Article Text

Abstract
Background: Techniques of positioning and holding neonatal face masks vary. Studies have shown that leak at the face mask is common and often substantial irrespective of operator experience.
Aims: (1) To identify a technique for face mask placement and hold which will minimise mask leak. (2) To investigate the effect of written instruction and demonstration of the identified technique on mask leak for two round face masks.
Method: Three experienced neonatologists compared methods of placing and holding face masks to minimise the leak for Fisher & Paykel 60 mm and Laerdal size 0/1 masks. 50 clinical staff gave positive pressure ventilation to a modified manikin designed to measure leak at the face mask. They were provided with written instructions on how to position and hold each mask and then received a demonstration. Face mask leak was measured after each teaching intervention.
Results: A technique of positioning and holding the face masks was identified which minimised leak. The mean (SD) mask leaks before instruction, after instruction and after demonstration were 55% (31), 49% (30), 33% (26) for the Laerdal mask and 57% (25), 47% (28), 32% (30) for the Fisher & Paykel mask. There was no significant difference in mask leak between the two masks. Written instruction alone reduced leak by 8.8% (CI 1.4% to 16.2%) for either mask; when combined with a demonstration mask leak was reduced by 24.1% (CI 16.4% to 31.8%).
Conclusion: Written instruction and demonstration of the identified optimal technique resulted in significantly reduced face mask leak.
Statistics from Altmetric.com
In a study comparing the Laerdal and new Fisher & Paykel round face masks, we found that during simulated neonatal resuscitation mask leak varied widely irrespective of the mask, operator experience or technique of mask application.1 The average mask leak was greater than 55% and the techniques of mask application varied considerably.1
Successful neonatal face mask ventilation requires an airtight seal between the rim of the mask and the face.2–4 Achieving this can be difficult.5 Efficacy of mask ventilation is judged by observing chest rise and an increase in heart rate.6 Leak at the face mask is a common reason for failure of ventilation2 and often occurs between the cheek and bridge of the nose at the orbital margin.3 4 It is a widespread misconception that using a manometer allows the operator to detect leaks.7 8 Even with large leaks, in the presence of a high gas flow into the system, the set pressure is achieved.1 8 9 Many participants in our previous study were unaware of their leak and most were unable to accurately assess the leak during positive pressure ventilation (PPV).1
Face mask ventilation is a mandatory skill for staff caring for newborn infants10 and training employs a variety of educational tools.2 3 11–14 Recommended techniques of mask placement and hold are variable,2–4 6 13 and have not been formally studied.
Round-shaped masks are the most widely used designs,15–17 and are more easily cleaned.15 18 A correctly sized mask should cover the nose and mouth,2–4 6 19 without extending beyond the chin tip or encroaching on the eyes.2–4 6 Applying excessive pressure may bruise the face and mould the back of the head.3 4
The primary aims of this study were to: (1) identify the technique for placing and holding a face mask which minimised mask leak during simulated neonatal resuscitation; (2) investigate the effect of written instruction and a demonstration of the identified technique on reducing mask leak from a Laerdal round mask and a Fisher & Paykel mask. A secondary aim was to determine whether leak at the face mask differed between the two mask designs following training.
METHODS
Equipment
Face masks
The size 0/1 Laerdal round mask (LR) (Laerdal, Stavanger, Norway) and the 60 mm Fisher & Paykel (FP) (Fisher & Paykel Healthcare, Auckland, New Zealand) “round” neonatal resuscitation mask were the appropriate sizes for the manikin. Participants had used the FP mask once previously and the LR mask is in routine use at our hospital.
Manual ventilation device
The Neopuff infant resuscitator (Fisher & Paykel Healthcare, Auckland, New Zealand) was used. It is a continuous flow, pressure limited, T-piece device with a built-in manometer and a positive end expiratory pressure (PEEP) valve. The operator set the gas flow to 8 l/min, the peak inspiratory pressure (PIP) to 30 cm H2O and PEEP to 5 cm H2O.
