Article Text

Abstract
Objective To evaluate the effect of opioid analgesics, compared to placebo, no drug, or other non-opioid analgesics or sedatives, on pain, duration of mechanical ventilation, mortality, growth and neurodevelopmental outcomes in newborn infants on mechanical ventilation.
Methods This was a systematic review and meta-analysis of randomised controlled trials (RCTs). Data sources used were Cochrane, MEDLINE, EMBASE and CINAHL databases, and references from review articles. RCTs or quasi-RCTs comparing opioids to a control, or to other analgesics or sedatives in newborn infants on mechanical ventilation were reviewed.
Results A total of 13 studies on 1505 infants were included. Infants given opioids showed reduced Premature Infant Pain Profile (PIPP) scores compared to the control group (weighted mean difference (WMD) −1.71, 95% CI −3.18 to −0.24). Heterogeneity was significantly high in all analyses of pain. Meta-analyses of mortality, duration of mechanical ventilation and long-term and short-term neurodevelopmental outcomes showed no statistically significant differences. Very preterm infants given morphine took significantly longer to reach full enteral feeding than those in control groups (WMD 2.10 days, 95% CI 0.35 to 3.85). One study that compared morphine with midazolam showed similar pain scores, but fewer adverse effects with morphine.
Conclusions There is insufficient evidence to recommend routine use of opioids in mechanically ventilated newborns. Opioids should be used selectively, when indicated by clinical judgment and evaluation of pain indicators. If sedation is required, morphine is safer than midazolam.
Statistics from Altmetric.com
Introduction
Mechanical ventilation is used in neonatal intensive care units (NICUs) for treating pulmonary insufficiency in term and preterm newborns. Newborns delivered at <28 weeks gestational age (GA) are virtually all ventilated,1 and 27% of all infants admitted to NICUs undergo mechanical ventilation.2 Mechanical ventilation is potentially painful or uncomfortable,3 and pain is a stressful experience that may have consequences on the course of the acute illness and the infant's development. Pain and stress can interact negatively with mechanical ventilation, leading to unsynchronised breathing and suboptimal ventilation. Moreover, pain can cause clinical instability, leading to changes in heart rate, respiratory rate, intracranial pressure, blood pressure and oxygen saturation and to the development ofcomplications such as intraventricular haemorrhage (IVH).4
What is already known on this topic
▶. Newborns feel pain and stress during mechanical ventilation, and this could have short-term and long-term adverse consequences.
▶. Appropriate interventions for reducing pain should be applied to newborns in intensive care units.
What this study adds
▶. Routine administration of opioids is not effective in reducing pain during mechanical ventilation.
▶. Opioids should be used selectively based on clinical judgment and evaluation of pain indicators.
Reduction of pain in mechanically ventilated newborns is a critical part of supportive treatment.5,–,7 While sedation is routinely administered in intubated children and adults, there is considerable variability in the approach to neonates.8 9 Historically, the belief that newborns could not feel pain may have accounted, in part, for the low use of analgesics, as demonstrated by reports that some neonatologists are reluctant to use opioid analgesics2 and that opioids are underused in NICUs.4 10 11 Reluctance to use opioid analgesics is mainly due to an underestimation of pain in neonates.12 although appreciation of neonates' pain is increasing,13 14 but also due to fear of systemic, respiratory and cardiovascular effects and of drug dependency.13 A non-systematic review10 underlined the paucity of scientific evidence defining optimal drug regimens and describing adverse effects, but concluded that the latter are generally overestimated.
Recently, an aggressive approach to treatment and prevention of pain in the neonate has been recommended,15 16 but uncertainty remains about long-term effects of opioid use and about which opioid is most effective and safe.17,–,19 The benefits and risks of the use of opioids in the ventilated neonate have not yet been systematically reviewed. Therefore, this review was carried out to determine the effects of opioid analgesics in neonates (term or preterm) receiving mechanical ventilation for any respiratory disease. We evaluated randomised controlled studies that investigated the effects of opioids on pain, duration of mechanical ventilation, mortality, neurodevelopment and other parameters. The questions addressed by this review are: is an opioid better than placebo, a non-pharmacological treatment, or a non-opioid analgesic for reducing pain in mechanically ventilated newborns? Does opioid treatment reduce the incidence of neonatal mortality and abnormal neurodevelopment? Can the goal of treatment be accomplished without hampering cardiorespiratory functions, feeding and weight gain? These questions were addressed with a systematic review following the Cochrane Collaboration methodology.
Methods
We used the Cochrane Collaboration method and software (RevMan 4.2) and the Cochrane Neonatal Review Group guidelines (guidelines for reviewers and editors, available at: http://neonatal.cochrane.org/en/index.html) for systematic review and meta-analysis of RCTs and the QUORUM guidelines.
Data sources
We searched MEDLINE, EMBASE, CINAHL and the Cochrane Central Register of Controlled Trials for articles published between 1966 and June 2008. We used a combined text word and MeSH heading search strategy with the terms: infan*, neonat*, newborn*, morphine, diamorphine, fentanyl, alfentanil, sufentanil, pethidine, meperidine, codeine, methadone, narcotics and analgesia. References from identified articles were scanned to find other relevant studies. Moreover, we searched abstracts by hand from the Society for Paediatric Research and the European Society for Paediatric Research 1995–2007 and corresponded with expert informants in the areas of anaesthesia, paediatric surgery and neonatology. No language restriction was used and no attempts were made to identify unpublished studies.
