





Abstract
More than 75,000 displaced Ethiopians have moved to Israel. Tuberculosis (TB) incidence in Ethiopia is 44 times higher than in Israel (344 versus 8 cases per 100,000 inhabitants, respectively). The aims of the present retrospective cohort study were to evaluate the pre-immigration screening process initiated in 2001 on pulmonary TB (PTB) morbidity and to assess its cost-effectiveness.
Ethiopian immigrants who were screened before departure (study group) were compared with those who were screened after arrival (comparison group).
Between 1998 and 2005, 24,051 Ethiopian immigrants arrived in Israel. PTB was diagnosed in 332 (1.4%) immigrants, an incidence density of 325 patients per 100,000 person-yrs. PTB cumulative incidence was lower in the study group than in the comparison group: 711 compared with 1,746 patients per 100,000 immigrants, respectively (rate ratio 0.4). PTB was detected significantly earlier in the study group than in the comparison group: 193 versus 487 days after entry, respectively. Disease incidence declined significantly during the first 2 yrs following immigration. A 5-yr predictive model indicated that 98 individuals would be free of PTB, saving US$91,055 on annual treatment cost, due to screening.
The pre-immigration screening process reduced pulmonary tuberculosis incidence in subsequent years following immigration. Pulmonary tuberculosis was diagnosed earlier in the screened group than in the comparison group and the process was found to be both cost-beneficial and cost-effective.
International immigration from developing to industrialised countries (“established market economies”) 1 increased by 17% between 1990 and 2005, and it is estimated that >190 million immigrants, defined as foreign-born persons legally admitted and expected to settle in the host country, are living outside of their home countries 2. This global movement is accompanied by public health concerns of the host countries regarding the threat of communicable infection dissemination from the immigrants to the indigenous population 3.
Israel has encouraged immigration of people of Jewish descent. This special trend of homecoming to Israel is distinctive in comparison with labour migration or immigration elsewhere, as Jewish immigrants are never refused residency, regardless of health status, age, education or sex. Thus, the possibility exists that the composition of newcomers to Israel may not meet the requirements of the work force, and may potentially include larger proportions of older and sick people, females, children and uneducated individuals. These subpopulations may be less prepared medically, mentally and socially for the stresses involved in immigration.
Tuberculosis (TB) incidence in Ethiopia is 344 cases per 100,000 inhabitants (data from 2005) 4. Following a few occurrences of retrospective detection of immigrants who were clinically infected with communicable diseases, such as pulmonary TB (PTB), meningococcal meningitis and rubella, even during the flight to Israel, the Israeli Public Health Services decided to change the process of medical absorption of the Ethiopian immigrants. Hence, a pre-immigration screening process of the eligible immigrants was initiated by establishing a health station in the Israeli embassy compound in Addis Ababa (Ethiopia) in April 2001. The targets of the new screening programme were: to minimise the arrival of infected immigrants; to speed up the medical screening procedures by providing the immigrants with “health clearance” within their first days in Israel; and to contain health expenses, as the immigrants are granted health insurance upon arrival. Previously, it had taken ∼1 month to perform similar screening procedures when the immigrants were already in Israel. Only following health clearance could the immigrants take part in educational, social and labour activities. Additionally, the screening procedure in Ethiopia reduces the cost of PTB treatment in Israel, benefiting from the lower cost of health commodities in Ethiopia and the high quality of Israeli health providers.
During the period of the current study (2001–2005), the pre-immigration screening procedure in Ethiopia included a medical evaluation, vaccinations against infectious diseases and TB screening, first by tuberculin skin tests (TSTs), which were read 48–72 h following intradermal injection, and secondly by chest radiographs (CXR), which were performed for each immigrant aged >6 months and then sent to Israel for reading. Individuals complaining of cough, weight loss or fever, as well as those whose CXR showed changes suggestive of PTB, were asked to provide sputum for microscopy on three consecutive days. Diagnosed PTB cases were treated in Ethiopia using directly observed therapy for 2 weeks or until sputum smears were negative, ensuring that the patients were no longer infectious. All other immigrants were transported to Israel and housed in absorption centres: hostels in the community guided by professionals who assist in the immigration process. A public health nurse visited the absorption centre within the first 2 weeks, collected the medical documents and blood samples for HIV, and performed a second TST on all individuals whose first TST showed indurations <10 mm in size. A positive reaction to the second TST represents a boosted reaction, indicating that infection has most likely occurred in the past. Patients with positive findings were referred to the regional TB clinic. Individuals in whom latent TB infection (LTBI) was identified were recommended preventive therapy, and directly observed therapy was initiated for LTBI cases aged <18 yrs or HIV infected.