Modified manikin
A Laerdal Resusci baby manikin (Laerdal, Stavanger, Norway) was modified by replacing the original “lung” with a 50 ml test lung (Dräger, Lubeck, Germany) connected by non-distensible tubing to the mouth by an airtight seal. It was positioned so inflation caused chest rise. A pressure monitoring line was connected to the airway tubing immediately proximal to the test lung. The compliance of this whole system when pressurised to 30 cm H2O was 0.5 ml/cm H2O, with a maximal test lung volume at this pressure of 65 ml.
Respiratory monitor, recording equipment and values measured
A Florian respiratory monitor (Acutronic Medical Systems, Ag, Switzerland) was used to measure inflating pressures and gas flow. The flow sensor was placed between the T-piece and face mask. The tidal volume passing through the sensor was calculated by integrating the flow signals and calibrated with a 10 ml syringe. Percentage leak at the face mask was the difference between the inspired and expired tidal volumes, expressed as a percentage of the inspired tidal volume
(Percentage leak = [(inspiratory tidal volume – expiratory tidal volume) ÷ inspiratory tidal volume] ×100)
Airway pressure was measured directly and calibrated against a column of water.
Mask leak rather than tidal volume is presented because it is the best way to compare different techniques and masks with different volumes and compliance.
The Spectra software programme (Grove Medical, London, UK) was used to acquire output from the Florian monitor through an analogue to digital converter onto a dedicated computer. The Florian monitor and computer screen were not visible to participants.
Determining the technique for mask placement and hold that minimises leak
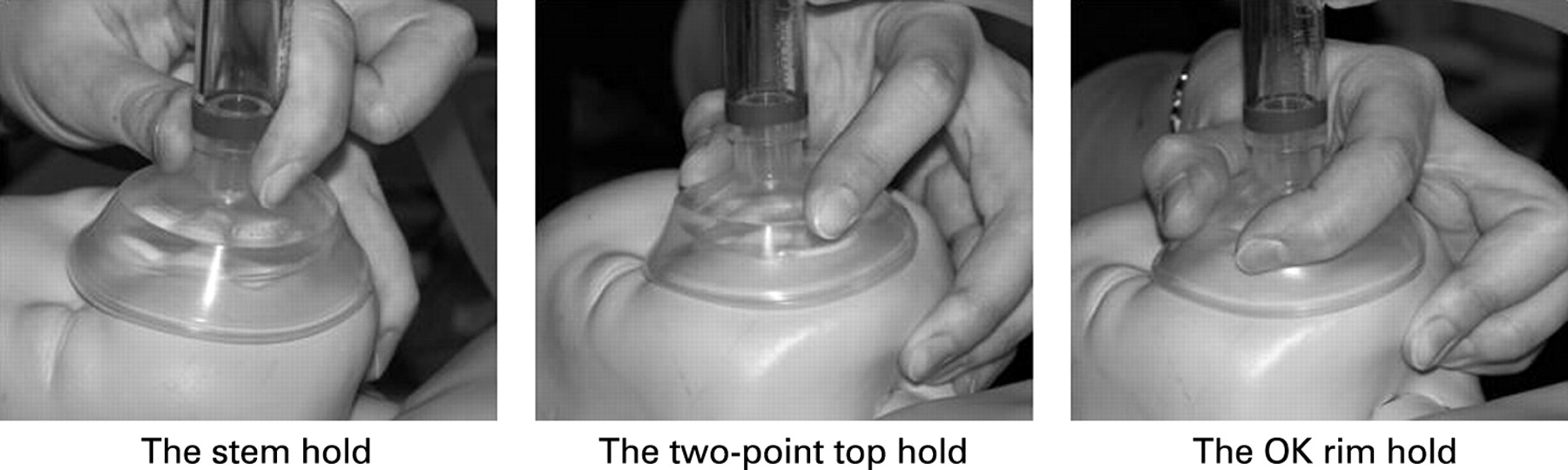
Three experienced neonatologists investigated recommended techniques of positioning and holding face masks2–4 6 13 19 to determine the method that minimised leak. These techniques included: two ways of positioning a mask on the face; placing it straight onto the face or rolling it onto the face beginning at the chin tip.3 4 There were three methods of holding the mask on the face, which are shown in figure 1: “The stem hold”—where the mask stem is held between the index finger and thumb.13 “The two-point top hold”—the thumb and index finger apply balanced pressure to the top flat portion of the mask where the silicone is thickest. The stem is not held and the fingers should not encroach onto the skirt of the mask.13 “The OK rim hold”—the thumb and index finger form a C shape (as in the “OK” hand gesture) placed around the top flat portion of the mask applying an even distribution of pressure to the outer edge and not encroaching onto the skirt of the mask.4 Jaw lift was also investigated; it was applied by using the third, fourth and fifth fingers to lift the chin forward4 against the downward pressure on the mask.
