





Abstract
Exercise training is an essential component of pulmonary rehabilitation. However, the cardiopulmonary stress imposed during different modalities of exercise training is not yet known.
In the present study, the cardiopulmonary stress of a 12-week exercise training programme in 11 chronic obstructive pulmonary disease (COPD) patients (forced expiratory volume in one second 42±12%pred, age 69±6 yrs) was measured. Pulmonary gas exchange and cardiac frequency (fC) of three training sessions were measured with a portable metabolic system at the beginning, mid-term and end of the programme. Symptoms were assessed with Borg scores.
The exercise intensity was compared with the recommendations for exercise training by the American College of Sports Medicine (ACSM). Training effects were significant (maximum change in work: 14±11 Watts, 6-min walk test: 44±36 m). Whole body exercises (cycling, walking and stair climbing) consistently resulted in higher cardiopulmonary stress (oxygen uptake (V′O2), minute ventilation and fC) than arm cranking and resistance training. Dyspnoea was higher during cycling than resistance training. Patients exercised for >70% (>20 min) of the total exercise time at >40% of the V′O2 reserve and fC reserve (“moderate” intensity according to the ACSM) throughout the programme.
The cardiopulmonary stress resistance training is lower than during whole-body exercise and results in fewer symptoms. In addition, exercise testing based on guidelines using a fixed percentage of baseline peak performance and symptom scores achieves and sustains training intensities recommended according to the American College of Sports Medicine.
Pulmonary rehabilitation (PR) programmes have consistently improved exercise capacity, symptoms and quality of life of patients with chronic obstructive pulmonary disease (COPD). Exercise training is an essential component of PR 1, and endurance training is commonly used. Generally, the endurance type of training applied during PR includes cycling and/or treadmill walking. Programmes including relatively high-intensity endurance training have proven to be effective 1. However, in addition to walking and cycling, other exercise modalities have been described during PR for COPD patients, e.g. resistance training 2, callisthenics 3, arm cranking 4 and stair climbing 5. In clinical rehabilitation, a combination of several of these exercises, is often applied. Although it is known that high intensity training leads to more desirable physiological training effects than low intensity training 6, the cardiopulmonary stress imposed by different exercises is not yet known. In addition, training intensity is conventionally set at a given fraction of an incremental peak exercise response. Due to the relatively slow oxygen uptake kinetics of patients with chronic diseases 7, 8, the actual metabolic load during somewhat longer exercise bouts may well be underestimated.
To improve cardiorespiratory fitness, the guidelines for exercise testing and prescription of the American College of Sports Medicine (ACSM) recommend for healthy individuals to exercise three to five times a week at 40–85% of the maximum oxygen uptake or heart rate reserve for >20 min continuously or at intervals 9. Whether these recommendations are achieved by patients with COPD is debated 1. It is unknown whether the exercise training regimens applied in the context of PR programmes are sufficient to exercise COPD patients at recommended intensities for healthy individuals. Moreover, the amount of time at which patients train, at given intensities, has not yet been studied.
Therefore, the present authors measured the cardiopulmonary stress of the different components of an exercise training programme in the context of pulmonary rehabilitation in patients with moderate-to-severe COPD. In addition, patients were also analysed to determine if they were able to exercise at intensities recommended by the ACSM.
MATERIALS AND METHODS
Study subjects
Eleven consecutive patients visiting the outpatient clinic entered the study. The following criteria were used for patient selection: 1) clinical diagnosis of COPD; 2) stable condition at inclusion with no recent infection or exacerbation; 3) remaining symptoms of dyspnoea and reduced exercise capacity despite optimal medical treatment; 4) no locomotor or neurological condition or disability limiting the ability to exercise; 5) no need of supplemental oxygen at rest or during exercise due to the inability of the equipment to measure oxygen uptake (V′O2) while breathing inspiratory O2 fractions >21%; and 6) patients had to be able to attend the outpatient rehabilitation centre three times per week. Patients who met the inclusion criteria gave oral informed consent to take part in the study. They performed testing at inclusion and after 3 months of outpatient pulmonary rehabilitation. All tests were part of the routine screening of COPD patients who enter a rehabilitation programme approved by the Medical Ethical Board of the University Hospitals Leuven, Leuven, Belgium. The tests consist of measurement of pulmonary function, peripheral and respiratory muscle strength, exercise capacity and quality of life. Details of all the performed tests have been described before 4.
