Article Text

Abstract
Objective: To assess the accuracy of measurements of end tidal carbon dioxide (CO2) during neonatal transport compared with arterial and transcutaneous measurements.
Design: Paired end tidal and transcutaneous CO2 recordings were taken frequently during road transport of 21 ventilated neonates. The first paired CO2 values were compared with an arterial blood gas. The differences between arterial CO2 (Paco2), transcutaneous CO2 (TcPco2), and end tidal CO2 (Petco2) were analysed. The Bland-Altman method was used to assess bias and repeatability.
Results: Petco2 correlated strongly with Paco2 and TcPco2. However, Petco2 underestimated Paco2 at a clinically unacceptable level (mean (SD) 1.1 (0.70) kPa) and did not trend reliably over time within individual subjects. The Petco2 bias was independent of Paco2 and severity of lung disease.
Conclusions: Petco2 had an unacceptable under-recording bias. TcPco2 should currently be considered the preferred method of non-invasive CO2 monitoring for neonatal transport.
- Paco2, arterial partial pressure of carbon dioxide
- TcPco2, transcutaneous partial pressure of carbon dioxide
- Petco2, end tidal partial pressure of carbon dioxide
- NETS, Newborn Emergency Transport Service (Victoria)
- PAo2/Pao2 ratio, alveolar-arterial oxygen tension ratio
- transportation
- carbon dioxide
- monitoring
- mechanical ventilation
Statistics from Altmetric.com
- Paco2, arterial partial pressure of carbon dioxide
- TcPco2, transcutaneous partial pressure of carbon dioxide
- Petco2, end tidal partial pressure of carbon dioxide
- NETS, Newborn Emergency Transport Service (Victoria)
- PAo2/Pao2 ratio, alveolar-arterial oxygen tension ratio
Continuous non-invasive carbon dioxide (CO2) monitoring has become an important bedside tool in neonatal intensive care. Transported sick neonates should receive full intensive care, but arterial blood gas monitoring is not possible. Assessing the efficacy of ventilation during neonatal transport is challenging. Continuous non-invasive CO2 monitoring has been shown to increase the likelihood of the patient arriving at the receiving hospital with a normal pH and partial pressure of CO2 (Paco2).1
Transcutaneous CO2 monitoring is the most commonly used non-invasive CO2 monitoring system in neonatal intensive care and has been shown to accurately predict Paco2 and monitor CO2 trends.1,2 Calibrated transcutaneous partial pressure of carbon dioxide (TcPco2) has been shown to reliably approximate Paco2 during neonatal transport and has been recommended as an alternative to frequent Paco2 measurements.1 However, TcPco2 devices are difficult to use,3,4 bulky, and weigh between 2 and 6 kg, thus limiting their use during neonatal transport.
End tidal CO2 (Petco2) monitors are lightweight and may indirectly monitor Paco2.5–8 Hence, Petco2 may be more useful during transportation than TcPco2 monitoring. Studies of Petco2 monitoring in newborn infants have had mixed results, primarily because of the effects of ventilation perfusion mismatching on Petco2, failure to reach an expiratory plateau during rapid respiratory rates, and the technical limitations of Petco2 devices to interpret CO2 in small tidal volume states.2,5,9–12 Recent technological advances in Petco2 monitoring, such as smaller sample volumes and sample cells calibrated to neonatal tidal volumes, have attempted to overcome the limitations.13 Some authors advocate Petco2 as an acceptable method of approximation of Paco2 trends in newborn infants.10,14–16
The Newborn Emergency Transport Service of Victoria (NETS) is the largest neonatal transport service in Australasia. More than 900 infants a year are transported, with approximately one third ventilated. Monitoring of TcPco2 and oxygen saturation have been standard practice for five years to indicate ventilation adequacy during transport, and previous unpublished data have shown a close correlation between TcPco2 and Paco2.
Arterial blood gases and TcPco2 are commonly used to monitor ventilation. The aim of this study was to assess the accuracy and reliability of Petco2 monitoring during neonatal transport.
