CPAP in neonates. The present study aimed to compare the incidence of nasal trauma caused by nasal mask with that caused by nasal prong during nCPAP treatment using the IFD.
PATIENTS AND METHODS
This was a randomised controlled study. All subjects were recruited prospectively on admission to the neonatal intensive care unit of the hospital of the Universiti Kebangsaan, Kuala Lumpur, Malaysia between 1 July 2001 and 31 December 2003. The study protocol was approved by the hospital’s research scientific and ethics committee.
The inclusion criteria were very low birth weight (VLBW, <1501 g) infants with respiratory distress who received nCPAP via the IFD on admission or were weaned off the ventilator and received nCPAP for continuing respiratory support. Exclusion criteria were CPAP by other methods—for example, bubble bottle or ventilator CPAP—and tracheo-oesophageal fistula, diaphragmatic hernia, pneumothorax, nasal deformities, bilateral choanal atresia, or other major malformations.
On admission to the neonatal intensive care unit, an eligible infant was assessed by a medical officer for the presence of respiratory distress based on the Silverman-Andersen retraction score.5 Briefly, this score is derived from the presence of five clinical signs (grunting, nasal flaring, sternal retraction, intercostal recession, and see-sawing movement of the abdomen and sternum) each with a maximum score of 2 and a minimum score of 0 and a total score of 10. The higher the total score, the more severe the respiratory distress. During the study, any infant with a Silverman-Andersen retraction score of 1–5 was given nCPAP after exclusion of choanal atresia, tracheo-oesophageal fistula, diaphragmatic hernia, and pneumothorax. Those with a Silverman-Andersen retraction score >5 were ventilated. Parents were then approached for informed consent for their infant to be enrolled in the study. The written consent form was available in three languages (Malay, English, and Chinese) for the three major ethnic groups in Malaysia. The parents of infants who initially received mechanical ventilation and were subsequently ready for extubation to nCPAP treatment were approached for consent for enrolment in the study before extubation. Oral intubation is used in our unit, and none of the infants enrolled in this study had nasal intubation.
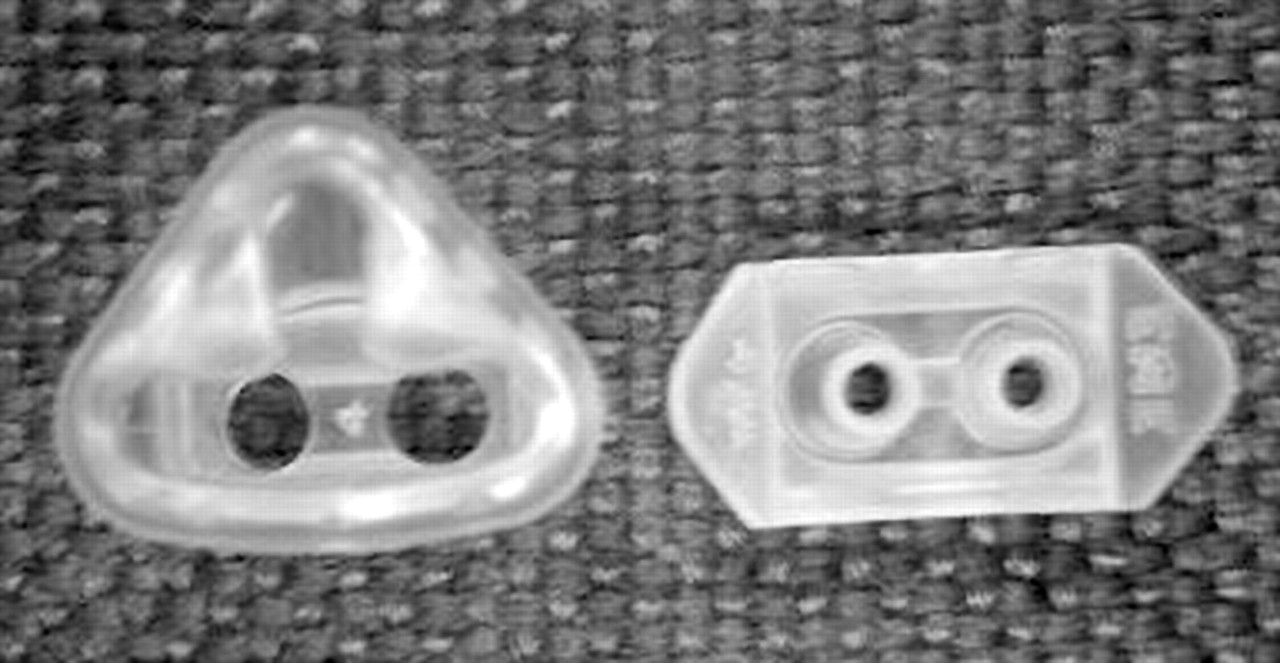
Eligible infants were stratified into those treated with nCPAP on admission and those receiving nCPAP after ventilation. They were randomised to receive nCPAP using either nasal prong or nasal mask (fig 1) based on group assignment contained in sequentially numbered sealed opaque envelopes, which had been prepared beforehand, shuffled randomly, and then numbered serially.
