Article Text

Abstract
Objective To evaluate the incidence and severity of nasal trauma secondary to nasal continuous positive airway pressure (nCPAP) in neonates.
Design Prospective observational study.
Setting Neonatal intensive care unit (NICU) of the University Hospital of Lausanne, Switzerland.
Patients All neonates admitted between January 2002 and December 2007 treated by nCPAP were eligible.
Methods Patients' noses were monitored during nCPAP. Nasal trauma was reported into three stages: (I) persistent erythema; (II) superficial ulceration; and (III) necrosis.
Results 989 neonates were enrolled. Mean gestational age was 34 weeks (SD 4), mean birth weight 2142 g (SD 840). Nasal trauma was reported in 420 (42.5%) patients and it was of stage I, II and III in 371 (88.3%), 46 (11%) and 3 (0.7%) patients, respectively. Incidence and severity of trauma were inversely correlated with gestational age and birth weight. The risk of nasal trauma was greater in neonates <32 weeks of gestational age (OR 2.48, 95% CI 1.59 to 3.86), weighing <1500 g at birth (OR 2.28, 95% CI 1.43 to 3.64), treated >5 days by nCPAP (OR 5.36, 95% CI 3.82 to 7.52), or staying >14 days in the NICU (OR 1.67, 95% CI 1.22 to 2.28). Most cases of nasal trauma (90%) appeared during the first 6 days of nCPAP. Persistent visible scars were present in two cases.
Conclusions Nasal trauma is a frequent complication of nCPAP, especially in preterm neonates, but long-term cosmetic sequelae are very rare. This study provides a description of nasal trauma and proposes a simple staging system. This could serve as a basis to develop strategies of prevention and treatment of this iatrogenic event.
Statistics from Altmetric.com
Introduction
Continuous positive airway pressure (CPAP) administered by nasal devices (nCPAP) is widely used in the respiratory management of newborn infants.1,–,5 Although complications such as gastric distension and air leaks are well described, there is little documentation of nasal trauma, another common side effect.6
The local pressure of CPAP devices to the nasal area tends to develop decubitus lesions in the newborn due to its cutaneous vulnerability and anatomical factors such as end-vascularisation of the columella and nostrils.7 Nasal trauma represent a source of discomfort for patients, possible site of infection and a risk of long term functional or cosmetic sequelae.8,–,10 There is few and heterogeneous data in the literature on this topic.11,–,16 Robertson et al first reported a rate of 20% for nasal deformities secondary to nCPAP in very low birthweight infants (7 cases).11 Nasal trauma have been described in case reports.12 13 Yong et al have studied the effect of mask versus cannula in the development of nasal trauma and found no statistically significant difference between these two devices (29% vs 35%, respectively).14 Other studies comparing different nCPAP systems reported this complication as a secondary outcome.15 16 Furthermore, nomenclature of these nasal lesions is highly variable including nasal trauma, injury, breakdown, blanching, bleeding or necrosis. The aims of this prospective observational study were to evaluate incidence, severity and risk factors for nasal trauma due to nCPAP. We did so using an adapted classification system derived from the decubitus ulcer literature.17 18
What is already known on this topic
▶ Nasal continuous positive airway pressure (nCPAP) is used frequently in the management of neonatal respiratory distress.
▶ Nasal trauma is a recognised complication of nCPAP but its extent has not been well described.
What this study adds
▶ Nasal continuous positive airway pressure (nCPAP) frequently causes nasal trauma in neonates; erythema is most common, but erosion or necrosis occasionally occur.
▶ We propose a standardised system to classify nasal trauma associated with nCPAP.
