Article Text

Abstract
Maintenance of neonatal normocarbia may prevent chronic lung disease and periventricular leucomalacia, but this requires frequent arterial sampling, which has risks. Alternative methods for measuring CO2 are therefore desirable. These include end tidal CO2, capillary sampling, and transcutaneous measurements. CO2 detectors have also proved effective and rapid indicators of endotracheal intubation. However, this method relies on the presence of exhaled CO2, which may be reduced in certain situations, such as cardiopulmonary arrest. Colorimetric CO2 detectors are therefore valuable adjuncts for airway management, especially during resuscitation, but Paco2 is still the best measure of CO2 in neonatal practice.
- Paco2, arterial partial pressure of carbon dioxide
- ETco2, end-tidal CO2
- ETT, endotracheal tube
- TcPco2, transcutaneous carbon dioxide
- ECMO, extracorporeal membrane oxygenation
- extracorporeal membrane oxygenation
- endotracheal intubation
- hypocarbia
- resuscitation
Statistics from Altmetric.com
- Paco2, arterial partial pressure of carbon dioxide
- ETco2, end-tidal CO2
- ETT, endotracheal tube
- TcPco2, transcutaneous carbon dioxide
- ECMO, extracorporeal membrane oxygenation
Maintenance of neonatal normocarbia may prevent chronic lung disease and periventricular leucomalacia.1,2 However, this requires frequent arterial sampling, potentially increasing the need for multiple blood transfusions.3 Indwelling peripheral or central arterial catheters or percutaneous arterial sampling are not risk free and have been associated with digital ischaemia and arterial spasm.4 Alternative methods for measuring carbon dioxide are therefore desirable and include end tidal carbon dioxide (ETco2), capillary sampling, and transcutaneous measurements. In addition, carbon dioxide detectors have proved to be effective and rapid indicators of endotracheal intubation.5 However, this method relies on the presence of exhaled CO2, which may be reduced in certain situations—for example, cardiopulmonary arrest. We highlight situations in which false positive and negative results may occur using colorimetric CO2 detectors in neonates and instances in which CO2 monitoring may be beneficial.
CONTINUOUS ETco2 DETECTORS
Continuous ETco2 detectors or capnometers measure exhaled CO2 and use either infrared absorption or mass spectroscopy to display a numerical value of CO2 tension in mm Hg or % CO2.6 Capnometers used in clinical practice use two different sampling techniques: sidestream and mainstream sampling. A mainstream capnometer has an airway adaptor cuvette attached in-line and close to the endotracheal tube (ETT). This method is more accurate than sidestream sampling. The cuvette incorporates an infrared light source and sensor that senses CO2 absorption to measure the partial pressure of CO2 (Paco2). A sidestream capnometer uses a sampling line that attaches to a T-piece adapter at the airway opening, through which the instrument continually aspirates tidal airway gas for analysis of CO2.7
Another measure of CO2 is capnography, which graphically displays expired CO2 over time and may be useful for trending CO2 concentrations. Low flow capnography with microstream technology accurately measures alveolar CO2 in newborns without pulmonary disease, as demonstrated by normal ETco2-Paco2 gradients.8 The measured ETco2-Paco2 gradient is significantly higher in newborns with pulmonary disease,8 and alveolar pathology could probably be missed by sidestream capnography.9,10 Capnography allows more rapid determination of both tracheal and unintended oesophageal intubation than clinical assessment in neonates during resuscitation.11,12 ETco2 wave pattern distribution among preterm infants is distinctly different from that of term controls, whereas inspiration is related to the degree of maturity.9
Poor overall correlation of the ETco2 and Paco2 (r = 0.39, p<0.01) was observed by Watkins and Weindling13 in a study of 19 infants (69 samples). However, two studies showed good correlation between ETco2 and Paco2. In a study of 60 infants, Wu et al14 observed a correlation in both term infants (44 samples, r = 0.78, p<0.001) and preterm infants (86 samples, r = 0.85, p<0.001). Nangia et al15 in a study of 152 samples observed a significant correlation between Paco2 and ETco2 in preterm infants <32 weeks (p<0.01).