Study selection
Reports identified by the literature search were screened for relevancy on the basis of title and abstract by all three reviewers. Then, the full texts of potentially relevant studies were evaluated by all reviewers and the decision to include each study was made by consensus.
We included randomised or quasi-RCTs that enrolled term (≥37 weeks GA), preterm (32–36 weeks) or very preterm (<32 weeks) infants on mechanical ventilation for any respiratory disease. Selected studies compared an opioid analgesic (administered at any dosage) to placebo, no intervention or another analgesic.
Validity assessment
Methodological quality of included trials was evaluated according to the guidelines of the Cochrane Neonatal Review Group. Weassessed quality regarding allocation concealment, blinding of carers and assessors to intervention, completeness of assessment of all randomised infants and blinding of assessors to outcome measurement. A ‘high quality’ study was defined as one in which allocation concealment was adequate.
Data extraction
Data on enrolment, treatment schedules, outcome measures, assessment scales and methodological quality were extracted independently by two reviewers (RB, KW); discrepancies were resolved by consensus, as recommended in the Cochrane Reviewer's Handbook.20 Further information was requested from the principal authors of the studies. For the purposes of this review, primary outcome measures were: pain, duration of mechanical ventilation, neonatal mortality (death within 28 days of life) or mortality to discharge and neurodevelopmental outcome and quality of life at short (≤1 year), medium (1–3 years) and long (>3 years) terms. Secondary outcomes were: incidence of bronchopulmonary dysplasia (need for oxygen at 28 days of life), chronic lung disease (need for oxygen at 36 weeks adjusted age); gastrointestinal complications; IVH, periventricular leukomalacia (PVL); hypotension requiring medical treatment (vasopressors or fluid boluses); days to reach full enteral feeding; breast versus bottle feeding at discharge; growth at term or near term (36–40 weeks adjusted age); and length of hospital stay.
On the basis of a critical review,21 the following scales were considered to be valid and reliable for use in newborn infants: the Neonatal Facial Coding System (NFCS),22 the Neonatal Infant Pain Scale (NIPS),23 and the Premature Infant Pain Profile (PIPP).24 We nonetheless included studies using other, non-validated scales.
Quantitative data synthesis
Outcomes were analysed using numbers of events rather than percentages of affected infants. For each outcome measure, we performed subgroup analyses regarding very preterm infants.
In the meta-analysis, treatment effects of categorical variables were analysed using RR, risk difference (RD) and number needed to treat, each with 95% CI; treatment effects of continuous variables were analysed using weighted mean difference (WMD). When different scales were used to measure pain, standardised mean difference (SMD)was calculated (data are, therefore, expressed as units of SD). Data from crossover trials were extracted and analysed as parallel groups. A fixed effects model for meta-analysis was used if heterogeneity allowed (p>0.10 on χ2 or analysis of variance (ANOVA) test), otherwise, a random effects model was used. Heterogeneity between trial results was examined using a χ2 test for dichotomous outcomes or ANOVA for continuous outcomes.
Results
Overview of included studies
The literature search identified 16 potentially relevant studies, of which 3 were excluded because they compared 1 opioid to another25,–,27 (figure 1). Thus, 13 studies described in 21 reports were eligible for review28,–,47 (table 1). Two studies have been published only in abstract form.37 47 Three studies focused on very preterm infants.28 29 35

Selection process for study inclusion.
Description of studies included in review
The majority of studies compared one opioid (morphine, meperidine, alfentanil, fentanyl) to placebo; one study compared fentanyl to no intervention,36 and another compared morphine to the muscle relaxant pancuronium and to the combination morphine+pancuronium.41 Regarding this latter study, we considered data regarding morphine+pancuronium versus pancuronium alone. Two of the studies focused on the effects of treatment during routine handling or interventions (endotracheal suction).
Study quality
The overall methodological quality of the studies was fair to good according to the guidelines of the Cochrane Neonatal Review Group. Randomisation and allocation concealment were adequate in seven studies,28 29 34 38 39 42 44 termed ‘high quality’ studies. In four studies35 36 41 43 randomisation was performed by drawing sealed envelopes, yet no details were given about how the randomisation list was generated or how allocation concealment was ensured. Finally, in the two abstracts,37 47 randomisation was performed by drawing sealed envelopes (P Lago and J Siwiec, personal communications)but adequacy of allocation concealment was not specified.
Blinding of carers and assessors to intervention was obtained in most studies. Blinding of interventions and outcomes was not guaranteed in Quinn et al;41 in the two studies published as abstracts, blinding was not performed by Siwiec et al (personal communication)47 and blinding of carers was not performed in Lago et al.36 A note of caution is required since in most studies the carers could have been more aware of the effects of pain control than stated.
Follow-up was almost complete for all studies. In the NEOPAIN study,29 30 of 391 infants surviving at 28 days in morphine group and 43 of 402 in placebo group did not undergo cranial ultrasonography at 4–7 or 28–35 days. In the report with long-term follow-up,40 8.4% of the surviving patients were lost at 5–6 years.
Opioid effects on pain
Overall, nine studies reported pain as an outcome measure and for two studies29 38 we obtained unpublished pain scores from the authors. Validated behavioural pain scales were used in five studies, of which three28 29 47 found significant results in favour of opioid (morphine). This significant difference was not present at every time point, for example, the NEOPAIN study29 found a significant difference 24 but not 72 h after starting treatment.