Maximal exercise capacity
Maximal exercise capacity was assessed by maximal cycle ergometry. The test was performed on a magnetically braked cycle ergometer (Ergoline 900, Bitz, Germany) according to the standards of the American Thoracic Society/American College of Chest Physicians’ statement on Cardiopulmonary Exercise Testing 10. After 3 min of unloaded pedalling, patients cycled at an incremental work rate (+10 W·min-1) until exhaustion. Cardiac frequency (fC) was monitored continuously by a 12-lead electrocardiogram. Minute ventilation (V′E), V′O2 and carbon dioxide production (V′CO2) were measured throughout the test. V′O2,max was referred to predicted values 11. On-line calculations of breath-by-breath V′E, V′O2, V′CO2 and respiratory exchange ratio (RER) were obtained using the VmaxST 1.0 (Viasys, MEDA, Belgium), a portable metabolic system. The device was secured to the upper chest with a harness and, due to its low weight (650 g), it gave minimal discomfort. The volume measurement was carried out by a turbine (Triple-V® Sensormedics BV, Bilthoven, the Netherlands). V′O2 was analysed using an electrochemical cell, and V′CO2 was measured using an infrared analyser. A similar model of this device has been validated by Prieur et al. 12. A face mask (Hans Rudolph Inc., Kansas City, MO, USA) with a dead space of <30 mL was carefully adjusted to the patient’s face and checked for air leaks.
Training programme
The 12-week training programme consisted of 1.5-h training sessions, which patients attended three times per week. The circuit training included cycling, walking and leg press resistance training, stair climbing and arm cranking. The training programme was based on previous experience 4 and driven by the patients’ perception of their symptoms. Training intensity was set at 60% of the initial maximal work rate for ergometry cycling, at 75% of the average walking speed during the 6-min walk test (6MWT) for treadmill walking and at 70% of the one repetition maximum (1RM; the maximum load which can be moved only once over the full range of motion without compensatory movements) for leg press resistance training. For walking, the average walking speed was determined by dividing the distance walked by the time (6 min) during the 6MWT performed at admission to the rehabilitation programme. Arm cranking and stair climbing (two-step chair) were performed in 2-min blocks (1–3 sets). Physiotherapists increased patients’ work rates or duration on a weekly basis, guided by a schedule and Borg-symptom scores. A Borg score of 4–6 for dyspnoea or fatigue was set as a target 13. Close supervision was provided during training, with a ratio of one physiotherapist for every four patients. In addition to the exercises, patients also followed education sessions regarding disease management and medication use. There was also individual psychological and social counselling, and nutritional and occupational therapy.
Exercise training session assessments
By the end of weeks 1, 6 and 12 of the PR programme, patients performed one exercise training session with the VmaxST. On-line breath-by-breath measurement of V′E, tidal volume (V′T), V′O2, V′CO2, respiratory rate (RR) and the ratio between inspiratory time and total cycle time (ti/ttot) were recorded by the VmaxST throughout the training session. fC was assessed using a heart rate monitor (Polar®; T31, Kempele, Finland). All variables were recorded at rest (2-min baseline) and during the whole exercise training session, which was identical to the previous clinical rehabilitation session. The session was supervised by a different physiotherapist, who was not involved in the clinical management of the patient. The exercises were performed in a fixed order. After 2 min of unloaded cycling as a warm-up, patients started the loaded cycling, which was followed by leg press resistance training, treadmill walking, arm cranking and finally stair climbing. Sufficient rest was assured after each exercise (patients rested until they felt able to continue). Patients could move freely without discomfort, as the device has a low weight. Pilot data showed that patients were not hindered in their exercise performance by the device 14, 15. The face mask could be removed during the resting periods between exercises, if necessary.