The aims of the present study were to evaluate the impact of the pre-immigration screening process on PTB morbidity rates among Ethiopian immigrants in Israel and to assess its cost-effectiveness compared with the post-immigration screening process.
MATERIALS AND METHODS
A retrospective cohort analysis of surveillance data for all Ethiopian immigrants developing PTB in Israel between January 1998 and December 2005 was performed. In conjunction with the inauguration of the health station in Addis Ababa and the establishment of the pre-immigration process in April 2001, the “study group” contained immigrants for whom pre-immigration screening was performed and who arrived in Israel between June 2001 and December 2005. The “comparison group” was composed of immigrants for whom post-immigration screening was performed and who arrived in Israel between January 1998 and May 2001 (historical comparison).
The TB national registry (Ministry of Health, Jerusalem, Israel) is the primary source for the reporting of PTB. HIV status was obtained by cross-matching PTB cases individually with the national name-based HIV/AIDS registry (Ministry of Health). The figures for Ethiopian immigrants to Israel were obtained from the Ministry of Absorption (Jerusalem) and from the Jewish Agency (Jerusalem). Dates of arrival in Israel and mortality data were obtained by linking each of the PTB cases with the national civil registry (Ministry of Interior, Jerusalem). These figures enabled an accurate calculation of the time elapsed from the date of arrival until disease diagnosis for each patient, and death dates were verified at the end of the follow-up period. Laboratory results were compared separately for each PTB case with the national TB laboratory (Abu Kabir, Israel). TST results, when available, were obtained from the patients’ medical records.
PTB cases were defined by the presence of culture-confirmed disease due to Mycobacterium tuberculosis complex or two consecutive positive sputum smear examinations for acid-fast bacilli. The latter was the more common definition in Ethiopia. PTB was also defined when clinical judgements led to the decision to treat the patient with a full course of antituberculous therapy after failure of therapy with broad-spectrum antibiotics 5, 6.
Operation costs of the pre-immigration infrastructure in Addis Ababa were obtained from decision makers and liaison professionals supervising the operation of the health station. These included salaries, rent and costs of drugs and equipment used for diagnosis and treatment, CXR performed in Ethiopia and CXR readings performed in Israel. Costs of treatment in Israel were determined by the Ministry of Health tariff 7.
Morbidity trends were described using incidence, prevalence and central tendency features. Comparisons of categorical attributes between the study and comparison groups were performed using Chi-squared tests and the Fisher approach. Comparisons of continuous attributes were performed using unpaired t-tests for independent samples. Comparisons of patients’ survival periods, from date of arrival in Israel to either disease date or death, between the study and comparison groups were calculated using the Log Rank test for survival analysis. Mortality and disease incidence data were only available for the PTB cases. Thus, for both groups, the same assumption of “no additional deaths” was employed, in order to compare the net influence of the pre-immigration screening process.
RESULTS
Between 1998 and 2005, 24,051 Ethiopians of Jewish descent immigrated to Israel, a mean±sd (range) flux of 3,006±571 (2,228–3,791) immigrants annually. Pre-immigration and post-immigration screening was performed in 14,768 and 9,283 immigrants, respectively. The mean (range) age at immigration was 22 (0–98) yrs, and nearly 80% were aged <35 yrs.