{kind=link}
Silicon nasal mask (left) and nasal prong (right).
After randomisation, the IFD was set up according to the manufacturer’s instructions. The medical officer in charge of the recruited infant inspected the infant’s nose using an overhead angle poise light before the start of nCPAP. Thereafter all infants were inspected daily by one of the investigators (SJC) by the same method at the same time of the day for the first seven days, and then weekly until the infants were weaned off nCPAP. The condition of the nose was documented systematically, and the presence of any of the five types of nasal trauma (redness, bleeding, crusting, excoriation, and narrowing of the passage) was recorded. If the initial investigator was unsure of the type of trauma sustained, a second opinion was sought from one of the other investigators (SCY). The intraobserver and interobserver bias had been minimised after a similar pilot study on the incidence of nasal trauma in infants during the use of nasal prong CPAP in our unit.
Assuming that the incidence of nasal trauma was 20% in the nasal prong group, it was calculated that a sample size of 37 infants in each arm was required to detect a difference of 10% between the two groups (two sided test) with a power of 80% at a significance level of 5%.
Statistical analysis was carried out using the statistical package SPSS version 10.1 (SPSS Inc, Chicago, Illinois, USA). Variables between the two arms of the study were compared. Categorical variables were analysed using the χ2 test (or Fisher’s exact test if the expected value was less than 5). Student’s t test was used to analyse continuous variables with normal distribution, and the Mann-Whitney U test for continuous variables with skewed distribution. Logistic regression analysis was carried out to determine the significant risk factors associated with nasal trauma (dependent variable) using various potential risk factors (duration of nCPAP treatment, type of nasal device used, birth weight, and gestation) identified during univariate analysis (with p values of <0.05) as independent variables. p<0.05 was considered significant.
RESULTS
A total of 212 VLBW infants were admitted to the neonatal intensive care unit during the study period. Of these, 125 received CPAP treatment; 97 (78%) of them were put on IFD and the remaining 28 (22%) were supported with bubble bottle CPAP because of a shortage of IFDs. Of the infants who used an IFD, parental consent was not obtained for eight. Thus only 89 infants were enrolled, with 41 randomised to the nasal mask group and 48 to the nasal prong group.
There was no significant difference in the ethnic and sex distribution between the two groups (p>0.05; table 1). Neither was there any significant difference between the two groups in the proportions of infants given antenatal steroids, surfactant treatment, and nCPAP on admission (p>0.05). There was also no significant difference in the mean birth weight, mean gestational age, mean Apgar scores at one and five minutes of life between the two groups (p>0.05). However, a significantly higher proportion of infants recruited to the nasal prong group were delivered by lower segment caesarean section (p = 0.02).
Comparison of ethnic origin, sex, and basic clinical data of infants using nasal mask versus nasal prong continuous positive airway pressure (CPAP)
There was no significant difference in the duration of conventional ventilation, duration of high frequency ventilation, duration of oxygen treatment, and hospital stay between the two groups of infants (table 2). There was no significant difference in the proportions of infants with nasal trauma between the two groups (p = 0.5). Neither was there any significant difference in the median interval between application of CPAP device and the onset of nasal trauma between the two groups. Although the infants in the nasal prong group received nCPAP for longer and had nasal trauma detected at an earlier median age than those in the nasal mask group, the differences were not significant (p⩾0.05). Neither was there any significant difference in mortality between the two groups of infants.
Comparison of clinical outcome between infants using nasal mask and nasal prong continuous positive airway pressure (CPAP)
Of the 12 infants who developed nasal trauma in the nasal mask group, six had crusting and/or excoriation on their nasal septum. Three developed narrowing of their nasal passage, and two sustained redness in their nasal mucosa. One infant had three types of trauma: bleeding, crusting, and excoriation. All these injuries (except for narrowing of the passage) were seen at the base of the nasal septum, at the junction between the philtrum and the base of the nasal septum.
Of the 17 infants who sustained nasal trauma in the nasal prong group, crusting and excoriation were seen in 10. Redness was noted in four, and one had bleeding from the inside of the nostrils. Two infants had more than one injury (one with narrowing of the passage and excoriation; and another with excoriation and bleeding from the site of injury). All these injuries (except for narrowing of the passage) were seen at the medial aspect of the nostrils at the nasal septum.