Patients were asked to grade their symptoms of dyspnoea and fatigue during the exercises using the modified Borg score.
Data handling
Signals from the VmaxST were transmitted during the training session by telemetry to a portable computer for online inspection of data quality. After the test, stored data were downloaded from the VmaxST to ensure complete breath-by-breath datasets and analysed with computer software.
In order to label the intensity at which patients were exercising, the recommended exercise intensity according to the Guidelines of the ACSM was applied to the cardiopulmonary data 10. The ACSM recommends an intensity of exercise corresponding to 40–85% of oxygen uptake reserve (V′O2,R) or cardiac frequency reserve (fC,R) to increase and maintain cardiorespiratory fitness 16. The V′O2,R is calculated from the difference between resting and maximum V′O2. Similarly, fC,R is the difference between resting and maximum fC. The thresholds considered as “moderate” and “hard” by the ACSM were used 16. This means training intensities >40% (moderate) and 60% (hard) of the V′O2,R and fC,R. To estimate the training intensity moderate and hard, 40 and 60% of this value, respectively, was added to the resting V′O2 and/or resting fC and is expressed as a percentage of V′O2,R or fC,R. A typical formula reads as follows:
V′O2,R = V′O2,rest+0.6 (V′O2,max - V′O2,rest)
Statistical analysis
Data were checked for normal distribution with the Kolmogorov–Smirnov test. The effects of exercise training were analysed with paired t-test. The cardiopulmonary measurements assessed in weeks 1, 6 and 12 were analysed with the repeated-measures ANOVA. If a p-value was <0.05, Tukey's post test was performed. For the symptom scores, the comparison was carried out with the Friedman test. In this case, if a p-value was <0.05, the Dunn's post test was performed. The level of significance for all comparisons was set at p<0.05.
RESULTS
The studied group (table 1⇓) showed moderate-to-severe airflow obstruction and was classified within Global Initiative for Chronic Obstructive Lung Disease stages II (n = 4), III (n = 4) and IV (n = 3). One patient had an acute exacerbation and could not be reassessed at week 6. Another patient withdrew from the rehabilitation programme at week 12 for personal reasons and could not perform the final exercise training session with the VmaxST. However, all the other measurements after 12 weeks were successfully performed by this patient. Although the assessments with the VmaxST throughout the exercise training sessions were well tolerated by patients, in week 12 two patients reported difficulties exercising while wearing the equipment (6% of measurements).
Baseline characteristics.
Training effect
As expected, FEV1 remained unaltered after 12 weeks of exercise training (ΔFEV1 = 0.02±0.18 L; p = 0.41). V′O2,max, Wmax and 6MWT increased significantly after training (0.09±0.13 L·min-1, 14±11 W and 44±36 m, respectively; p<0.05 for all). There was no statistically significant difference in isometric quadriceps force (ΔQF = 5±16 N·m-1; p = 0.25), despite a significant increase of the training load of the leg press resistance training during the programme (Δload = 53±30 kg; p = 0.0001, which represents 43±26% increase). V′O2, V′CO2, V′E and fC at iso-work rate (100% of the initial maximal work rate) decreased significantly after 12 weeks of exercise training (reductions of 7, 15, 9 and 7%, respectively; p<0.02 for all).
Cardiopulmonary response and symptoms during the exercise training programme
Figure 1⇓ shows the progression of the training load for cycling, leg press resistance training and walking during the exercise training programme. There were patients who sustained high intensity training from the first week on and were able to tolerate further increments in the exercise load during the programme. However, others improved their training load less than predicted (fig. 1⇓). Participation rate was 97%.