Patients and methods
Setting and patients
All patients admitted between January 2002 and December 2007 in the neonatal intensive care unit (NICU) of the University Hospital of Lausanne, Switzerland, were considered as eligible. Our tertiary centre covers a region with approximately 14 000 deliveries per year. The NICU has 30 beds and we care for 500–600 neonates per annum including 120–140 newborns weighing <1500 g. Inclusion criterion was nCPAP treatment. Exclusion criteria were nCPAP treatment duration <24 h, pre-existing nasal lesions secondary to naso-tracheal intubation, upper airway malformations or patients referred from other centres after more than 24 h of nCPAP treatment. All newborn infants included in the study were prospectively observed to detect nasal trauma from the first day of nCPAP treatment until its weaning. If a nasal lesion persisted at the time of discharge, an ambulatory follow-up by the plastic paediatric surgeon (JH) was organised.
This study was integrated in the iatrogenic events recording programme of our NICU, which is part of the quality improvement plan coordinated by the Paediatric Department of the Hospital. The collection and use of the data was authorised by the Federal Expert Committee on Professional Disclosure in Medical Research within the framework of the Data Protection Law.
Applications and modalities of nCPAP
Standard policy in our NICU is to promote the routine use of nCPAP within minutes after birth for all newborns with respiratory distress of various aetiologies. Pressure of 5 cm H2O is maintained and oxygen is adjusted to keep PaO2 >50 mm Hg. Nasal intubation and mechanical ventilation are considered when nCPAP is not sufficient to achieve a satisfactory PaO2 while breathing 80–100% O2 and lower the PaCO2 <65 mm Hg, or to relieve marked retractions or frequent apnoeas. Weaning nCPAP is considered when the tachypnoea and retractions become minimal or have disappeared, and when there is no longer need for supplemental oxygen. Nasal CPAP is reintroduced when the infant has tachypnoea >70/min, deep retractions or frequent episodes of apnoea and bradycardia.
Throughout the study period, the same nCPAP system was used (Infant Flow Driver system, Hamilton Medical, Bonaduz, Switzerland). Nasal prongs and masks were used alternatively, in every patient, switching the devices every 4–6 h. Their size was adapted to the nose and nostrils and they were fixed to a fitted hat with Velcro moustaches (figure 1A,B). Infants were positioned supine, prone or on their sides. Nursing care of all infants under nCPAP included gentle massages, without any ointment, of pressure points of nasal devices every 2–4 h. When a nasal trauma appeared, an ointment (dexpanthenolum) was applied with massages and paracetamol was given in the presence of elevated pain scores. In case of persisting trauma or increase in severity of the trauma, a hydrocolloid film (Varihesive) was placed between pressure points and nCPAP devices. These practices were not considered as interventional since they were already in place for all patients under nCPAP before the onset of the study and were applied during the entire study period. Nurses and medical staff were trained for careful observation of the nose every 30–60 min during nCPAP treatment, which was removed every 2–4 h to allow closer local inspection. This inspection was external and not instrumented, so it is possible that isolated internal trauma of the nostrils was missed.

Examples of nCPAP prongs (A) and mask (B) fixation.
Description and classification of nasal trauma
There is currently no recognised classification available to describe the severity of nasal trauma secondary to nCPAP in neonates. We therefore classified trauma based on the standardised classification of the decubitus lesions from the US National Pressure Ulcer Advisory Panel (NPUAP).17 18
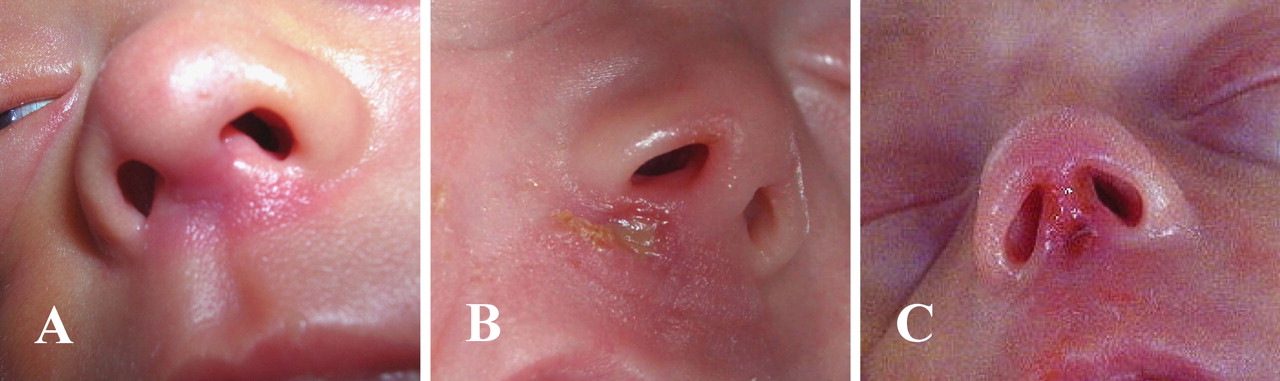
▶ Stage I: erythema not blanching, on an otherwise intact skin (figure 2A)
▶ Stage II: superficial ulcer or erosion, with partial thickness skin loss (figure 2B)
▶ Stage III: necrosis, with full thickness skin loss (figure 2C).