Continuous ETco2 is a close measure of arterial CO2 partial pressures in patients with normal ventilation and perfusion and a reliable measure of endotracheal intubation.6 Neonates have a smaller tidal volume and a higher respiratory rate giving a shorter inspiratory time. Therefore they may have a wide variation in ETco2 values, as true alveolar gas is not always measured. ETco2 monitoring in patients in the neonatal intensive care unit is as accurate as capillary or transcutaneous monitoring, but less precise than the latter. It may be useful for trending or for screening patients for abnormal arterial CO2 values.16
TRANSCUTANEOUS CO2 DETECTORS
The thin epidermal layer of preterm infants is advantageous in the accurate measurement of transcutaneous CO2 (TcPco2). The disadvantages include heat induced skin damage and burns from the electrodes.17,18 In addition, inadequate tissue perfusion and acidosis may alter the TcPco2 correlation with Paco2.19,20 TcPco2 improves short term respiratory outcome in neonates receiving mechanical ventilation during transport and has been successfully used for infants on high frequency oscillatory ventilation.21–23 It has been shown to be superior to ETco2 during neonatal transport as the latter has a significant under-recording bias.21
Several neonatal studies have shown a better agreement between TcPco2 with Paco2 than ETco2.24–28 For eaxmple, Hand et al,24 in a study of 12 preterm infants (51 samples), observed a linear correlation between TcPco2 and Paco2 (r = 0.71, slope = 0.9), but not with ETco2 (r = 0.52, slope = 0.42). Another study of 12 infants (72 samples) by Geven et al25 found good correlation with TcPco2 (r ranged from −0.29 to +0.95) but not ETco2 (r ranged from −0.99 to +0.97). Aliwalis et al27 studied 27 ventilated preterm infants in the first 24 hours of life and showed moderate agreement between non-invasive methods and Paco2, although birth weight, site of transcutaneous probe application, mean blood pressure, and mean arterial pressure did not influence the agreement.
However, sensor preparation, positioning, taping, and repeated changes of the sensor location make the handling difficult and complicate its use in the neonatal intensive care unit. Another caveat is the need to correlate the TcPco2 with an initial arterial CO2 value.29,30 Recently, a new sensor for combined assessment of pulse oximetry oxygen saturation and TcPco2 has been introduced (TOSCA Monitor; Linde Medical Sensors, Basel, Switzerland). The monitor combines pulse oximetry and ETco2 measurement in a single ear sensor, which works at 42°C to enhance blood flow in capillaries below the sensor and reduces motion artefacts because of less head movement in the newborn.31 Despite these problems, TcPco2 remains an important method of monitoring CO2 in neonates, as it may offer a reliable trend over time with the Paco2 and could guide clinicians to changes in the state of the lung and minimise the need for blood gas analysis.28
OVERVIEW OF COLORIMETRIC ETco2 DETECTORS
Use of portable, disposable, colorimetric ETco2 detectors is a rapid and efficient method of ascertaining correct intratracheal ETT placement.32 The device (Pedi-Cap from Nellcor, Inc, Hayward, California, USA; CO2 Clip from Portex Inc, Keene, New Hampshire, USA) is connected in series between the ventilator and the ETT. It contains a pH sensitive chemical indicator (metacresol purple), which changes from purple to yellow with expired CO2. Correct use requires the confirmation of persistent reversible colour change (from purple to yellow) with each inspiration and expiration after six complete breaths are delivered.
Colorimetric detectors are extremely accurate in animal studies, in children weighing >2 kg, and in adults.32–34 The minimum CO2 concentration needed for colour change has been shown to be 0.54% (0.5 kPa), whereas the maximum colour change occurs above 2–5 kPa (2–5%).32 The paediatric colorimetric detector has a dead space of 3 ml and a flow resistance of 2.5 (0.5) cm H2O at 10 litres/min (Pedicap) and allows brief usage in infants up to 1 kg.32
ADVANTAGES OF ETco2
One of the most common causes of neonatal intubation failure is inadvertent oesophageal intubation, which can have catastrophic consequences.32 Direct visualisation of the ETT passing through the vocal cords, ETT condensation, observation of chest wall movement, and auscultation of breath sounds are commonly used clinical signs to aid confirmation of correct ETT placement. However, as none of these are infallible, the addition of CO2 detection using the colorimetric device is a very useful adjunct to clinical assessment. The disposable ETco2 detector significantly decreases the time for clinical determination of ETT position in neonates.