Work rate progression of a) cycling, b) leg press resistance training and c) treadmill walking during the exercise training programme. _____: individual progression of each patient; -----: anticipated progression. Wmax: baseline maximal work rate; 1RM: baseline one repetition maximum (the maximum load which can be moved only once over the full range of motion without compensatory movements); 6MWT: baseline 6-min walk test.
There was no difference in heart rate before starting a given exercise in weeks 1, 6 and 12 (p = 0.39, 0.60 and 0.36, respectively).
There was an overall increase in V′O2, V′E and fC during leg press and arm cranking throughout the 12-week programme (p<0.05 for both). V′E during stair climbing was also higher in week 12 (p = 0.02). For the remaining exercises, despite significant increase in work rate, V′O2, V′E and fC remained unchanged over time. Symptoms reported during exercises did not change throughout the programme, except for an increased dyspnoea during arm cranking (p<0.05) and an increase in fatigue during walking (p = 0.02) at the end of the programme.
V′O2, V′E and fC responses of a representative patient during a training session in week 1 are illustrated in figure 2⇓. This patient (male, 51 kg, FEV1 0.88 L) cycled at 55 W (69% Wmax) for 10 min, performed leg press resistance training (three sets of eight repetitions) with 110 kg (70% 1RM), walked on the treadmill with a speed of 4.2 km·h-1 (74% 6MWTspeed) for 10 min, and performed arm cranking and stair climbing, each for 2 min. The values of V′O2, V′E and fC achieved at the end of the different exercises by this patient were close to the maximal values obtained during the initial incremental exercise test.
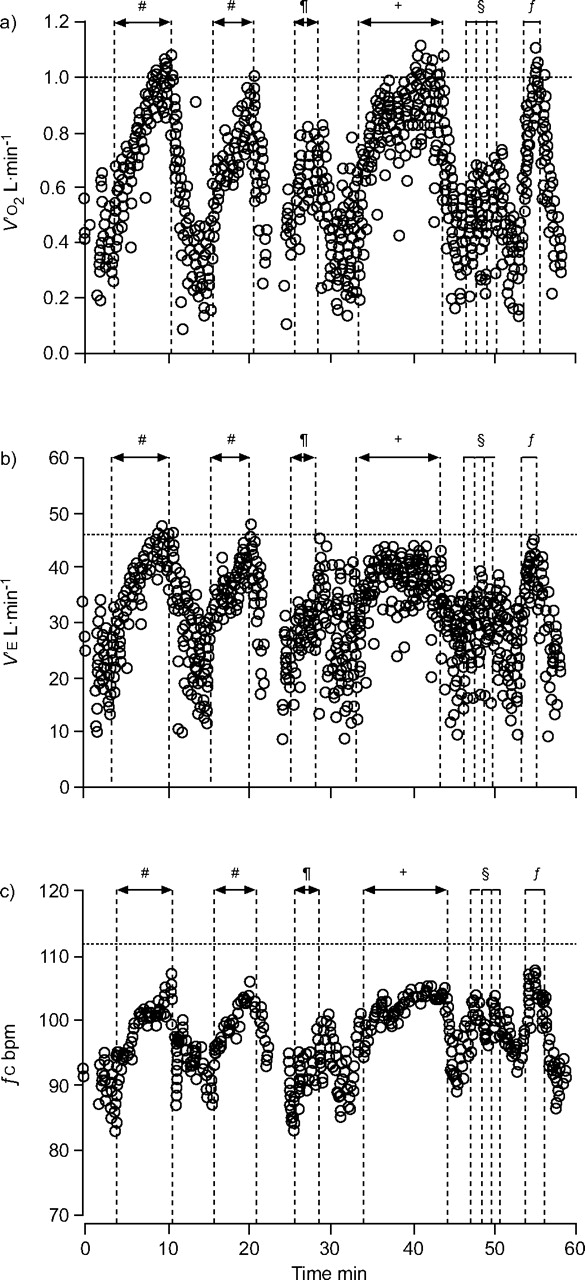
a) Oxygen uptake (V′O2), b) minute ventilation (V′E), and c) cardiac frequency (fC) in a representative patient during one exercise session in week 1. -----: V′O2,max (a), V′E,max (b) and HRmax (c) achieved during baseline incremental exercise in this patient. #: cycling; ¶: leg press resistance; +: treadmill walking; §: arm cranking; ƒ: stair climbing.