A total of 332 (1.4%) Ethiopian immigrants both immigrated and were diagnosed with PTB between 1998 and 2005. In order to estimate the influence of the time elapsed from immigration date to disease diagnosis, 46 patients from the study group and 19 patients from the comparison group, who were diagnosed within 2 weeks of immigration, were identified and excluded from the analyses (fig. 1⇓). It was assumed that they had arrived in Israel with already active disease, and the first 2 weeks between immigration date and registration represent the delay in the reporting process by local health personnel. Thus, these patients were considered as point prevalent upon entry (270 PTB patients per 100,000 immigrants), rather than incident cases.

Study flow chart of Ethiopian immigrants to Israel who were diagnosed with tuberculosis (TB). In total, 24,051 Ethiopians immigrated to Israel in 1998–2005.
The remaining 267 immigrants who both immigrated and were diagnosed with PTB after 1998 were further divided into a study group, which included 105 individuals who were screened in Ethiopia and developed PTB in Israel, and a comparison group, which included 162 individuals who were screened following arrival in Israel and developed PTB in Israel. No major differences were detected in demographic determinants between the two groups (table 1⇓). The PTB incidence densities in the study and comparison groups were 267 and 324 cases per 100,000 person-yrs, respectively. The disease odds ratio (OR) between the study and comparison groups was 0.4.
Demographic characteristics of pulmonary tuberculosis patients among Ethiopians in Israel who immigrated and were diagnosed in 1998–2005, stratified by screening procedure#
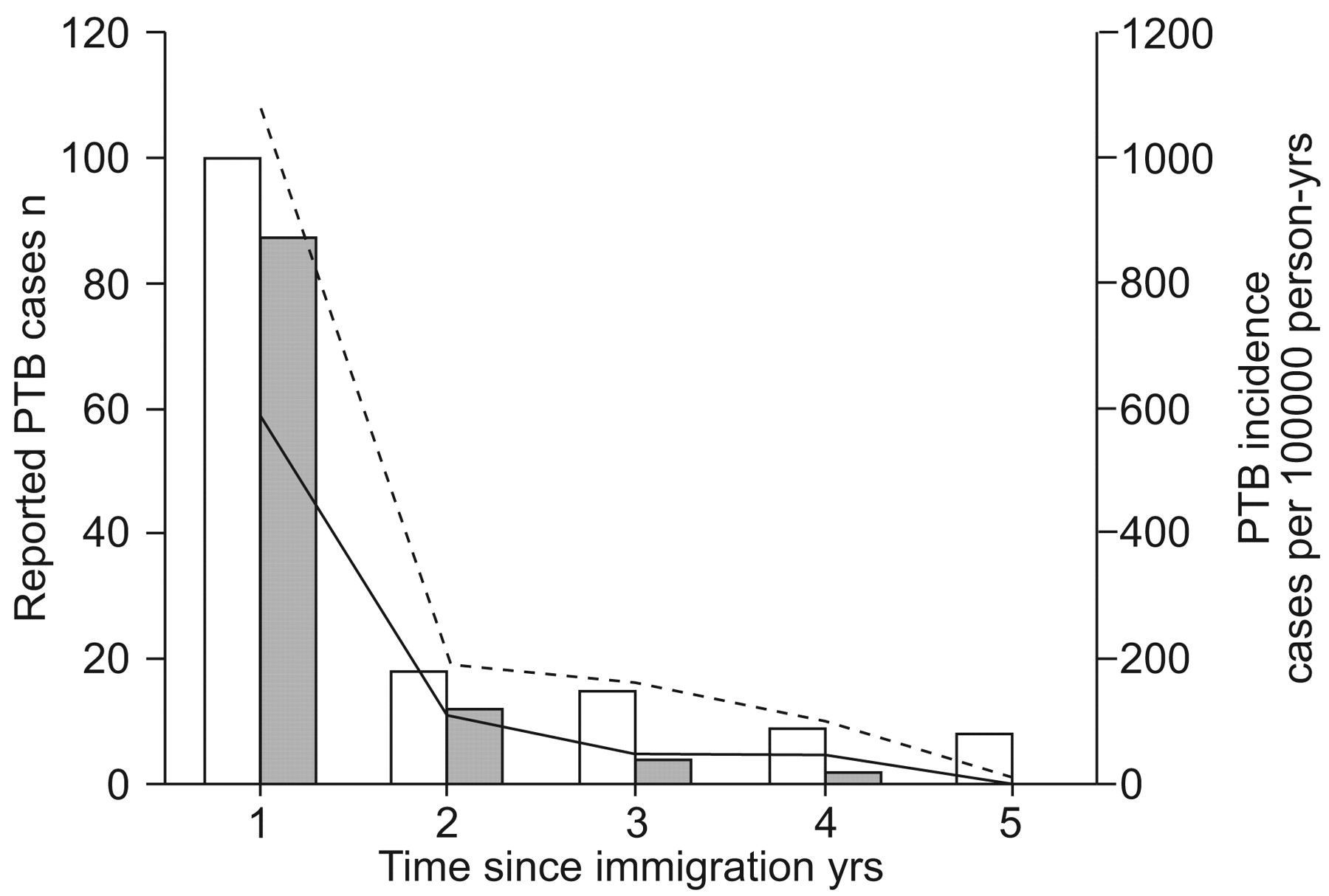
Both the numbers of PTB cases and the disease rates were lower in the study group than the comparison group for each of the years following immigration (rate ratio 0.82, p<0.01; table 2⇓) and decreased throughout the follow-up period. The most significant effect was noticed during the first year after arrival in Israel (fig. 2⇓).

Numbers of pulmonary tuberculosis (PTB) cases (□ and ▓) and incidence rates (······· and ––––) among Ethiopian immigrants, by length of time in Israel and screening procedure. □ and ·······: individuals screened post-immigration (comparison group); ▓ and ––––: individuals screened pre-immigration (study group).
Pulmonary tuberculosis(PTB) morbidity rates among Ethiopians in Israel who immigrated before or after initiation of pre-immigration screening, by length of follow-up after immigration