Classification of nasal trauma. (A) stage I (non-blanching erythema), (B) stage II (superficial erosion), (C) stage III (necrosis of full thickness of skin).
When a patient presented a nasal trauma evolving through different stages, only the most severe stage was considered.
Data
Administrative, demographical, clinical and respiratory data were anonymously registered and computerised.
Every nasal trauma secondary to nCPAP was always reported using a specific form indicating the date of occurrence, severity of trauma, its evolution and possible treatment. Reports were later reviewed and collated by one research nurse (CS-D).
Statistical analyses
We analysed the results with the SPSS V.15.0 for Windows. Univariate analyses of variance were performed for comparisons between groups. χ2 Tests were used for frequencies, with two by two comparisons in a second step and post-hoc tests (Tukey) for comparison of variables two by two. Correlation analysis and logistic regressions were also performed. The threshold for significance was p<0.05.
Results
Among the 2987 infants admitted in our NICU during the study period, 1529 were treated by nCPAP (51.2%). Exclusion criteria were present in 396 patients (250 treated by nCPAP <24 h, 105 with pre-existing nasal lesion secondary to nasal intubation, two with upper airway malformations and 39 referred from another unit after >24 h of nCPAP). During follow-up, 144 patients were lost (101 transferred to another unit while still under nCPAP and 43 died). In total, 989 patients were finally included and observed during 13 719 days of nCPAP treatment.
Population characteristics
Table 1 shows demographical and neonatal characteristics of the study population and table 2 the main indications for nCPAP treatment. As the population displayed a normal distribution, only mean values are shown in the tables.
Demographic and clinical characteristics (n = 989)
Primary indications for nasal continuous positive airway pressure
Incidence and severity of nasal trauma
Among the 989 patients included, 420 (42.5%) developed a nasal trauma. According to our classification, there were 371 (88.3%) cases of stage I nasal trauma, 46 (11%) of stage II and 3 (0.7%) of stage III. This corresponds to a general incidence of 30.6 cases of nasal trauma/1000 days of nCPAP, respectively 27.1 cases of stage I/1000 days of nCPAP and 3.5 cases of stages II–III/1000 days of nCPAP. For statistical analyses, the three patients who developed stage III were grouped with stage II.
Table 3 describes characteristics of subgroups of patients, depending on their outcome and two by two comparisons.
Patient characteristics according to severity of nasal trauma (n = 989)
Frequency and severity of nasal trauma stratified for different gestational age and birthweight categories are shown in table 4.
Frequency and severity of nasal trauma among gestational age and birthweight categories (n = 989)
Nasal trauma due to nCPAP developed in 90% of the patients <28 weeks of gestation and in 77% of those <32 weeks of gestation, compared to 28% of those ≥32 weeks of gestation and 11% of term neonates. A similar distribution was found when comparing the frequency in different birth weight categories. Frequency of nasal trauma in infants <26 weeks and weighing <750 g was not greater than when compared to infants of 26–28 weeks and of birth weights of 750–1000 g (data not shown).