The average cardiopulmonary stress imposed by the different exercise modalities throughout the training programme is shown in table 2⇓. Relatively high intensity exercise in terms of V′O2, V′E and fC was reached from the first week on. The cardiopulmonary responses were lower during arm exercises (arm cranking) and resistance training (leg press) when compared with whole body exercises (cycling, walking and stair climbing; table 2⇓). Similarly to V′O2, V′E and fC, symptoms of dyspnoea reported by patients were consistently lower during leg press when compared to cycling (p<0.05 week 1, 6 and 12). In terms of fatigue sensation, leg press induced less fatigue than cycling at week 12 (p<0.01).
Average time, mean oxygen uptake(V′O2), mean minute ventilation (V′E) and mean cardiac frequency (fC) for all exercises from one training session in weeks 1, 6 and 12
The ventilatory equivalent for oxygen (V′E/V′O2) was systematically lower during walking when compared to cycling during the programme (p<0.001). Note that V′O2 was not different between these two exercises. The RER was also higher during cycling when compared with walking in weeks 1 and 12 (p<0.0001).
Exercise time and thresholds of exercise intensity
The duration of the trainings increased over time and were 66±7, 81±7 and 80±13 min in weeks 1, 6 and 12, respectively (ANOVA, p = 0.02). The corresponding exercise time was 30±3 min in week 1, 38±4 min in week 6 and 36±10 min in week 12 (ANOVA, p = 0.03). This represents 46, 47 and 45% (weeks 1, 6 and 12, respectively) of the training session.
Figure 3⇓ shows the total exercise time as well as the time above the thresholds considered moderate and hard (≥40 and ≥60% of V′O2,R and fC,R, respectively) by the ACSM in weeks 1, 6 and 12. Patients spent >80% of the total exercise time above 40% of V′O2,R (moderate threshold; 88±7, 89±7 and 84±9% in weeks 1, 6 and 12, respectively; ANOVA, p = 0.18). Concerning the fC,R, patients achieved moderate intensities for >70% of the total exercise time (76±29, 71±22 and 83±23% in weeks 1, 6 and 12, respectively; p = 0.36; fig. 3a⇓). For the threshold considered hard (≥60% of V′O2,R or fC,R), patients spent 67±25% of the total exercise time above this intensity in terms of V′O2,R in week 1 and 75±15% in weeks 6 and 12 (ANOVA, p = 0.33). Slightly less time was spent above the intensity hard in terms of fC,R; 51±42% in week 1, 48±30% in week 6 and 64±34% in week 12; ANOVA, p = 0.26; fig. 3b⇓).