Four studies used PIPP to evaluate pain (figure 2).28 29 44 47 When PIPP scores were pooled across these studies, considerable heterogeneity was found (χ2=24.76, p<0.0001). Meta-analysis (random effects model) showed that PIPP scores were reduced in infants treated with opioid (in all cases, morphine) compared to controls (WMD −1.71, 95% CI −3.18 to −0.24). When only high quality studies were considered,28 29 44 heterogeneity persisted but the pain reduction in favour of opioid treatment was no longer significant (WMD −1.51, 95% CI −3.17 to 0.14). In meta-analysis of studies of very preterm infants,28 29 no significant effect of morphine versus placebo was found (WMD −2.68, 95% CI −6.62 to 1.27). Other well validated pain scales were used by two studies. Guinsburg et al35 administered fentanyl or placebo in a single dose and then measured pain at 30 and 60 min using a modified NFCS. Pain scores were significantly lower compared to placebo only when assessed from video recordings but not when assessed at bedside (WMD 0.19, 95% CI −1.15 to 1.53). Simons et al44 used the NIPS to evaluate infants before, during and after endotracheal suctioning and found no significant effect of morphine versus placebo (WMD −0.19, 95% CI −0.72 to 0.34).

Meta-analysis for primary outcome (pain measured with Premature Infant Pain Profile (PIPP) scale).
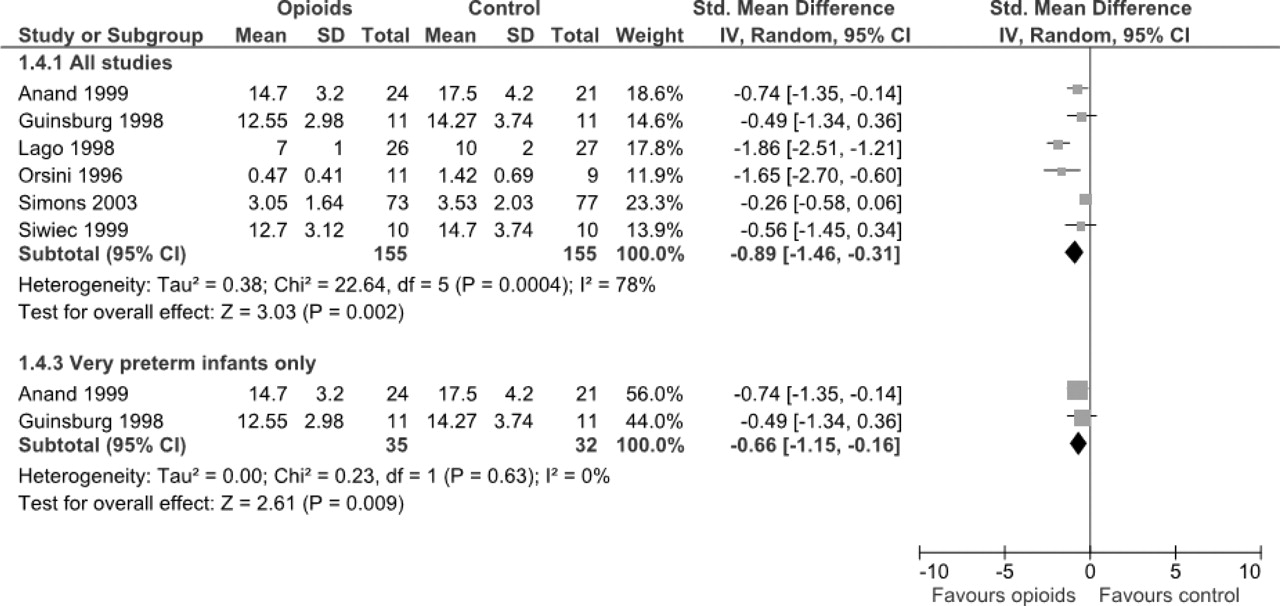
A total of 9 different non-validated pain scores were used in 10 studies. Three studies found a significant difference in favour of the opioid group;36 38 39 this positive effect of opioids was also observed by Saarenmaa et al at the higher dose of alfentanil,43 by Guinsberg et al35 when video recordings of infants were analysed and by Lago et al.37 In contrast, four studies found no significant difference between opioid and control treatments. Results from six studies could be pooled in meta-analysis using a random effects model (figure 3) and a significant effect was found in favour of the opioid group: SMD was −0.89 (95% CI −1.46 to −0.31), that is, there was a pooled difference of 0.89 units of SD. In the subgroup analysis of studies on very preterm infants,28 35 a significant effect in favour of opioids was found (random effects model: SMD −0.66, 95% CI −1.15 to −0.16). This meta-analysis of should nonetheless be interpreted with caution because of inconsistencies in the types and doses of opioids used, outcome measures recorded and statistical analyses.

Meta-analysis for primary outcome (pain measured with other scales).