The time that elapsed between immigration date and disease diagnosis date (the detection period) was significantly shorter in the study group than in the comparison group (mean±sd 193±260 versus 487±640 days, respectively; p<0.01). Survival analysis demonstrated a continuous and increasing difference in detection period between groups over the follow-up period (OR 0.72, log rank test p = 0.002; fig. 3⇓).

{kind=link}
{kind=link}
{kind=link}
Survival function for the cohorts who immigrated before (comparison group; ·······) and after (study group; ––––) the pre-immigration screening process was initiated. Odds ratio (95% confidence interval): 0.72 (0.59–0.89); p = 0.002.
The HIV rate among PTB patients from the study group was not statistically different from that in the comparison group (12.3 and 12.4%, respectively; p = 0.99).
Based on the promising findings in morbidity trends following the initiation of the pre-immigration screening process, a 5-yr predictive model indicated that nearly 98 individuals would be free of PTB as a result of the screening process, if the immigration rate continued to be 3,000 individuals·yr−1 (table 3⇓). Any PTB case diagnosed in Ethiopia is treated before departure at a lower cost than in Israel. In addition, individuals diagnosed with LTBI are recommended preventive therapy. Expenses pertaining to the diagnosis, treatment and follow-up of each individual PTB case in Israel amount to US$7,619 7, whereas the annual cost for maintaining the health station in Addis Ababa for the screening process is US$60,100. Thus, the net direct saving in costs for the pre-immigration screening process is US$449,817 for 5 yrs, which is the cost of 98 PTB cases deducted from the cost of the maintenance of the health station during this period. Note that, due to the differences in the health services cost index between 2001 and 2005, sensitivity analysis may allow a 2.7% range.
A predictive model comparing probable pulmonary tuberculosis cases, assuming an annual influx of 3,000 screened immigrants
DISCUSSION
PTB incidence among the Ethiopian immigrants screened pre-immigration was lower than among immigrants who were screened post-immigration (267 versus 324 cases per 100,000 person-yrs, respectively). The incidence was highest in the first year of residence in Israel and declined in an exponential manner, particularly within the first 2 yrs following immigration.