METHODS
Ventilated infants requiring road transport to a level 3 neonatal intensive care unit during March to August 2002 were recruited if the paediatrician involved in the transport was specifically trained to use both Petco2 and TcPco2 monitors, an arterial catheter was being used, endotracheal tube position could be confirmed by chest radiograph before transport, and both TcPco2 and Petco2 monitoring could be started before the first arterial blood gas was measured by the NETS team. Because of the effects of barometric pressure on Petco2, infants transported by air were not studied.5 Informed parental consent was obtained for each infant before transport.
Infants were not studied if they were older than 28 days, had a capillary refill time of greater than two seconds, or TcPco2 or Petco2 readings could not be made or were lost during transport.
TcPco2 was measured using the Microgas 7650 system (weight 5.6 kg) with Combi.M sensor 82 (Linde, Basel, Switzerland) applied to the skin of the anterior chest or abdomen. The manufacturers report that the Combi.M sensor 82, once calibrated, will remain accurate for up to four hours at one site. Petco2 was measured using a side stream end tidal analyser specifically designed for neonatal use (the Agilent Microstream system; Agilent Technologies, Andover, Massachusetts, USA); a result was the highest of five consecutive measurements.13 Arterial blood gases were analysed with the i-STAT portable clinical analyser (i-STAT Corporation, East Windsor, New Jersey, USA). Infants were ventilated using the Hoekloos Infant ventilator Mark 3 (Hoekloos, Amsterdam, Netherlands). The Australian Therapeutics Goods Administration has approved both devices for use in newborn infants. A specialist neonatal transport nurse and neonatal paediatrician escorted all infants.
After calibration of the TcPco2 and Petco2 monitors, paired CO2 measurements were recorded every 20 minutes, starting at stabilisation and continuing throughout the transport. The initial recordings were calibrated with a simultaneous Paco2. The NETS team was not blinded to the TcPco2 or Petco2 values; any ventilator changes were based on the TcPco2 or Paco2 values.
The severity of each baby’s lung disease was determined by calculating the alveolar to arterial oxygen tension ratio (PAo2/Pao2 ratio) where PAo2 = (Barometric pressure − 47) × (Fio2 − Pao2). Severe lung disease was defined as a PAo2/Pao2 ratio <0.3. A PAo2/Pao2 ratio of <0.3 has been associated with less precision of Petco2 measurements to estimate Paco2.15
The parents of all infants enrolled in the study provided written and signed informed consent for their infants to be transported by NETS and this involved specific consent to the use of all devices used in the study. This study was discussed with the Royal Women’s Hospital Ethics in Human Research Committee. It was decided that formal ethics approval was not required as the above written informed consent adequately informed the parents and addressed the ethical issues of the study.
Statistical analysis
The differences between Paco2, TcPco2, and Petco2 (expressed as P(a-Tc)co2, P(a-Et)co2, and P(Tc-Et)co2 respectively) were analysed using a Student’s paired t test, and their correlations were calculated. The Bland-Altman technique was used to assess agreement and repeatability.17 A bias of less than ± 0.7 kPa was considered clinically acceptable. Intrasubject P(Tc-Et)co2 variability over time was calculated.
RESULTS
Twenty six infants were enrolled, but five were excluded because the Petco2 could not be continuously measured in three, both TcPco2 and Petco2 could not be measured in another, and in the fifth infant the initial blood gas was venous. Table 1 summarises the characteristics of the 21 infants. A total of 21 P(a-Tc)co2 and P(a-Et)co2 differences and 82 P(Tc-Et)co2 differences (median recordings per subject 4.0 (range 2–10)) were calculated.