Opioid effects on other primary outcome measures
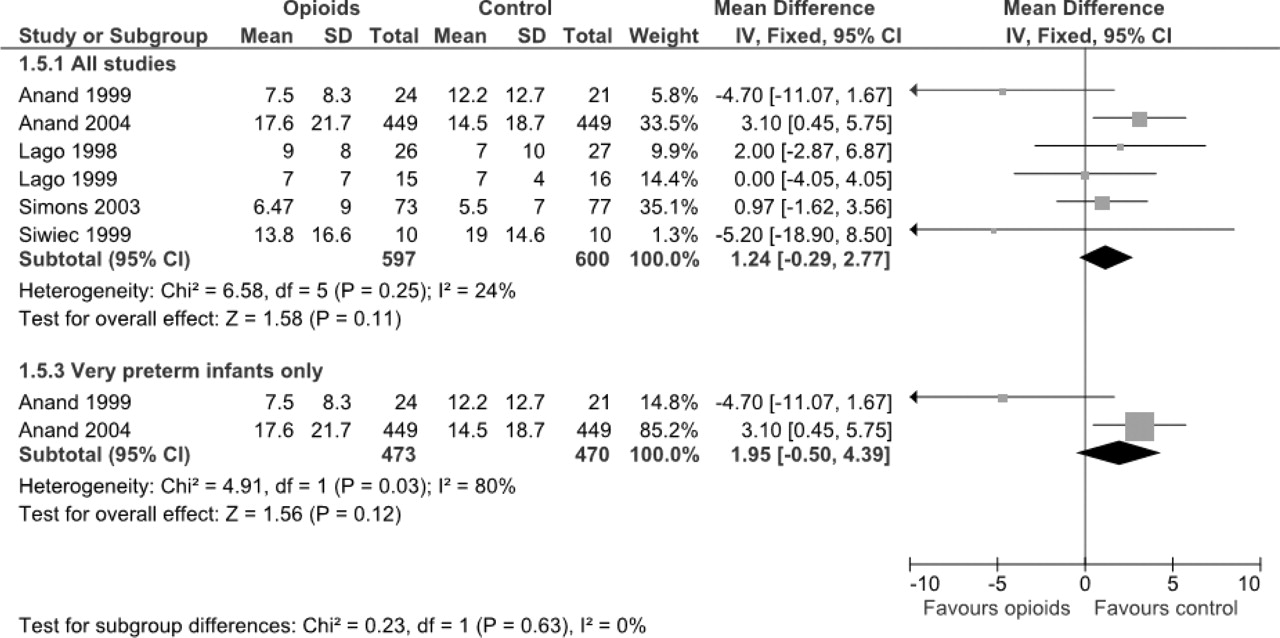
In all, 10 studies reported the duration of ventilation during treatment and only 129 found a significant difference between opioid and control groups (p=0.0338). Three studies34 41 42 were not included in meta-analysis because they presented this outcome as a median and range. Orsini et al38 reported no significant difference in duration of ventilator use between fentanyl and placebo groups, but no data were available for analysis. Meta-analysis of six studies (figure 4) showed no significant effect (WMD 1.24 days, 95% CI −0.29 to 2.77); there was minor evidence of heterogeneity (χ2=6.58; p=0.25). Meta-analysis of results from studies on very preterm infants28 29 revealed no significant difference between morphine and placebo (WMD 1.95 days, 95% CI −0.50 to 4.39).
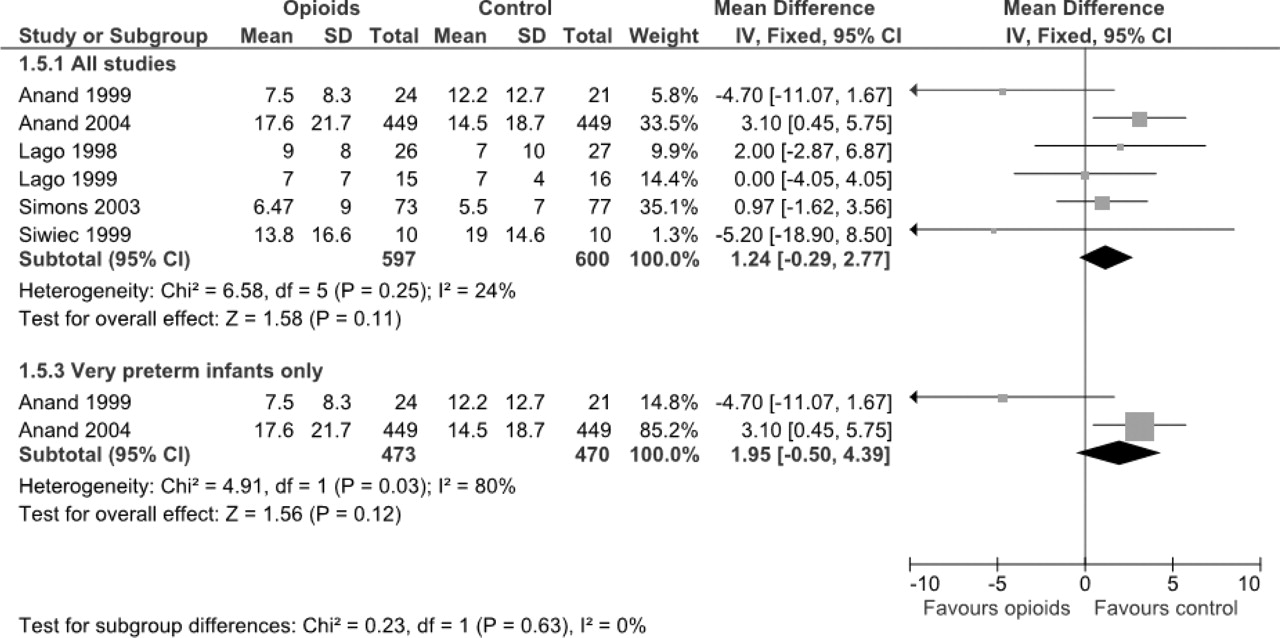
Meta-analysis of primary outcome (duration of ventilation).