The annual PTB incidence in Ethiopian immigrants during their first year in Israel was higher than the published Ethiopian national rate for PTB, which is 102 patients per 100,000 inhabitants (both smear-positive and -negative patients; data from 2005) 4, and also higher than that recorded among South-East Asian immigrants to Australia 6 and asylum seekers to the Netherlands 8 (74.9 and 284 patients per 100,000 immigrants, respectively). Incidence in the present study decreased significantly during the first years following immigration and became as low as 50 per 100,000 immigrants in the study group after 3 yrs, despite the relatively high HIV prevalence among Ethiopians in Israel (∼2% in 2004; Z. Mor, personal communication). As a general rule, immigrants from countries with incidence rates higher than this level are eligible for screening. It is worth noticing that the decline in PTB incidence reported from Denmark and the Netherlands on immigrants from Somalia, which borders Ethiopia at the Horn of Africa, was more gradual, showing sustainable annual TB incidence as high as 9.5% 7 yrs after arrival 9 and even after 10 yrs 10. The same phenomenon was recorded in the USA, where TB rates remain high for years in the older age groups of immigrants 11. The variations between these previous studies and the present findings can be partially explained by differences in the social status of the immigrants in the absorbing country. Somali refugees to Western Europe and migrant workers to the USA may be undocumented, discriminated against, under the threat of deportation and lacking access to medical facilities. Conversely, Ethiopian newcomers to Israel are naturalised upon arrival, are eligible for health and social insurance, governmental lodging, financial benefits, opportunities in the labour market, and free educational and nutritional support during the initial phase of assimilation in Israel. Additionally, Ethiopian immigrants in Israel are examined periodically by medical staff at the absorption centres. These efforts are encouraged by government, social and health authorities, and are regarded as core values in the Israeli moral ethos.
The health status of the Ethiopian immigrants may be worse than average migrant labourers, as they lived in rural areas in the country of origin, belong to the lowest social class, are uneducated, illiterate and a displaced population. Thus, the Ethiopian immigrants in Israel do not enjoy the “healthy migrant effect” as typical labour migrants. Nevertheless, most of the PTB cases were diagnosed early due to screening efforts and the effective medical vigilance of index cases and their contacts thereafter by the district health departments and by the TB regional clinics throughout the country. For this reason, expanding the screening process among immigrants during subsequent years in the host country, as suggested in the Netherlands 8 and Belgium 12, may be unnecessary in the Israeli setting.
The PTB point prevalence on arrival in the present study was 270 per 100,000 immigrants, which is lower than documented among asylum seekers at Heathrow Airport, London, UK 13 and in Belgium 14, but is higher than in Somalis screened in Norway 15 or in Switzerland 16 (415, 252, 248 and 198 cases per 100,000 immigrants, respectively). The gap in TB prevalence between Ethiopia and Somalia may be related to the relatively higher TB prevalence in Ethiopia, the age composition and the basic health status of the immigrants to Israel, and the active case-finding process applied to all immigrants.
PTB was diagnosed an average of 294 days earlier in the study group than in the comparison group. Several explanations are possible for this. First, detection of LTBI individuals by TST while in Ethiopia allowed a better follow-up in Israel and early detection and treatment of PTB cases and their contacts. Secondly, the establishment of a database of all the immigrants in the study group, which included pre-immigration CXR, TST and physical examination, allowed for easier and more rapid access and follow-up of PTB patients and their contacts while performing epidemiological investigations. Thirdly, time differences in immigration between the two groups led to greater experience among TB health professionals in Israel and the entire TB infrastructure in Israel being better equipped for diagnosis, treatment and follow-up of the immigrants, by the time the study group was assessed.
The pre-immigration screening process was found to be cost-beneficial in the current study, sparing 98 possible cases in 5 yrs from contracting PTB, and also cost-effective, saving direct expenses of US$90,000 per annum. The screening process takes advantage of the low cost of CXR and staff in Ethiopia relative to Israel, and has the advantage of size once the procedure is operated by a single provider. This calculation is conservative, as it does not capture the entire expected savings of the faster health clearance of the immigrants in the study group in a presumptive period of 1 month, compared with the post-immigration procedures practised in the comparison group. As those medically noncleared immigrants were unable to work or attend language classes during the time of the post-immigration screening, all 45% of the immigrants who were at working age were paid an unemployment fee of US$343 per month by the Israeli government, which totals US$2,083,500 paid by the national budget during the study period. Thus, the faster health clearance, as a consequence of the pre-immigration screening process, allowed the immigrants to integrate sooner into Israeli society and the labour market, saving governmental funds.