Characteristics of the 21 subjects enrolled in study
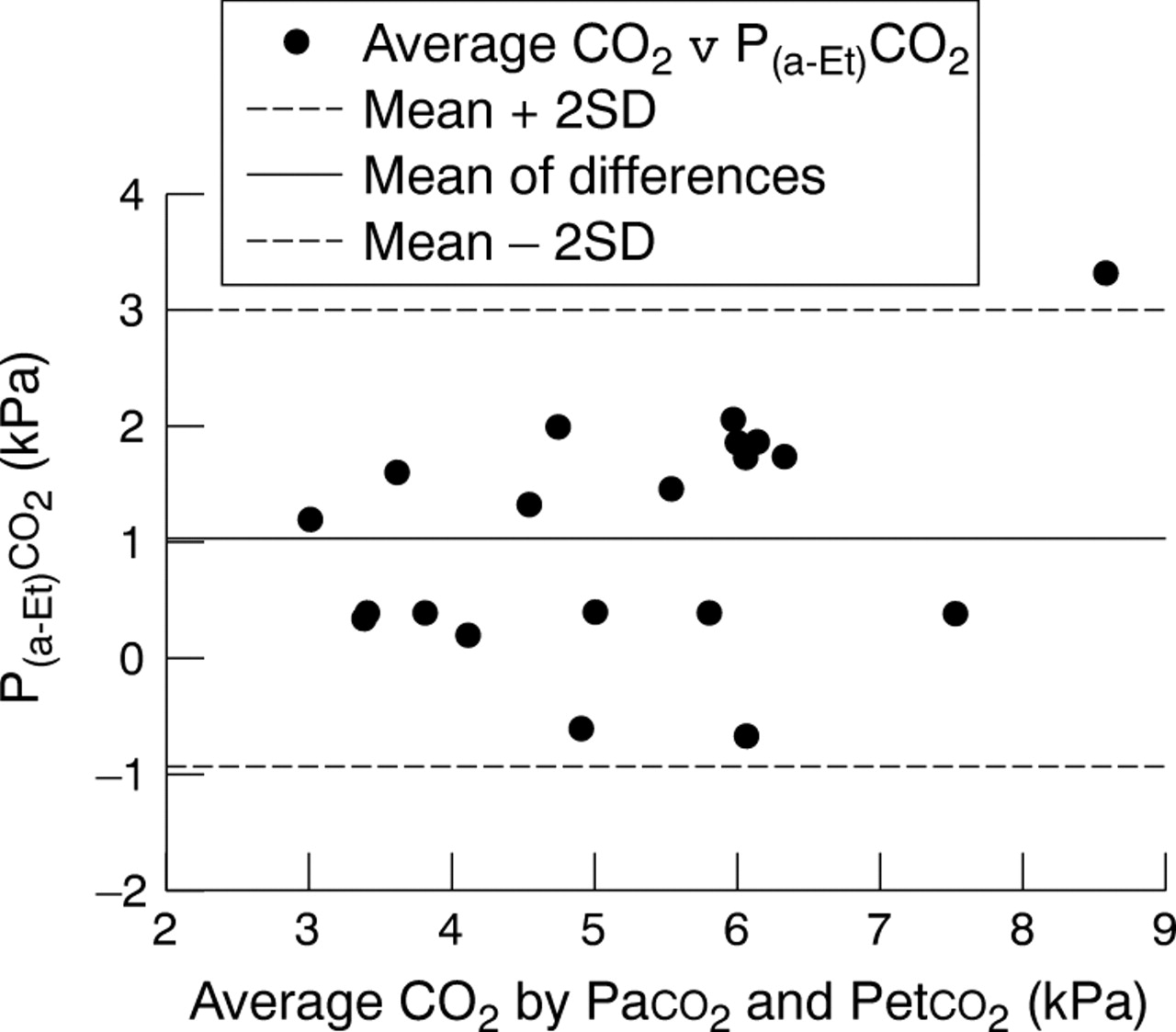
There was a linear relation between Petco2, Paco2, and TcPco2. However, Petco2 underestimated Paco2 by an average of 1.04 kPa (table 2, fig 1). Only 48% of Petco2 recordings were within 1.0 kPa of the paired Paco2. The bias of the Petco2 values was independent of the Paco2.