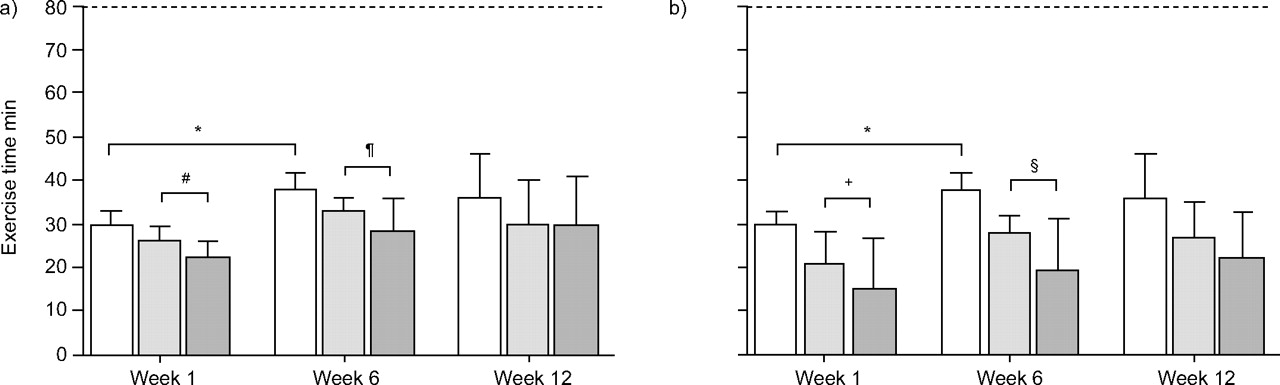
Total exercise time performed in weeks 1, 6 and 12 (open bars) and time above the thresholds in a) moderate (≥40% of oxygen uptake reserve (V′O2,R) or cardiac frequency reserve (fC,R); □: total exercise time; ░: time ≥40% V′O2,R; ░: time ≥40% fC,R) and b) hard (≥60% of V′O2,R or fC,R; □: total exercise time; ░: time ≥60% V′O2,R; ▒: time ≥60% fC,R). Data are expressed as mean±sd. The increase in exercise time is indicated (*p<0.05). -----: average duration of the training sessions (exercise time+resting time). #: p = 0.12; ¶: p = 0.11; +: p = 0.059; §: p = 0.054.
There was poor agreement between the thresholds based on the V′O2,R in comparison to those based on the fC,R throughout the programme. An example of this lack of concordance between these two thresholds of exercise intensity is shown in fig. 4⇓.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bland and Altman plot showing the poor agreement between time spent in exercises >40% of the oxygen uptake reserve (V′O2,R) and >40% of the cardiac frequency reserve (fC,R). –·–·–·–·: upper limit (mean+(1.96×sd)); ------: lower limit (mean-(1.96×sd)); – – – –: mean.
DISCUSSION
The present study showed that the applied exercise training programme enabled the studied group to achieve and sustain training intensities that are well within the limits of what is proposed to be effective for healthy adults according to the ACSM. In addition, resistance training (leg press) resulted in less cardiopulmonary stress when compared with whole body exercises. Lastly, a poor concordance between intensity based on V′O2,R and heart rate reserve was shown, i.e. an acceptable training intensity in terms of V′O2,R was reached at a heart rate which would be considered too low.
Work rate progression and whole body exercises
Although guidelines were given for work rate progression, this progress was variable among patients due to symptoms (fig. 1⇑). The work rate progress patients presented during the training may partially have been the result of an improvement in movement efficiency, as a relatively larger increase was observed in training load (intensity and duration) than in V′O2. Milani et al. 17 have previously shown that COPD patients improve mechanical efficiency to a larger extent than V′O2 after exercise training.
For most of the patients, the intensity achieved during cycling, walking and stair climbing was high enough to produce oxygen consumption and ventilation close to maximal responses achieved in the baseline incremental cycling. Although the three whole-body activities (cycling, walking and stair climbing) resulted in similar cardiopulmonary responses, they have different characteristics and were performed in different ways. During cycling, most of the patients performed interval training (5–8 sets of 2-min blocks). This is a common approach to be able to train at relatively high work rates. Others have shown that COPD patients achieve higher work rates during interval training when compared with continuous training 18. During treadmill walking, most of the patients tolerated longer blocks of continuous exercise, even with increments in walking speed and duration. This is probably due to the differences between these two exercise modalities. In comparison with cycling, walking has been shown to be less fatiguing and to produce less lactate at similar V′O2 levels 19–21. Hence, patients are able to exercise for longer periods. During cycling, more lactate is produced, which results in a continuous rise in ventilation (the so-called slow phase of ventilatory rise at iso-load) 20. In order to cope with the increasing ventilatory stress, the exercise blocks (especially during cycling) were divided into shorter blocks. Although lactate was not measured in the present study, the higher RER and V′E/V′O2 during cycling compared with walking are suggestive of more lactate production. In addition, other differences during cycling and walking, such as more hypoxaemia 21, 22 and increased dead space 21, may also have influenced the performance of these exercises.