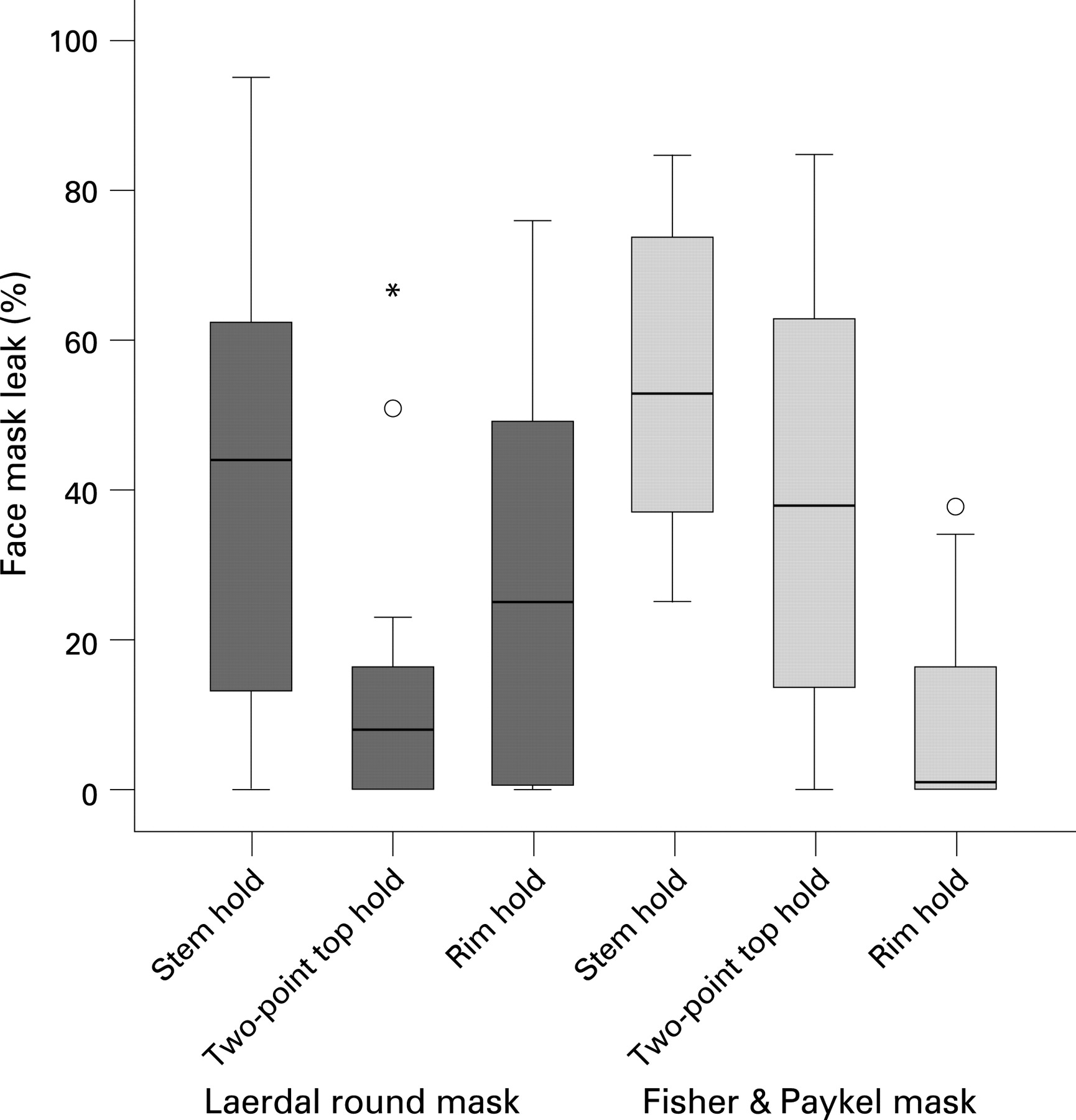
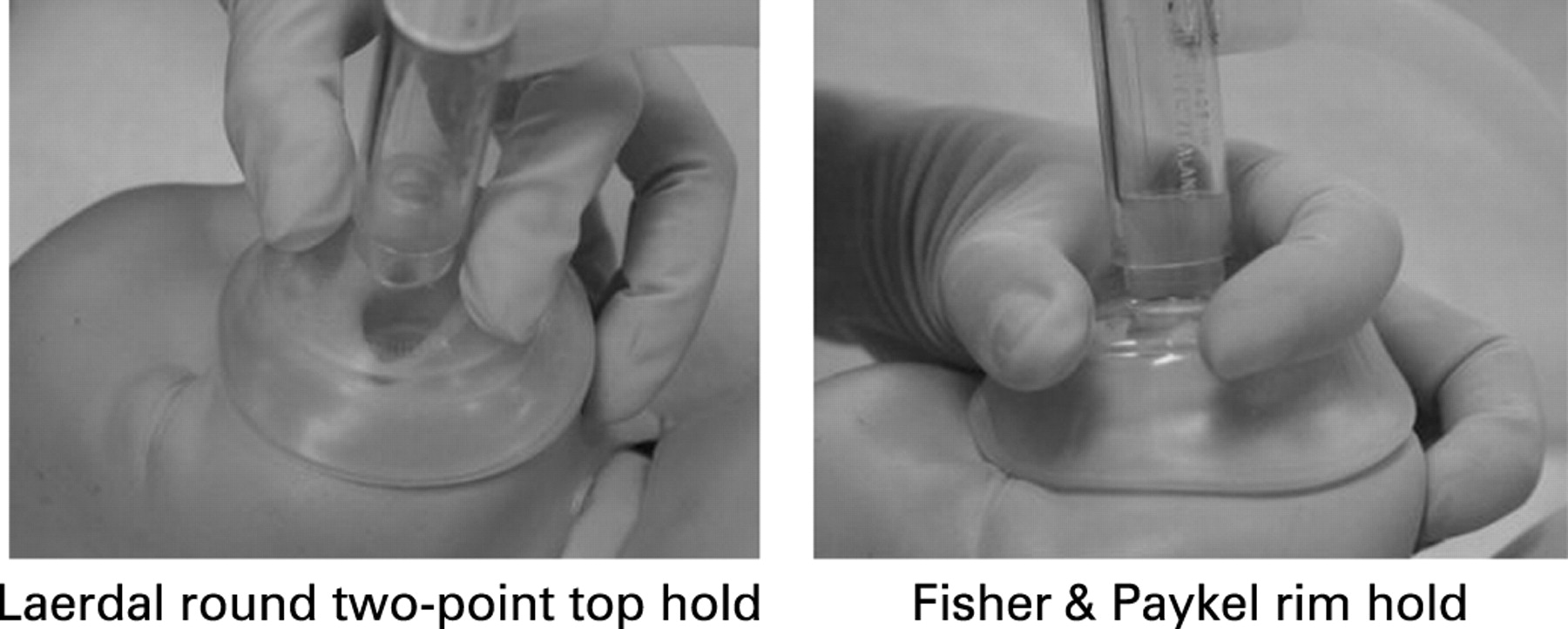
The three neonatologists tested the different components of each technique. They found that rolling the mask upwards onto the face from the chin tip resulted in more accurate positioning of the mask and reduced the leak at the orbital margin. Jaw lift reduced the leak and also reduced the downward pressure onto the manikin’s head. Rolling the mask onto the face and jaw lift were subsequently used with each of the three mask holds. When they were satisfied they had perfected all techniques each neonatologist ventilated the modified manikin using the three holds with each mask five times (15 tests in total for each mask hold combination). Each recording lasted 1 minute. The results are shown in figure 2, where mean percentage mask leak is grouped by type of hold for each mask design. The lowest median leak was found with the two-point top hold for the LR mask and with the rim hold for the FP mask (fig 3). During this process two clinical cues, which identified the presence of a good mask seal, were identified; a whistling/hissing sound from the PEEP valve during expiration and the maintenance of PEEP at the set level.