A comparison of CO2 (kPa) measured in three different ways
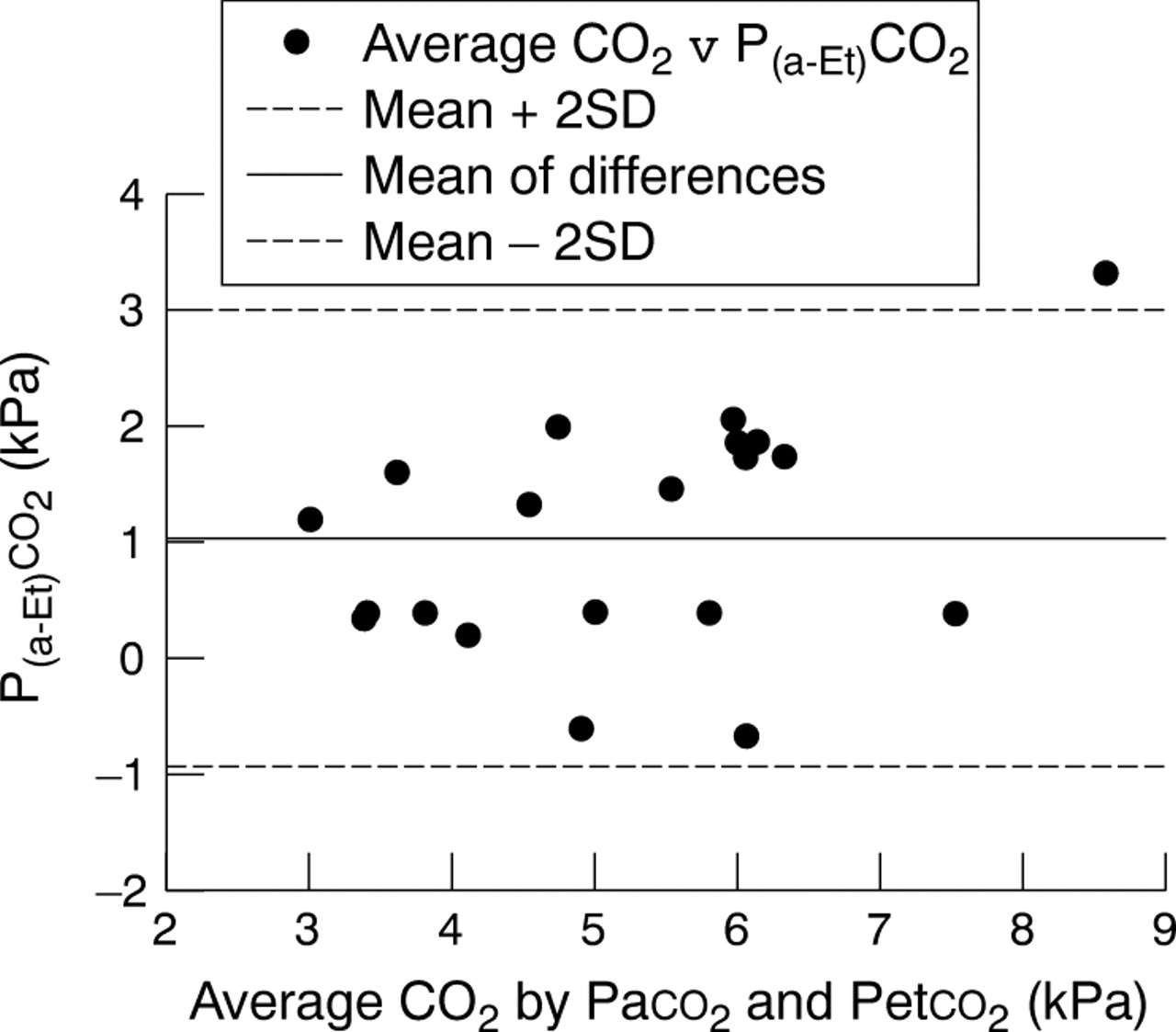
Bland-Altman plot of the difference between Paco2 and Petco2 (P(a-Et)co2) against average CO2.