The detector also has prognostic value for return of spontaneous circulation and short term survival in adults and children.35,36 In adults, none of the patients with colorimetric ETco2 <2% were successfully resuscitated after cardiopulmonary resuscitation.32
CONFOUNDERS IN THE USE OF COLORIMETRIC ETco2
There are several limitations to the use of colorimetric ETco2 in neonates. Figure 1 lists causes of apparent false positive and false negative results. Colorimetric ETco2 detectors cannot detect hypocarbia or hypercarbia, right main stem bronchus intubation, or oropharyngeal intubations in spontaneously breathing patients.32 If the colorimetric detector is contaminated with acidic gastric contents or drugs such as adrenaline (epinephrine), there is fixed yellow discoloration and results are unreliable. Humidity decreases the clinical lifespan of the detector from a maximum of two hours (Portex) or 24 hours (Smiths).

Colorimetric end tidal CO2 (ETco2) detectors: possible causes of apparent false positive and negative results in neonates. VA ECMO, Venoarterial extracorporeal membrane oxygenation.
The adult device has a dead space of 38 ml and is not recommended in children weighing <15 kg, as the large dead space of the detector may dilute the child’s small tidal volume, producing a false negative result and potentially inducing hypercarbia from hypoventilation.32 In addition, abiding by the manufacturer’s recommendations of six complete ventilations for colour change may result in gastric distension if the ETT is misplaced in the oesophagus, resulting in the loss of valuable time during resuscitation. Although useful in confirming correct ETT placement, this device shows minimal changes if used continuously, for example during paediatric transport.37 Capnoflo resuscitators which have the colorimetric strip incorporated in the clear connector of the ventilator bag have shown similar results.37
CO2 is a product of cellular metabolism and is removed through the circulation and the lungs. Therefore ETco2 reflects ventilation, metabolism, and circulation.32 During cardiopulmonary resuscitation, a positive test confirms placement of the ETT within the airway, whereas a negative test indicates either oesophageal placement or airway intubation with poor or absent pulmonary blood flow.38 In this situation, an alternative means of assessing ETT placement is required. Aziz et al39 showed only three false positives in patients with severe cardiopulmonary arrest in a study of 45 neonates.
During neonatal resuscitation, the transition from fluid to air filled lungs may reduce alveolar gas exchange and exhaled CO2 sufficiently to cause a false negative result. This may induce significant neonatal morbidity caused by erroneous extubation and delay in establishing adequate ventilation. Similar results may occur in infants with cardiac anomalies, pulmonary hypoperfusion, myocardial dysfunction, or hypoxaemia after asphyxia. Severe airway obstruction such as liquid inhalation (fluid, blood, or meconium) may produce CO2 concentrations below the device’s detection limit because of ventilation-perfusion mismatch.40,41 False negative results may also occur in severely hypocarbic neonates especially those weighing <1 kg.
Neonates requiring venoarterial extracorporeal membrane oxygenation (ECMO) may also potentially show a false negative result with the ETco2 detector. In this scenario, the membrane oxygenator, bypassing the pulmonary circulation, removes CO2, resulting in significantly reduced ETco2. Reintubation of an infant on ECMO is associated with slower ETco2 colour change, and additional clinical signs of ETT placement are essential.