Correlation analyses confirmed that gestational age and birth weight inversely correlated with the severity of nasal trauma (respectively −0.477 and −0.441; p<0.001). Partial correlations showed that, when birth weight was controlled, gestational age correlated at −0.209 (p<0.001). On the contrary, when gestational age was controlled, birth weight correlated at −0.060 (NS).
Logistic regression showed that the relative risk for development of nasal trauma was significantly increased when gestational age was <32 weeks (OR 2.48, 95% CI 1.59 to 3.86), birth weight <1500 g (OR 2.28, 95% CI 1.43 to 3.64), nCPAP duration >5 days (OR 5.36, 95% CI 3.82 to 7.52) and NICU duration >14 days (OR 1.67, 95% CI 1.22 to 2.28). Cut-offs for risk comparisons by gestational age and birth weight were a priori chosen based on existing categories of newborn infants in outcome studies. Cut-offs for risk comparisons with regards to durations of nCPAP treatment and NICU stay were decided after post-hoc analyses. All these factors represented a significant risk for the development of nasal trauma (p≤0.001), however they were not significant for the risk of progression of a stage I into a more severe stage (II or III). Nasal intubation did not appear to be a significant risk factor for subsequent development of nasal trauma under nCPAP (OR 1.16, 95% CI 0.76 to 1.77).
Onset of nasal trauma
Figure 3 shows the timing of the onset of the nasal trauma in the course of nCPAP treatment.
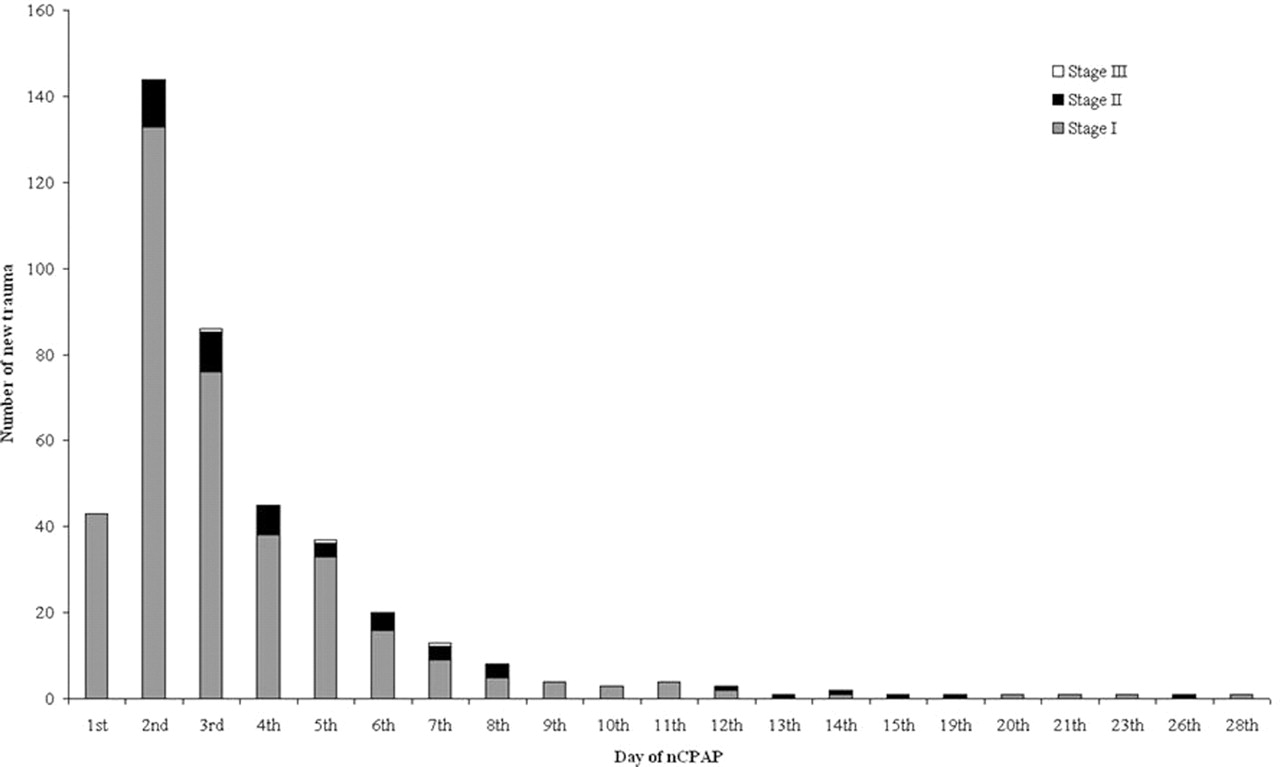
Onset of nasal trauma during the nCPAP treatment.