TcPco2 was closely related to Paco2, with no significant difference between the two measurements (table 2). Two thirds of TcPco2 readings were within 0.7 kPa of the Paco2, and 81% of TcPco2 readings were within 1 kPa of the paired Paco2. There was no significant change in the difference between TcPco2 and Paco2 as the CO2 level changed (fig 2).

Bland-Altman plot of the difference between Paco2 and TcPco2 (P(a-Tc)co2) against average CO2.
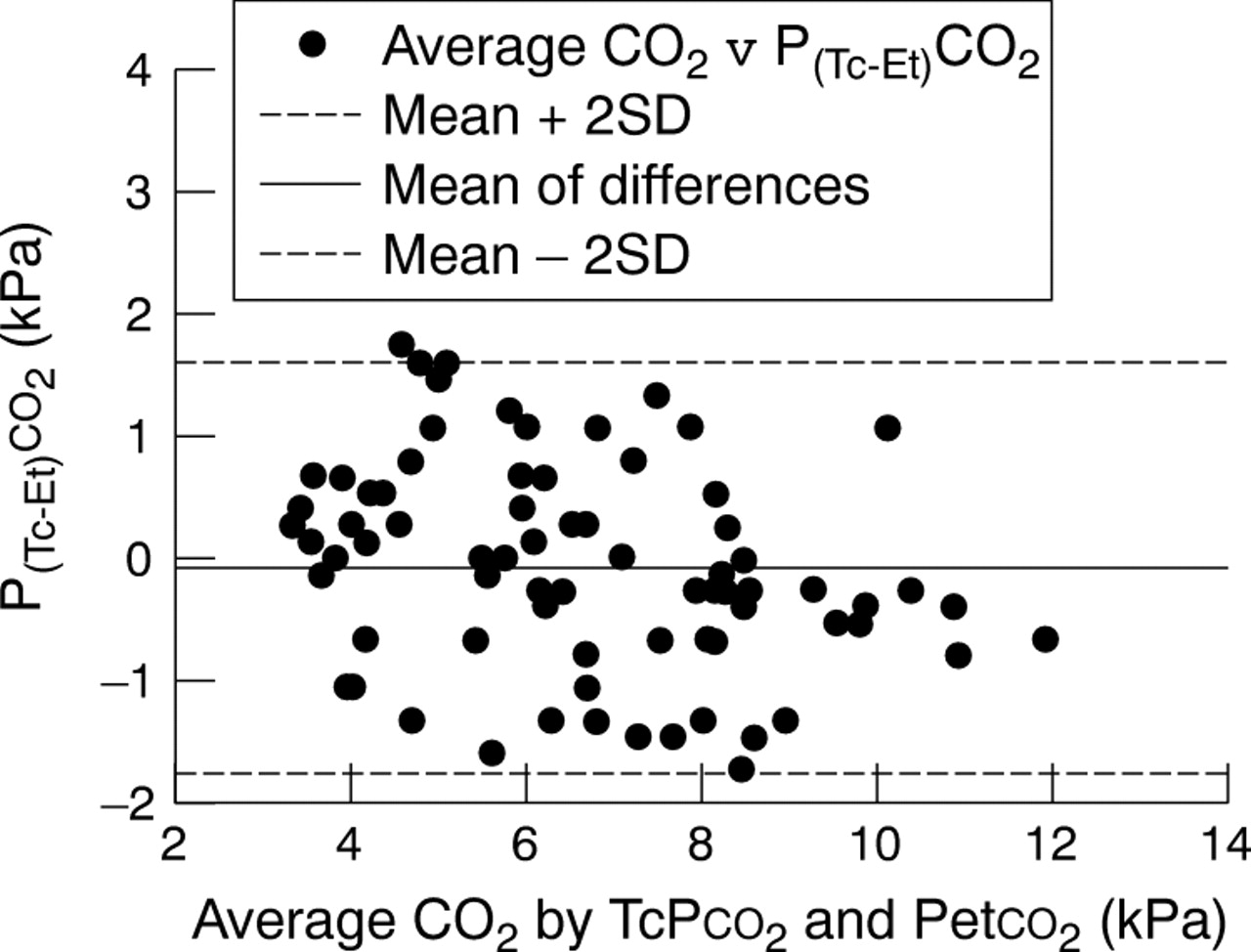
When the initial TcPco2 and Petco2 values for each subject were calibrated to the original Paco2, there was a closer relation between Petco2 and TcPco2: 64% of Petco2 values were within 0.7 kPa of the paired TcPco2 value (fig 3). Although the P(Tc-Et)co2 difference was not significant, the variability, as demonstrated by the Bland-Altman plot, was large (table 2, fig 3).