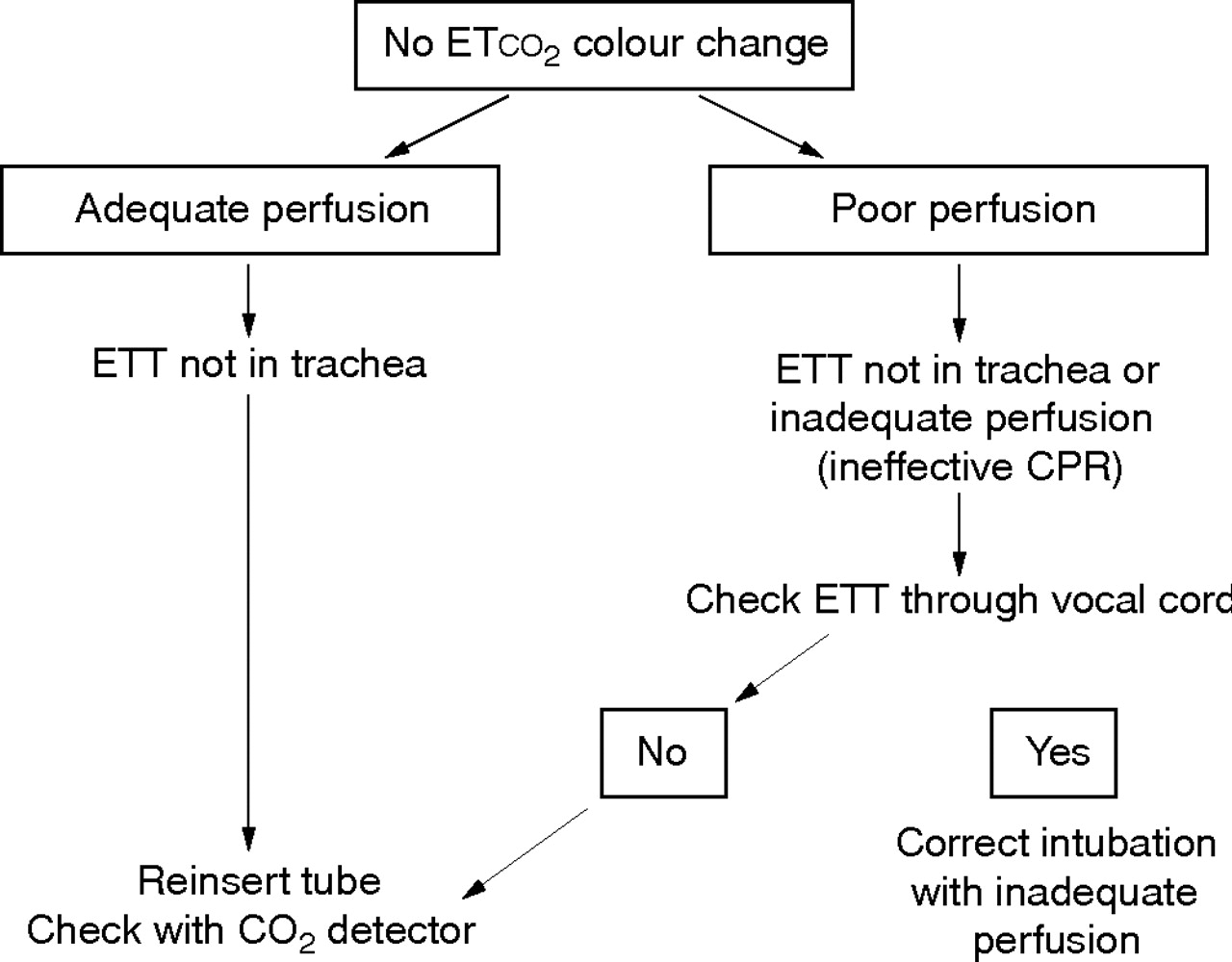
Disposable colorimetric ETco2 detectors are a valuable clinical tool in neonatal airway management. Their advantages have been confirmed in neonates weighing >2 kg with good cardiac output and spontaneous circulation.32 Non-invasive methods of CO2 monitoring (TcPco2, ETco2) have been shown to have moderate agreement with Paco2 in preterm infants in the first 24 hours of life.27 However, there are several specific neonatal caveats to their use. Absence of ETco2 colour change especially during cardiopulmonary arrest may not always be an indication for reintubation, and further clinical assessment is vital (fig 2). Therefore, in addition to the ETco2 detector, careful establishment of the presence of bilateral breath sounds and ETT placement by direct visualisation and other clinical signs is essential. Additional research is required to establish the role of ETco2 detectors in neonatal resuscitation especially in cases of reduced pulmonary blood flow, meconium aspiration, and cardiopulmonary arrest.
{kind=link}
{kind=link}
Clinical algorithm for management if no colorimetric end tidal CO2 (ETco2) colour change. ETT, Endotracheal tube; CPR, cardiopulmonary resuscitation. Adapted from the Nellcor clinical datasheet.
CONCLUSIONS
Although Paco2 sampling remains the gold standard in neonatal care until non-invasive technology is further refined, colorimetric CO2 detectors are very valuable adjuncts for airway management, especially during resuscitation. If non-invasive CO2 methods are used, the user should be aware of the limitations. TcPco2 is still the best non-invasive indicator of CO2 trends over time, especially in preterm infants or infants with respiratory disease.
REFERENCES
Footnotes
-
Competing interests: none declared