During stair climbing, patients also stepped in short blocks (1–3 sets of 2-min blocks). This activity resulted in similar levels of V′O2, V′E, fC and symptoms to cycling and walking. The profile of stair climbing is, however, different, as patients reach peak exercise responses very quickly. Therefore, it is difficult, if not impossible, to sustain this activity for longer periods with the current applied pace (∼22 steps·min-1) and step height (21 cm). The fixed order of the exercises, with stair climbing being the last one, could potentially have led to a gradual increase in the cardiopulmonary stress and may have increased kinetics of the cardiopulmonary adaptation 23. However, patients were able to rest for long periods before starting a given exercise, which allowed heart rate to decrease sufficiently after each activity. Furthermore, others have shown the high cardiopulmonary stress imposed by stair climbing. Previous studies have shown that in patients with chronic airflow obstruction 24 and chronic heart failure 25, stair climbing represents strenuous exercise, eliciting physiological responses similar to cycle ergometry and treadmill tests.
Arm exercise and resistance training
The cardiopulmonary stress imposed by arm exercise and resistance training was lower when compared with whole body exercises (cycling, walking and stair climbing). Carter et al. 26 found reduced work capacity for arms compared with legs in COPD patients. This is a consequence of the smaller muscle mass involved during arm exercises. However, although the cardiopulmonary response was lower during arm cranking in comparison with cycling, there was no difference in symptoms of dyspnoea. This may be due to the features of the pulmonary disease which may also hinder the performance of arm work, such as dyssynchronous breathing 27, involvement of inspiratory muscles of the rib cage in upper torso and arm positioning 28, nutritional status 29 and dynamic hyperinflation 30.
For leg press resistance training, in addition to the lower cardiopulmonary stress, patients also experienced less dyspnoea in comparison to cycling. Richardson et al. 31 showed that exercising the quadriceps muscle alone (knee extensor exercise) resulted in lower peak values of V′O2, V′E and fC and fewer symptoms of dyspnoea when compared with cycling. In addition, the lower cardiopulmonary stress achieved during leg press can also be attributed to the average duration of this exercise. The exercise time for leg press was 2 min throughout the training (three sets of eight repetitions), which may also have contributed to the lower cardiopulmonary response The reduced sensation of dyspnoea during leg press is not surprising, since, during resistance training, patients are not usually limited by the central cardiorespiratory limitations commonly present in COPD. This will result in fewer symptoms, and consequently, patients are able to achieve significantly higher relative work rates 31, 32. Although patients presented an increase in load during quadriceps resistance training, this progression was lower than what was anticipated based on experience in healthy elderly 33, 34. However, the load progression observed in the present study was similar to that achieved in other studies, including COPD patients, which showed a significant effect on lower limb muscle force 2, 5.
Exercise time and thresholds of exercise intensity
In the present study, patients spent less than half of the total time of the training session executing the prescribed exercises. This was due to the characteristics of most of the exercises performed (intermittent) and the relatively long periods of rest patients needed in order to recover after each exercise. Intermittent exercise has been shown to be time consuming 35. In addition, Lacasse et al. 36 showed that COPD patients have a lower heart rate recovery after exercise when compared with healthy subjects, requiring longer rest periods.
There was a higher variability in exercise time in week 12. This was probably due to the fact that two patients could not perform the exercises as planned because of complaints such as dyspnoea on the day of the assessment.