{kind=link}
{kind=link}
{kind=link}
Bland-Altman plot of the difference between TcPco2 and Petco2 (P(Tc-Et)co2) against average CO2.
There was no significant relation between Petco2 accuracy and severity of lung disease (table 3), although there was a non-significant trend towards Petco2 values being more likely to reflect either Paco2 or TcPco2 in infants with a PAo2/Pao2 ratio >0.3. Muscle relaxation did not alter the reliability of Petco2 to trend with TcPco2.
Relation between Petco2 values and severity of lung disease
DISCUSSION
This study shows that, in neonates requiring ventilation during transport, TcPco2 monitoring more accurately reflected Paco2 than Petco2 monitoring. Furthermore, Petco2 monitoring should be used with caution. Both Petco2 and TcPco2 were linearly related to Paco2 and each other. However, a linear relation alone (or correlation coefficients—the method used in many of the previous reports) does not adequately describe the agreement between two clinical measurement techniques.2,10,18 Assessing agreement between two methods of clinical measurement is complex. The method described by Bland and Altman is a more informative technique for assessing agreement, reliability, and repeatability, and allows interpretation within a clinical context.17 With the use of this technique, Petco2 was neither as precise nor reliable a method of assessing Paco2 during the transport of ventilated neonates, whereas TcPco2 provided a more reliable method. The degree of bias demonstrated between Petco2 and Paco2 (1.04 kPa) is clinically unacceptable.
Most of the infants in this study had mechanical ventilation instigated by the transport team; knowledge of any changes in the CO2 is essential for safe delivery of ventilation. Frequent Paco2 measurements are not practical during neonatal transport; a reliable non-invasive indicator of Paco2 is essential. Calibrated TcPco2 is an acceptable surrogate for Paco2 trends over time. Transcutaneous gas monitoring is an established and validated practice in neonatology.3 Newborn infants are particularly suited to transcutaneous monitoring because of their thin skin. Although proper use is dependent on appropriate training and placement, the only practical limitations are skin perfusion (which may be altered by vasoconstrictive agents, hypovolaemia, and oedema) and the temperature produced by the device. The response time of TcPco2 is too slow (30–50 seconds) to allow monitoring of the respiratory pattern.19 TcPco2 monitoring in neonatal transport has previously been evaluated and shown to result in improved ventilation on arrival at the receiving institution.1,20
What is already known on this topic
-
TcPco2 has been shown to be an accurate and reliable method of indicating Paco2 in neonates receiving intensive care
-
Although measurement of Petco2 can also indicate endotracheal tube position, in previous studies the ability to accurately reflect Paco2 has been variable
What this study adds
-
This study shows that TcPco2 accurately reflects Paco2 during neonatal transport, whereas Petco2 underestimates Paco2 by about 1.0 kPa, a clinically unacceptable difference
-
Petco2 was also unable to reliably reflect TcPco2 over time, therefore this study supports the use of TcPco2 as the preferred method of non-invasive CO2 monitoring during neonatal transport
Many authors have reported a good correlation between Petco2, TcPco2, and Paco2 in newborn infants, but in only three studies that evaluated Petco2 was the relation assessed using the Bland-Altman technique.14,15,21 Rozycki et al14 described a mean (SD) P(a-Et)co2 bias of 0.92 (0.92) kPa in 45 newborn infants receiving mechanical ventilation, with only 36.9% of Petco2 values falling within 0.67 kPa of the Paco2. The authors concluded that despite the significant bias, Petco2 provided a reliable estimate of Paco2 trends. A similar mean P(a-Et)co2 difference of 0.91 (0.68) kPa was reported by Tobias and