The pre-immigration screening process in Ethiopia further emphasises the value of centralised TB control performed by a single provider. The post-immigration screening was performed in a decentralised manner and was operated by multiple district health departments in Israel. Due to the variability of capabilities and experience between the health departments, each office responded differently in terms of time taken to screen the immigrants. As M. tuberculosis has the potential to spread in the community, control measures should begin at the earliest stage possible, preferably before departure. The present study demonstrates the advantage of a national organisation that is capable of funding and maintaining TB clinics, is responsible for reliable inter-organisational data flow and is able to establish a feedback mechanism.
As screening immigrants for TB is a fundamental activity performed by developed countries, the Israeli experience may demonstrate the benefits of centralised screening processes that are supported by a national organisation and provide incentive for both immigrants and the experts in diagnosing and treating TB.
The current study is subject to several limitations. First, there was a limited follow up period: 4.5 yrs for the study group and ≤7 yrs for the comparison group. However, due to the intensity and the quality of the screening process, the majority of PTB cases were detected in the first year following immigration. Secondly, only incomplete data were available regarding TST results among the immigrants. More complete data would have allowed examination of association between CXR and TST. Thirdly, the study group followed the comparison group, rather than being studied concomitantly. This sampling (selection) bias may have led to different immigration groups in time and better treatment in the later group, as a result of the learning curve of the staff treating the immigrants. However, interviewing key professionals involved in Ethiopian immigration to Israel, it appears unlikely that there are ethnic or demographic differences between the two groups. Fourthly, over-diagnosis (selection) bias in the study group may be differential in the direction of higher detection rates in that group. However, the actual findings of lower morbidity rates in the study group make this bias even more conservative, lowering the relative risk.
The strengths of the present study include the close follow-up of the entire cohort of all Ethiopian immigrants and every TB patient, the high sensitivity and specificity of case ascertainment in the unique database and the numerous total person-yrs of follow-up. The study included the entire immigrant population; thus, it is far less subject to both selection and information bias.
In conclusion, the pre-immigration screening process for pulmonary tuberculosis is centralised in nature, allows for unification of medical procedures and reduces the burden on local health departments and medical providers. It has proven to be effective among Ethiopian immigrants arriving in Israel. Following the process, pulmonary tuberculosis disease incidence was reduced and the infection was detected at earlier stages. The screening process was proven both cost-beneficial and cost-effective, and may be performed by other developed countries in order to ensure better tuberculosis detection in immigrants from high-tuberculosis prevalence areas.
Support statement
The present study was partially sponsored by the League against Tuberculosis and Lung Diseases (Rehovot, Israel) and the National Institute for Health Policy and Health Services Research (Tel Hashomer, Israel).
Statement of interest
None declared.
Acknowledgments
The authors wish to express their gratitude to the following experts: N. Koren-Morag (Tel Aviv University, Tel Aviv, Israel) for her professional biostatistics guidance; D. Chemtob, director of the Dept of Tuberculosis and AIDS in the Ministry of Health (Jerusalem, Israel), for his devoted assistance in data collection; and Z. Schwartzberg from the Jewish Agency, Ethiopian desk (Jerusalem, Israel), for his assistance in accessing and organising the immigrants’ documentation. The findings of this study were also presented in the thesis of Z. Mor for a Masters degree in Public Health at Tel Aviv University (Tel Aviv, Israel).
Footnotes
-
Earn CME accreditation by answering questions about this article. You will find these at the back of the printed copy of this issue or online at www.erj.ersjournals.com/current.shtml
- Received November 3, 2007.
- Accepted March 10, 2008.
- © ERS Journals Ltd
References