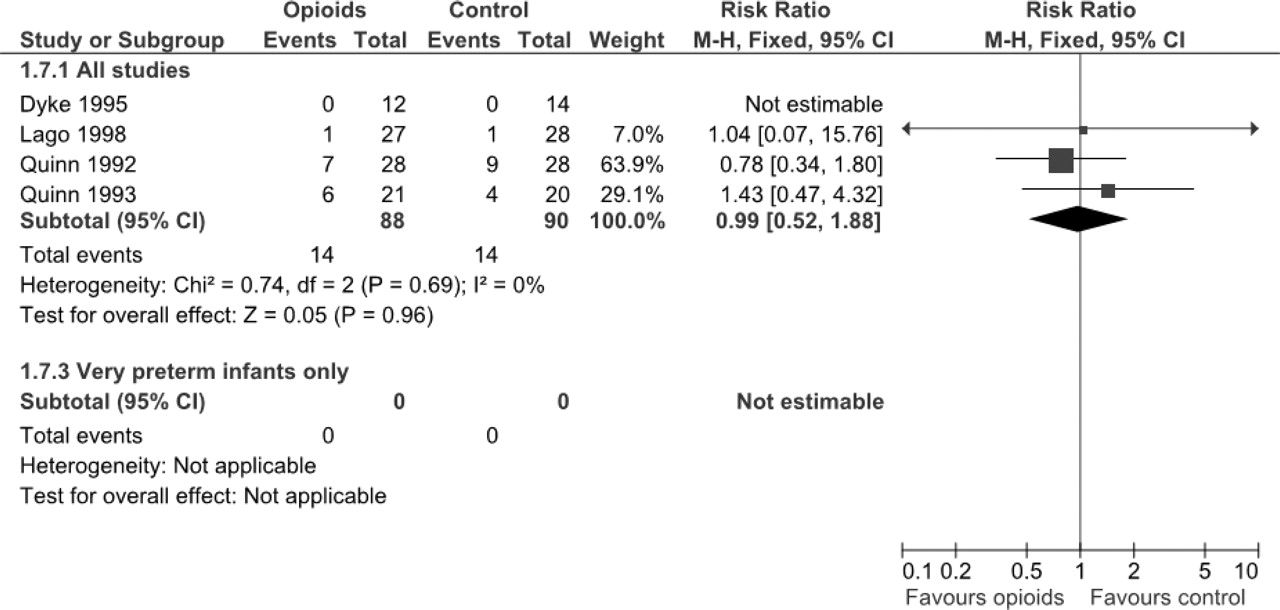
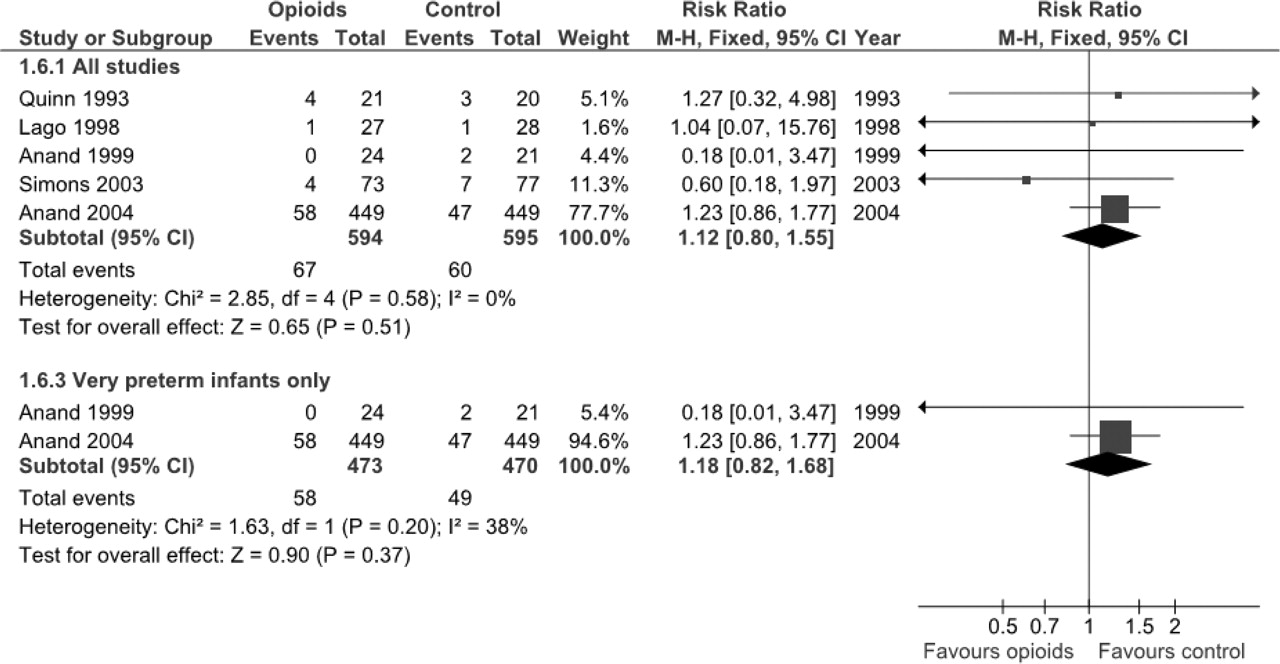
Seven studies reported the effect of treatment on neonatal mortality and none found any significant difference between opioid and placebo or no treatment groups. Meta-analysis was possible for five trials28 29 36 42 44 (figure 5) and showed no significant effect: RR of mortality was 1.12 (95% CI 0.80 to 1.55); RD of mortality was 0.01 (95% CI −0.02 to 0.05); these results did not change when only high quality studies were analysed. At subgroup analysis of very preterm infants,28 29 RR was 1.18 (95% CI 0.82 to 1.68), RD 0.03 (95% CI −0.02 to 0.06). Meta-analysis of four trials that reported on mortality to discharge34 36 41 42 showed no significant effect of opioid treatment: RR 0.99 (95% CI 0.52 to 1.88), RD −0.001 (95% CI −0.11 to 0.10) (figure 6)
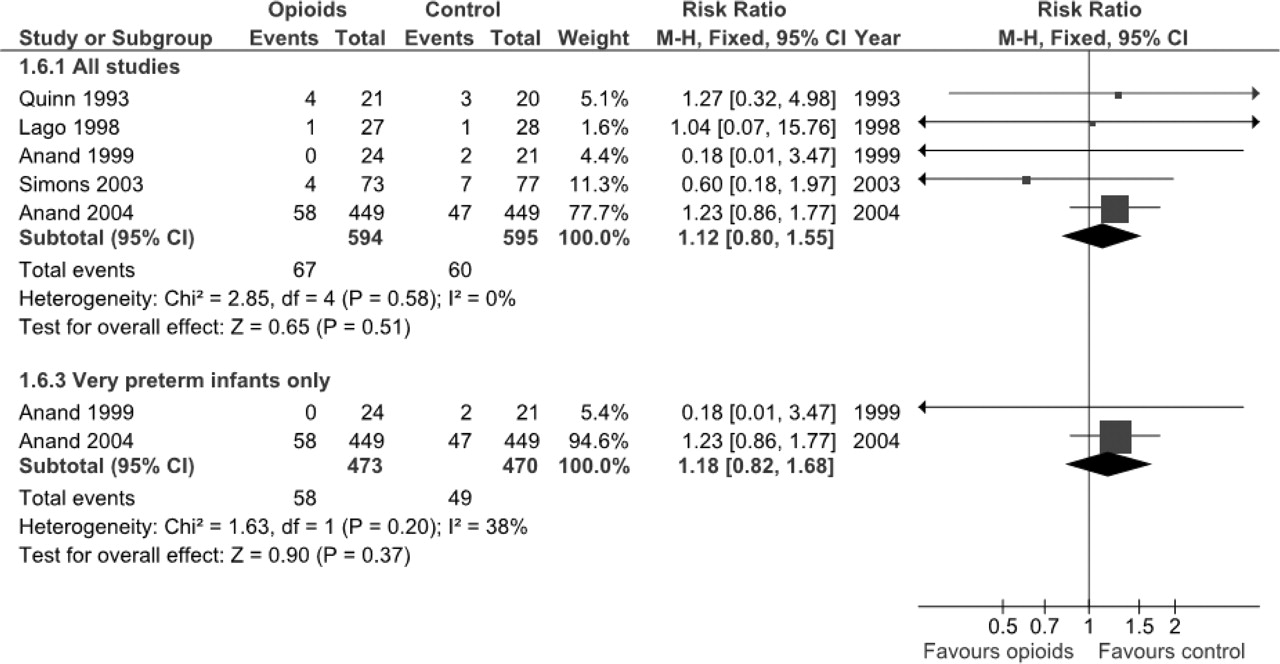
Meta-analysis of primary outcome (neonatal mortality).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of primary outcome (mortality to discharge).
Neurodevelopmental outcomes were reported in two studies. Anand et al28 assessed neurodevelopmental outcome at 36 weeks corrected age using the neurobehavioural assessment of the premature infant (NAPI) examination cluster scores. After adjusting for differences in Neonatal Medical Index and GA, these authors found no significant differences in NAPI scores; mean (SD) values were 58.8 (20.0) in morphine group versus 55.7 (22.4) in placebo group. MacGregor et al assessed the neurodevelopment of infants aged 5–6 years who had been recruited in neonatal period by two sequential studies.40 Of the 136 recruited infants, 95 survived and 87 of these were assessed using Wechsler Preschool and Primary Scale of Intelligence – Revised (WPPSI-R), Movement ABC and Child Behavior Checklist. There was no significant difference in disability at age 5–6 years between morphine and non-morphine groups (RR 1.46, 95% CI 0.51 to 4.24; RD 0.06, 95% CI −0.09 to 0.20), nor were there significant differences in intelligence (point estimate 2.0, 95% CI −6.0 to 11.0), motor impairment (point estimate −2.0, 95% CI −5.5 to 2.0) and behavioural problems (point estimate −3.0, 95% CI −12 to 3). Furthermore, there was no significant difference in combined death and disability rates between morphine and non-morphine groups for the 136 children in the original cohorts. Calculations that assumed that outcomes on the missing newborns favoured the morphine or non-morphine group did not alter the conclusion of no significant effect on death or disability.