Mean time interval between the application of nCPAP and the onset of nasal trauma was 2.7 days (SD 3.3; range 0–27). The mode corresponded to the median on the second day and the 90th percentile on the sixth day of nCPAP treatment. Stage I trauma appeared earlier after a mean of 2.5 days of nCPAP (SD 3.3; range 0–27) and stage II–III after a mean of 4.5 days (SD 4.8, range 1–25).
Evolution of nasal trauma
Stage II nasal trauma was preceded by stage I in 36/46 (78.3%) of cases, whereas 371/407 (91.1%) stage I nasal trauma did not progress into stage II or III. Two cases of the 46 stage II (4.3%) evolved into stage III. Specific measures included application of a hydrocolloid film in 21/420 (5%) patients with nasal trauma. No nCPAP had to be discontinued and no infant had to be intubated because of nasal trauma.
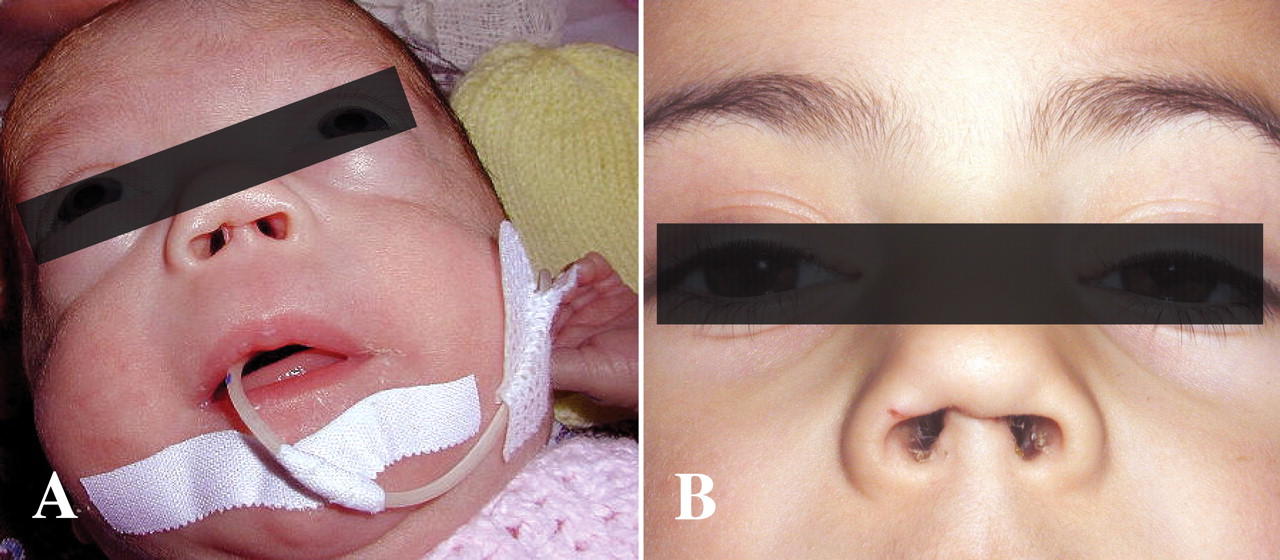
Healing at the time of nCPAP weaning was observed in all stages I and II nasal trauma. The three patients with stage III trauma presented a scar at the time of hospital discharge and were therefore followed up by our paediatric plastic surgeon (JH). In one patient the scar was attenuated. The other two patients are likely to require cosmetic surgery later (figure 4A,B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stage III nasal trauma. Examples of nasal scars. (A) Columella scar at 38 weeks of corrected age in a premature infant born at 27 weeks of gestational age (birth weight 650 g). (B) Columella scar and nasal deformity at 6 years of age in a premature infant born at 28 weeks of gestational age (birth weight 1160 g).