Table 3 compares the clinical variables of infants who developed nasal trauma with those without trauma after nCPAP. Infants with nasal trauma had significantly lower mean birth weight (p = 0.003) and longer mean duration of nCPAP treatment (p = 0.001) than those without trauma. Although infants with nasal trauma had lower mean gestational age than those without, the difference was not significant. There was no significant difference in the proportion of infants who were placed on nCPAP immediately on admission to the neonatal intensive care unit (p = 0.3). Logistic regression analysis showed that the only significant risk factor associated with the development of nasal trauma after nCPAP treatment was the duration of nCPAP (adjusted odds ratio 1.04; 95% confidence interval 1.01 to 1.07; p = 0.003) after various potential confounders had been controlled for. Birth weight, gestation, and type of nasal device were not significant risk factors.
Comparison of potential risk factors associated with the development of nasal trauma in very low birthweight infants after nasal continuous positive airway pressure (nCPAP)
DISCUSSION
This is the first reported randomised controlled study comparing nasal prong with nasal mask in infants receiving nCPAP. Nasal masks, which were used in the 1970s, were abandoned in the 1980s as there was difficulty in maintaining a good seal and they tended to obstruct the nasal airways.6–8 In recent years, the manufacturer of the IFD has produced soft silicon nasal masks, which can be used in place of the nasal prong. These nasal masks are softer and fit the nasal airway better than the older generations of nasal masks of the 1970s.
In this study, we found that, although not significant, the incidence of nasal trauma from nasal prong was higher than that resulting from the nasal mask. In a case series reported by Robertson et al,4 the incidence of nasal trauma resulting from nasal prong with the IFD was 20% in a group of VLBW infants. This is lower than our value, which may partly be because we included redness as a sign of trauma. We consider it important to include this mild form of trauma as it may progress to full blown trauma with prolonged use of nCPAP. In this study, redness injury alone accounted for 17% (two infants) of the trauma in the nasal mask group, and 23% (four infants) of the trauma in the nasal prong group. None of our patients developed nasal septum necrosis, and all 29 infants had recovered fully from their nasal injuries at the time of discharge from hospital. During the study, once trauma was detected, treatment was instituted immediately. If there was redness, excoriation, or crusting, a protective dressing (Duoderm) was applied to the area to prevent it worsening. This barrier protection may have helped to halt the progression of trauma in our patients as the point of maximum pressure was shielded, and healing was allowed to take place.
Although the types of injury were similar in the two groups, the sites of injury differed. In the nasal mask group, injuries occurred primarily at the base of the nasal septum at the junction between the nasal septum and the philtrum. This suggests that this is the area at which the mask exerts the greatest pressure, as prolonged pressure leads to impairment of tissue perfusion with resultant skin trauma. Injuries in the nasal prong group were confined primarily to the medial aspect of the nostrils on the nasal septum, indicating this to be the site of maximum pressure exerted by the prong. The lateral part of the nostrils may expand outwards when the prong are applied; the medial parts, being less mobile, are exposed to greater persistent pressure from the prong with resultant trauma.
Logistic regression analysis showed that the only significant risk factor associated with the development of nasal trauma after nCPAP was longer duration of nCPAP treatment. The prolonged use of nCPAP results in more pressure being exerted, and if there is any area of pressure points exerted by the device, this would definitely cause trauma. This finding suggests that monitoring of the infant’s nasal condition and proper application of the nasal device should be meticulously carried out to minimise trauma to the delicate skin of this high risk group of infants.
On the basis of the findings of this study, we recommend that nCPAP should be stopped as soon as it is no longer needed. There is a need to redesign the medial aspects of the nasal prong to be softer without compromising the efficacy of the CPAP delivery system. Currently, there are no published studies that suggest which site of trauma is of greatest clinical significance. However, we speculate that with constant injury to the inside of the nostril, there is greater risk of excessive production of nasal secretions leading to recurrent obstructive apnoea and potentially adverse sequelae.
What is already known on this topic
-
nCPAP is a common mode of respiratory support for preterm infants which can be delivered using prongs or mask
-
Nasal trauma has been reported with the use of nasal prongs but there are no studies on the efficacy and problems of using a mask
What this study adds
-
Nasal trauma is common during nCPAP treatment, which should therefore be terminated as soon as possible
-
No significant difference in the incidence of nasal trauma was found between the use of prongs or mask
In conclusion, there is no significant difference in the incidence of trauma caused by nasal prong and nasal mask. The only significant risk factor associated with the development of nasal trauma is longer duration of CPAP treatment.
Acknowledgments
This study was fully funded by a research grant (FF/28/2001) from the Faculty of Medicine, Universiti Kebangsaan, Malaysia.
Footnotes
-
Published online first 7 June 2005
-
Competing interests: none declared