The thresholds of exercise intensity achieved in the present study are those proposed by the ACSM to improve cardiorespiratory fitness. Exercises should be performed between three and five times a week for >20 min (or, at lower intensity, preferably 30 min), either continuously or in intervals, at an intensity of 40–85% of the V′O2,R or fC,R 9. In the present study, patients succeeded in achieving these thresholds, as they exercised three times a week at >40% of the V′O2,R (which corresponded to 55% of baseline V′O2,max) and fC,R (corresponding to 84% of baseline fC,max) for >20 min (considered as moderate intensity by the ACSM). When higher intensities were set (≥60% of the V′O2,R and fCR; ACSH's hard intensity), it was observed that the time period during which patients were exercising at such intensities was lower. However, patients still remained >20 min above the threshold hard for V′O2,R (corresponding to 70% of baseline V′O2,max). In terms of fC,R, patients only exercised at ≥60% of the fC,R (which corresponded to 89% of baseline fC,max) for >20 min in week 12. In the present study, training intensities target following published guidelines and symptoms resulted in a homogeneous response of thresholds based on V′O2. Much more variable, however, was the response based on fC. The poor agreement between time spent above the thresholds based on V′O2 and fC may be related to different factors. The differences between the fC and V′O2 kinetics might be one of the factors. It has been shown in COPD that fC kinetics are slower when compared with V′O2 kinetics during exercise 8. In addition, ventilatory limitation to exercise is often present in patients with COPD. Consequently, it is common that patients stop exercising before reaching their cardiocirculatory limits 37. These features indicate that heart rate may not be an appropriate target to set exercise intensity to COPD patients; this has been previously suggested by others 38.
Limitations of the study
Patients who needed oxygen supplementation could not be included in the study. This was due to the inability of the VmaxST equipment to measure V′O2 while breathing inspiratory O2 fractions >21% (room air). Therefore, the present results may not be readily extrapolated to the more severe patients. However, since leg press resistance training elicited less V′E and dyspnoea than whole body exercise in the present study, it might be expected that the more severe patients may especially benefit from this type of exercise. These patients usually have dynamic hyperinflation 30 and ventilatory limitations are more apparent, hence, small muscle group training may be especially interesting in this population.
The present study does not allow identification of the minimal training intensity at which COPD patients should exercise in order to achieve physiological training effects. Rather, the cardiopulmonary stress imposed was investigated during clinical rehabilitation at a given fraction of the peak work rate.
The small sample size could be considered a limitation, since it may hinder the generalisation of the results. Specifically, severely oxygen-dependent COPD patients were not included in the present study. In addition, although the exercise training applied to the COPD patients is rather similar among centres, there might be differences in the programmes which may result in different cardiopulmonary stress. Nevertheless, the present data strongly support the relatively high cardiopulmonary stress of whole body exercise training in COPD.
In summary, the results of the present study provide new insights into training intensity imposed on chronic obstructive pulmonary disease patients with conventional exercise training programmes, since the majority of the patients trained at relatively high work rates. Without knowing the results of the metabolic assessments during the training, physiotherapists were able to keep patients at high intensity training based on guidelines using a fixed percentage of baseline peak performance further guided by symptoms scores. The patients with moderate-to-severe airflow obstruction included in the study tolerated relatively high intensity training and obtained significant improvements in exercise capacity after completion of the programme. The cardiopulmonary stress during resistance training is, as expected, lower than during whole-body exercise and results in fewer symptoms. The applied exercise training programme enabled the studied group to achieve and sustain training intensities that are recommended according to the American College of Sports Medicine. Exercise training based on guidelines using a fixed percentage of baseline peak performance and symptom scores seems to result in relatively homogeneous oxygen uptake response, while cardiac frequency response is much more variable. This would not incite for the use of cardiac frequency to guide training intensity in chronic obstructive pulmonary disease.
Acknowledgments
The authors would like to thank the following for the fundamental help in the assessments: I. Coosemans, V. Barbier, I. Muyllaert, A. Debrock, M. van Vliet, G. Maury, E. Libaert, L. Vandromme and the Lung Function staff of the Respiratory Dept from UZ Gasthuisberg, Leuven, Belgium.
- Received September 22, 2005.
- Accepted February 23, 2006.
- © ERS Journals Ltd
References