Discussion
Nasal trauma secondary to nCPAP is an adverse event with potential short or long-term consequences. Little data are available in the literature on this topic, with reported incidences ranging from 20% to 60%.11 14,–,16 Comparisons between published studies are difficult because of highly variable descriptions and definitions of nasal trauma, which can differ in severity from limited local redness to full necrosis.
We propose a simple and reproducible classification system including three stages adapted from the general classification of the US NPUAP17 18 Our results showed that nasal trauma secondary to nCPAP was a very frequent complication in neonates, with a rate of more than 40% in the studied population. The general incidence was greater than 30 cases/1000 days of nCPAP, with a vast majority of superficial trauma (88.3% of stage I). Our incidence of cases of stage II to III trauma (3.5 cases/1000 days of nCPAP) is comparable to those reported in a recent study on iatrogenic events in NICU (2.7 cases/1000 days of nCPAP).19
Frequency and severity of nasal trauma increased with lower gestational age (>90% in neonates <28 weeks of gestational age), lower birth weight, longer duration of nCPAP and longer NICU stay. Moreover, incidence of nasal trauma might be underestimated since some infants of lower gestational age and birth weight were excluded due to pre-existing nasal trauma secondary to nasal intubation. Estimated relative risk was significantly higher in patients <32 weeks of gestational age, weighing <1500 g, and those staying in the NICU >14 days. Duration of nCPAP >5 days was the strongest risk factor (OR 5.36, 95% CI 3.82 to 7.52), which is in agreement with a previous observation.14 Our results showed that the majority of nasal trauma appeared during the first days of nCPAP. Nasal trauma occurred rarely after several weeks of treatment. The immaturity of the skin could be implicated in the pathogenesis of such trauma.7 20 Cosmetic or functional sequelae of nasal trauma due to nCPAP have been reported with an unforeseeable need for surgery.9 10 21 No infant in our population needed surgical repair so far, but ulterior interventions may be required in two of them who kept a scar after several months.
Another possible complication of nCPAP trauma is nosocomial infections, as suggested by a study in neonates treated with oxygen cannulas.8 However, our study was not designed to evaluate this hypothesis and further data are required.
The use of the same nCPAP system during the study strengthens the internal validity of the study, even if it limits its generalisability. The role of different application systems on nasal trauma remains unclear and the need for research aimed to determine which device is the least traumatic was recently underlined in a Cochrane meta-analysis.22
Common recommendations for prevention of nasal trauma due to nCPAP in neonates include careful local monitoring and avoidance of pressure, friction and moisture.23,–,25 Since such measures were already in place for several years during the study period, they are unlikely to provide a sufficient prevention for the apparition of nasal trauma, but could help limit their severity.
In conclusion, this study is so far the largest prospective cohort study documenting the development of nasal trauma secondary to the use of nCPAP. We showed that nasal trauma is a very frequent complication of nCPAP, especially in more preterm infants, most often limited to a not blanching erythema appearing early in the course of the treatment. Long-term cosmetic sequelae are very rare and will require specialised follow-up and possible surgery. Further studies are needed in order to define preventive or therapeutic strategies to reduce this iatrogenic complication.
Acknowledgments
The authors are grateful to all families and infants who participated to the study. Thanks to Prof A Moessinger for helpful suggestions and critical review of the manuscript and V Blanc for handling of the paediatric iatrogenic events database. Also thanks to Prof S Fanconi and the Department of Paediatrics of the Centre Hospitalier Universitaire Vaudois for support.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.