Setting and participants
The 50 clinicians from our first study1 took part in this study. They included consultants, fellows, registrars, neonatal nurses and midwives of the Royal Women’s Hospital, Melbourne, Australia. Their years of neonatal experience were recorded.
Study protocol
The results of our first study1 provided the baseline percentage mask leak, ventilation rate, PIP and PEEP for both mask designs and for each participant using their usual techniques of mask application before any training; these data are presented in the results as “before instruction.”
Each participant received written instructions containing text and photographs of the techniques the investigators found to have the least leak for each mask. Before each recording, participants were given time to familiarise themselves with the equipment. Participants were asked to ventilate the manikin for 2 minutes at a rate of 40–60 inflations per minute with a PIP of 30 cm H2O and a PEEP of 5 cm H2O ensuring that they were achieving adequate chest rise. We measured the mean ventilation rate, PIP, PEEP, inspired and expired tidal volumes and percentage leak for 2 minutes with each mask, excluding the first five inflations in each case.
The best technique for each mask was then demonstrated to each participant by one instructor (FEW). The inability to achieve the set PEEP with a large leak was demonstrated; as was the presence of a strong whistling/hissing noise from the PEEP valve of the Neopuff, which occurs with minimal face mask leak. Recordings were then made for 30 seconds of PPV with each mask, excluding the first three inflations in each case. Participants knew face mask leak was being assessed.
Participant survey
At the end of the assessments participants were asked, “Would you now feel more or less confident using this mask to deliver intermittent positive pressure ventilation (IPPV) in a resuscitation situation with the ‘two-point top hold’ for the LR mask and … with the ‘OK Rim hold’ for the FP mask.” There were five possible responses ranging from much more confident to much less confident.
Randomisation and statistical analysis
The order of assessment of the two masks was determined by a computer generated randomisation list. Data were analysed using SPSS version 12.0 and Stata 9.2. Multiple linear regression was used to investigate the difference in face mask leak between the two masks and to assess the influence of technique training on mask leak. The regression analysis uses robust standard errors to allow for the repeated measures. Paired t tests were used to compare other ventilation parameters. A p<0.05 was considered significant. Data are expressed as mean (SD) or percentage unless otherwise stated.
RESULTS
Participants
There were 10 participants in each professional category. The median years of experience were: consultants 18.5 years, fellows (SpR level) 3.3 years, registrars (SHO level) 0.1 years, neonatal nurses 9.5 years and midwives 3.5 years. A total of 10 648 inflations were recorded and analysed.
The effect on mask leak for the three holds and two masks is shown in figure 2. The median percentage leak for the two-point top hold and the rim hold was the smallest and least variable for the LR and FP masks, respectively. These two holds are shown in figure 3. Participants’ usual techniques were presented in our first study.1
Inflation pressures and rate
The mean (SD) PIP, PEEP and ventilation rates with the LR mask were 29.3 (2.8) cm H2O, 4.0 (0.7) cm H2O and 49 (19.8)/min before instruction and 29.7 (2.1) cm H2O, 4.0 (0.8) cm H2O and 54 (36.9)/min after instruction. With the FP mask they were 29.3 (1.8) cm H2O, 3.9 (0.7) cm H2O and 52 (38.1)/min before instruction and 29.7 (1.9) cm H2O, 4.1 (0.7) cm H2O and 49 (13.7)/min after instruction. There was no significant difference between the two masks before or after instruction. The only significant difference following instruction was for the FP mask where the PEEP increased by 0.2 cm H2O (p = 0.038, CI 0.1 to 0.4).
Percentage gas leak at the face mask
The mean (SD) percentage leak before instruction, after instruction and after demonstration of the optimal techniques was 55% (31), 49% (30), 33% (26) and 57% (25), 47% (28), 32% (30) for the LR and FP masks respectively. There was no significant difference between the two masks.