Meyer21 in 25 infants and toddlers (up to 48 months of age) receiving mechanical ventilation for respiratory failure; the P(a-Tc)co2 difference in this study was 0.31 (0.18) kPa. Sivan et al15 obtained a clinically acceptable P(a-Et)co2 result, with a mean difference of 0.45 (0.88) kPa in a study involving 134 children (aged 2 days to 16 years) receiving mechanical ventilation. The mean P(a-Tc)co2 in this group was −0.17 (0.96) kPa. The P(a-Tc)co2 bias was related to skin perfusion but remained clinically acceptable. Primary diagnosis was not described in this study, nor was the proportion of the population who were newborn infants, making inference to the neonatal population difficult. Sivan and colleagues concluded that the degree of the P(a-Et)co2 bias was reduced in children with mild lung disease, as defined by a PAo2/Pao2 ratio of >0.3. In the cohort with severe lung disease, the mean P(a-Et)co2 1.04 (0.97) kPa was similar to our study.
Parenchymal lung disease with ventilation perfusion (V/Q) mismatching and a PaO2/PAO2 <0.3 is a feature of most causes of neonatal respiratory failure. During our study, only two infants did not require oxygen, and nearly all had parenchymal lung disease. Our study was not designed to assess the relation between degree of lung disease and Petco2 accuracy.
Petco2 monitoring has been validated in adult ventilated patients and healthy anaesthetised infants, but the infants in our study had respiratory failure.10,18 Petco2 is dependent on alveolar CO2 (PAco2) and the site of sampling. Non-uniform alveoli CO2 emptying patterns in patients with large ventilation perfusion mismatching result in PAco2 underestimating Paco2.5,22
Technical limitations of end tidal analysis in patients with high rate, low tidal volume breathing would have contributed to the difference between Petco2 and Paco2. To account for the fresh inhaled gas admixture during proximal Petco2 sampling, a minimum sampling flow rate of 150 ml/min is required.5 The end tidal analyser used in our study sampled at 50 ml/min. Despite manufacturer assurances, this may have had an impact on our results. The response time of end tidal analysers must be less than the respiratory cycle. The response time of the end tidal analyser used was 190 milliseconds, which is adequate for the ventilation rates used during the study, although at high respiratory rates with a short expiratory time, all exhaled alveolar gas would not have migrated to a proximal end tidal sampling site on completion of each respiratory cycle.5
The relation between TcPco2 and Petco2 was not constant over time within individuals, even when both values were adjusted to Paco2. In our opinion Petco2 monitoring cannot be used to reliably monitor trends in Paco2 over time in newborn infants with lung disease.
Despite our findings, Petco2 monitoring may offer some benefits over TcPco2 monitoring. Primarily the ability to rapidly and reliably confirm endotracheal tube position within the trachea, with either a capnograph or colorimetric end tidal CO2 indicator, is of great benefit within the noisy environment of neonatal transport.7 This study did not aim to assess the ability of Petco2 or TcPco2 to indicate endotracheal tube position. Inadvertent extubation is not a common occurrence in our transport population and did not occur in any of the neonates involved in this study. Further study is required to determine the role of Petco2 in ensuring the endotracheal tube position during transport.
CONCLUSIONS
Owing to the bias of about −1 kPa and lack of consistency in measuring Paco2 over time, Petco2 cannot be recommended during neonatal transport to monitor ventilation. TcPco2 monitoring was generally more precise, reliable, and agreed with Paco2. TcPco2 monitoring is the preferred method of non-invasive CO2 monitoring during neonatal transport.
REFERENCES
Footnotes
-
Published Online First 29 April 2005
-
Competing interests: none declared