Opioid effects on secondary outcome measures
We considered as secondary outcome measures the incidence of bronchopulmonary dysplasia (defined as oxygen need at 28 days of life), chronic lung disease (oxygen need at 36 weeks postconceptional age), gastrointestinal complications, IVH and PVL; hypotension requiring medical treatment; days to reach full enteral feeding; growth (weight gain); and days of hospitalisation. Results are reported in table 2.
Secondary outcomes of the systematic review and meta-analysis
Four studies34 36 37 44 investigated the incidence of bronchopulmonary dysplasia (oxygen at 28 days) and reported no significant effect of treatment (RR 1.19, 95% CI 0.73 to 1.92; RD 0.03, 95% CI −0.06 to 0.13).
Three studies29 38 47 reported on the incidence of chronic lung disease (oxygen at 36 weeks postmenstrual age) and again found no significant effect of treatment (RR 0.95, 95% CI 0.73 to 1.22; RD −0.01, 95% CI −0.07 to 0.04). Only one study29 reported on very preterm infants: no significant effect was found (RR 1.02, 95% CI 0.78 to 1.32; RD 0.001, 95% CI −0.05 to 0.06).
Among gastrointestinal complications, the incidence of necrotising enterocolitis was reported in two studies,36 44 without significant differences between opioid and control groups. Meta-analysis confirmed no significant effect (RR 0.93, 95% CI 0.36 to 2.37; RD −0.01, 95% CI −0.08 to 0.07). The incidence of IVH was distinguished according to Papile grade. Six studies reported on incidence of all grades of IVH.28 34 38 41 42 44 Only Simons et al44 found a significant reduction in IVH incidence in favour of the morphine group, with RR 0.58 (95% CI 0.35 to 0.95). Meta-analysis of all six studies revealed no significant effect (RR 0.84, 95% CI 0.60 to 1.17; RD −0.05, 95% CI −0.14 to 0.04). The study that considered very preterm infants only28 found no significant effect (RR 0.66, 95% CI 0.17 to 2.60; RD −0.07, 95% CI −0.28 to 0.15).
Incidence of severe IVH (Papile grade III or IV) was reported in five trials,28 29 36 44 47 none of which found a significant difference. Lack of significant effect of opioid on this parameter was confirmed at meta-analysis of all five studies (RR 0.98, 95% CI 0.70 to 1.38; RD −0.00, 95% CI −0.04 to 0.03) and of studies with very preterm infants only28 29 (RR 1.12, 95% CI 0.78 to 1.60; RD 0.01, 95% CI −0.03 to 0.05); meta-analysis showed only minor heterogeneity. The NEOPAIN group29 did a post hoc analysis of participants who did not require additional morphine analgesia and found a significantly increased risk of developing severe IVH in the morphine-treated infants compared to controls. When the meta-analyses were repeated with data from this post hoc analysis, the results were not different and significance was not reached (data not shown).
Regarding the incidence of PVL, none of five studies28 29 36 44 47 reporting this outcome measure found a significant difference between opioid and control groups. This finding was confirmed at meta-analysis of all studies (RR 0.79, 95% CI 0.51 to 1.22; RD −0.02, 95% CI −0.04 to 0.01) and studies of very preterm babies only (RR 0.80, 95% CI 0.49 to 1.29; RD −0.02, 95% CI −0.05 to 0.02);28 29 heterogeneity was not a confounding factor. Reanalysis of studies of very preterm babies also revealed no significant effect (data not shown).
Three studies reported incidence of hypotension requiring medical treatment.29 42 44 Significant heterogeneity exists between studies. The random effect meta-analyses showed no significant effect between opioids and placebo. The NEOPAIN study29 considered only very preterm infants and reported a higher incidence of hypotension requiring medical intervention in morphine group (RR 1.63, 95% CI 1.25 to 2.11; RD 0.10, 95% CI 0.05 to 0.15).
Four studies considered the number of days to full enteral feeding. While there was no significant difference between opioid group and placebo or no treatment group in three studies,28 36 37 morphine-treated neonates in the NEOPAIN study29 took longer than those receiving placebo to tolerate full volume nasogastric feeding (p=0.04). Meta-analysis of the four studies showed a borderline significant effect (WMD 1.43 days, 95% CI −0.01 to 2.87; p=0.05), while that of two studies dealing with very preterm infants28 29 found a significant effect in favour of control treatment (WMD 2.10 days, 95% CI 0.35 to 3.85).
Anand et al28 reported no significant effect of opioid treatment on weight gain at 36–40 weeks postconceptional age, but the data were not available for analysis. Lago et al36 found no significant difference in the number of days needed for ‘growth to birth weight’ (days to recover birth weight)between the fentanyl group (mean 12, SD 7 days) and the no-treatment group (mean 15, SD 5 days). Anand et al28 investigated daily weight gain adjusted for birth weight up to discharge in an analysis of covariance model and reported a significant difference 28 days after birth but not at discharge; mean (SD) values for morphine versus placebo groups were 1.26 (0.152) versus 1.15 (0.146) g/kg day (p=0.04) at day 28 and 1.78 (0.716) versus 1.96 (0.837) g/kg day at discharge (p=not specified).
Four studies reported on length of hospital stay28 34 36 37 but the results from Dyke et al34 were not suited for meta-analysis because they were presented as median and range. No study found a significant difference between opioid and control groups. In meta-analysis of three trials, no significant effect was found (WMD 1.80 days, 95% CI −7.03 to 10.62).