Compared with the mean percentage mask leak of participants before instruction, with either mask, written instruction reduced mask leak by 8.8% (CI 1.4% to 16.2%, p = 0.02), the demonstration further reduced leak by 15.3% (CI 9.0% to 22.7%, p<0.0005). The combined effect of written instruction followed by a demonstration reduced leak by 24.1% (CI 16.4% to 31.8%, p<0.0005). Figure 4 shows a box-plot of percentage mask leak for each mask design before and after training.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Participant survey responses
For the LR mask using the “two-point top hold,” 32% were much more/more confident, 50% neutral/no change and 18% much less/less confident. For the FP mask with “the OK rim hold,” 56% were much more/more confident, 24% neutral/no change and 20% much less/less confident.
DISCUSSION
This study identified techniques of placing and holding neonatal face masks which minimised mask leak. Teaching participants these techniques significantly reduced the leak when they ventilated a modified manikin. There was no significant difference in face mask leak between the two neonatal masks before or after technique training.
With variable and unmeasured mask leaks variable tidal volumes are delivered to the lungs. A large leak may reduce the tidal volume and a small leak, with a fixed inflating pressure, may result in excessive tidal volumes. Successful neonatal resuscitation is dependent on delivering an appropriate tidal volume. Controlling the face mask leak is one part of achieving this.
This study was done using a modified manikin; the results may be different with newborn infants.
A criticism of this study is that the reduction in leak may have resulted from the experience gained by the participants as the studies progressed. If this were the case it is likely that the most experienced clinicians would have lower leaks; however we found a wide and similar variation across all professional categories. This variation in performance irrespective of experience was previously reported.9 20 If experience was important then we would have expected the leak to be lower with a familiar mask than with a new mask; this was not the case.
Caution should be applied in extrapolating the results of this study. Different devices have different characteristics—for example, self inflating bags without PEEP will have a lower leak. The use of different inflation times (Ti) will also alter leak. We did not measure Ti in our study but it is unlikely that this systematically changed through the different phases of the study.
Clinical skills are best taught in stages and both theoretical knowledge and practical demonstration are important.3 13 21 We have seen that a significant reduction in leak can be achieved with written instruction alone; with a further important reduction in leak after the technique was demonstrated.
It has been shown that the manometer does not reliably identify mask leak unless it is very large.1 8 9 During face mask ventilation, poor mask application and resultant variable mask leaks affect the tidal volume delivery, which may be inadequate for effective gas exchange.7 22 The delivery of very low tidal volumes as a result of large mask leaks could result in failure to resuscitate an infant. Clinical cues, which suggest mask leak, were identified and used in the education process.
This study has shown that identifying, teaching and demonstrating improved techniques of placing and holding neonatal face masks reduces leak with a modified manikin. This may lead to improvements in the efficacy of face mask ventilation during neonatal resuscitation and hopefully a reduction in the incidence of failed face mask resuscitation.
CONCLUSION
There was no significant difference in face mask leak between the Laerdal and Fisher & Paykel neonatal face masks when tested on a modified manikin. Specific techniques of face mask placement and hold reduced leak and were incorporated into educational strategies. There was a significant reduction in face mask leak following written instruction alone and a further reduction following demonstration. Further studies are required to determine whether these techniques prove effective in the delivery room.
What is already known on this topic
Leak at the face mask is large during PPV and may result in inadequate ventilation.
Operators are unable to reliably detect leak during PPV.
Techniques used to position and hold masks on the face are variable.
What this study adds
No difference in mask leak was demonstrated between two round face masks before or after technique training.
Teaching an improved technique significantly reduces leak at the face mask when tested with a modified manikin.
Acknowledgments
We thank the staff of the Royal Women’s Hospital Melbourne for their participation, and Fisher & Paykel Healthcare for providing samples of their neonatal resuscitation mask. Supported in part by a RWH Postgraduate degree scholarship (COFK) and a NHMRC Practitioner Fellowship (PGD); the Australian National Health and Medical Research Council Program Grant No 384100.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.