Discussion
Pain control in ventilated newborns is a debated issue in neonatology.17 18 Previous review conducted with unreported methods48 yielded mixed results.
This systematic review of data from 1519 newborn infants studied in 13 controlled trials assessed evidence supporting opioid use during mechanical ventilation following Cochrane Collaboration methodology.
One of the primary outcomes of this review, infants' pain, was evaluated in 11 studies, using well validated, or less well validated scales. When pain was assessed on a validated scale such as PIPP, the WMD of 1.71 points was statistically significant in favour of opioid treatment, but this difference is not clinically significant. Marked statistical heterogeneity was found in this analysis. Heterogeneity can be caused by a small number of participants, as in the study by Anand et al,28 and by methodological differences in measuring PIPP score. Only the abstract by Siwiec et al47 evaluated PIPP score in unstipulated infants: PIPP score was <6 in morphine group, indicating minimal pain.17 In the other studies, which measured PIPP during endotracheal suctioning,39 43 morphine treatment did not reduce PIPP score below 7.9 (ie, incomplete control of pain).
Heterogeneity was significantly high in all the analyses involving pain. Exclusion of lower quality studies or limitation to very preterm infants did not diminish the heterogeneity. Although causes of heterogeneity were not formally studied in a post hoc analysis, possible explanations are inconsistencies in the opioids used and differences in dosages, outcome measures and statistical reporting. The ‘extra protocol’ use of opioids in more recent studies29 44 may have diluted the effect of the intervention being studied. However, this observation suggests that opioids are now widely accepted for use in NICU and that it is considered unethical not to give newborns the analgesic relief they need, if clinically justified.
Most studies evaluated the effect of an opioid started at the beginning of mechanical ventilation, assuming that mechanical ventilation is a painful procedure. The overall effect of opioids in this setting was found to be small and quite inconsistent. Given the pharmacological characteristics of opioids, possible explanations for this finding are numerous: pain could not have been measured correctly or newborns on mechanical ventilation may not always feel pain. The effect of opioids given ‘on demand’ in studies that allowed for extra protocol opioid administration could have altered the measurements of pain. Non-drug interventions that were not mentioned in the papers could reduce pain and stress in newborns on the ventilator, thus reducing the need for drug control of pain. Indeed, infants in one recent study44 had low pain scores, so the lack of effect of opioids might be expected.
We had anticipated that this review would reveal the effects of opioids when administered on an ‘as needed’ basis according to signs of pain. This issuewas addressed only by Lago et al,36 who observed a significant reduction of pain when fentanyl was titrated (administered in proportion to need) according to a behavioural assessment of each infant's pain. However, interpretation of these results is limited by the fact that this trial enrolled only 55 infants and did not use a well validated pain scale.
Among primary outcomes of the review, opioid use did not have major adverse effects on infants regarding mortality and duration of ventilation. For another important primary outcome, medium-term and long-term neurodevelopment, only limited data from one study were available. Considering that opioids could influence neurological outcomes either positively (reducing the adverse effects of pain) or negatively (interfering with neurotransmitters), there is urgent need for data addressing this subject, specifically for very preterm and vulnerable infants. These data could come in a few years' time from follow-up studies of the two recent, larger clinical trials.29 44
With regard to other secondary outcomes, no significant effects were found, with the exception of an increase in days to reach full enteral feeding. These results were found to be consistent across studies and meta-analysis yielded valid estimates of effects.
The subgroup analysis of the effects of opioids in very preterm babies yielded similar results, with a small reduction of pain scores; clinical adverse effects were noticed for days to reach full enteral feeding and hypotension. The finding of more frequent hypotension in very preterm newborns deserves attention, as the consequence on systemic and cerebral circulation could leads to adverse neurological outcome. A note of caution came in fact from two studies28 29 that showed a tendency toward more frequent hypotension requiring medical intervention and adverse neurological effects for higher opioid doses in smaller babies. It is worth noting that all the studies reporting hypotension as an outcome used morphine as intervention; no comparison with fentanyl is thus possible in this review. No data were available on the effects of opioids on cerebral and systemic blood flow.
Finally, different dosage regimens were used across studies but no clear relationship with effect was found.
Conclusions and future research
This systematic review found insufficient evidence to recommend routine use of opioids in mechanically ventilated newborns. In the absence of firm evidence to support a routine policy, we suggest that opioids be used selectively based on clinical judgment and evaluation of pain indicators, even though there are limitations to pain measurement in newborns. This issue should be further investigated in large, well conducted studies. Future studies should enrol only newborns who express pain (assessed on validated scores) when on mechanical ventilation and should evaluate the administration of opioids on an ‘as needed’ basis according to signs of pain. Data are specifically needed for very preterm babies. In this group of newborns more data are needed to clarify the haemodynamic effects of opioids (in particular morphine); cerebral and system blood flow should be investigated to investigate the mechanisms of adverse effects such as IVH and lower tolerance to feeding. Medium-term and long-term neurodevelopmental consequences of opioid treatment have not been adequately addressed to date, so follow-up investigations of the patients enrolled in these trials are valuable.
Acknowledgments
We thank PG Duca, Department of Statistics, University of Milan, for statistical advice, V Castagna for help in document retrieval and V Matarese for editorial advice.
References
Footnotes
-
Ethics approval Not required.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
This paper is based on a Cochrane review published in The Cochrane Library 2008, Issue 1. Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback and The Cochrane Library should be consulted for the most recent version of the review.