Article Text

Abstract
Objectives A recent update of the definition of acute respiratory distress syndrome (ARDS) proposed an empirical classification based on ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) at ARDS onset. Since the proposal did not mandate PaO2/FiO2 calculation under standardised ventilator settings (SVS), we hypothesised that a stratification based on baseline PaO2/FiO2 would not provide accurate assessment of lung injury severity.
Design A prospective, multicentre, observational study.
Setting A network of teaching hospitals.
Participants 478 patients with eligible criteria for moderate (100<PaO2/FiO2≤200) and severe (PaO2/FiO2≤100) ARDS and followed until hospital discharge.
Interventions We examined physiological and ventilator parameters in association with the PaO2/FiO2 at ARDS onset, after 24 h of usual care and at 24 h under a SVS. At 24 h, patients were reclassified as severe, moderate, mild (200<PaO2/FiO2≤300) ARDS and non-ARDS (PaO2/FiO2>300).
Primary and secondary outcomes Group severity and hospital mortality.
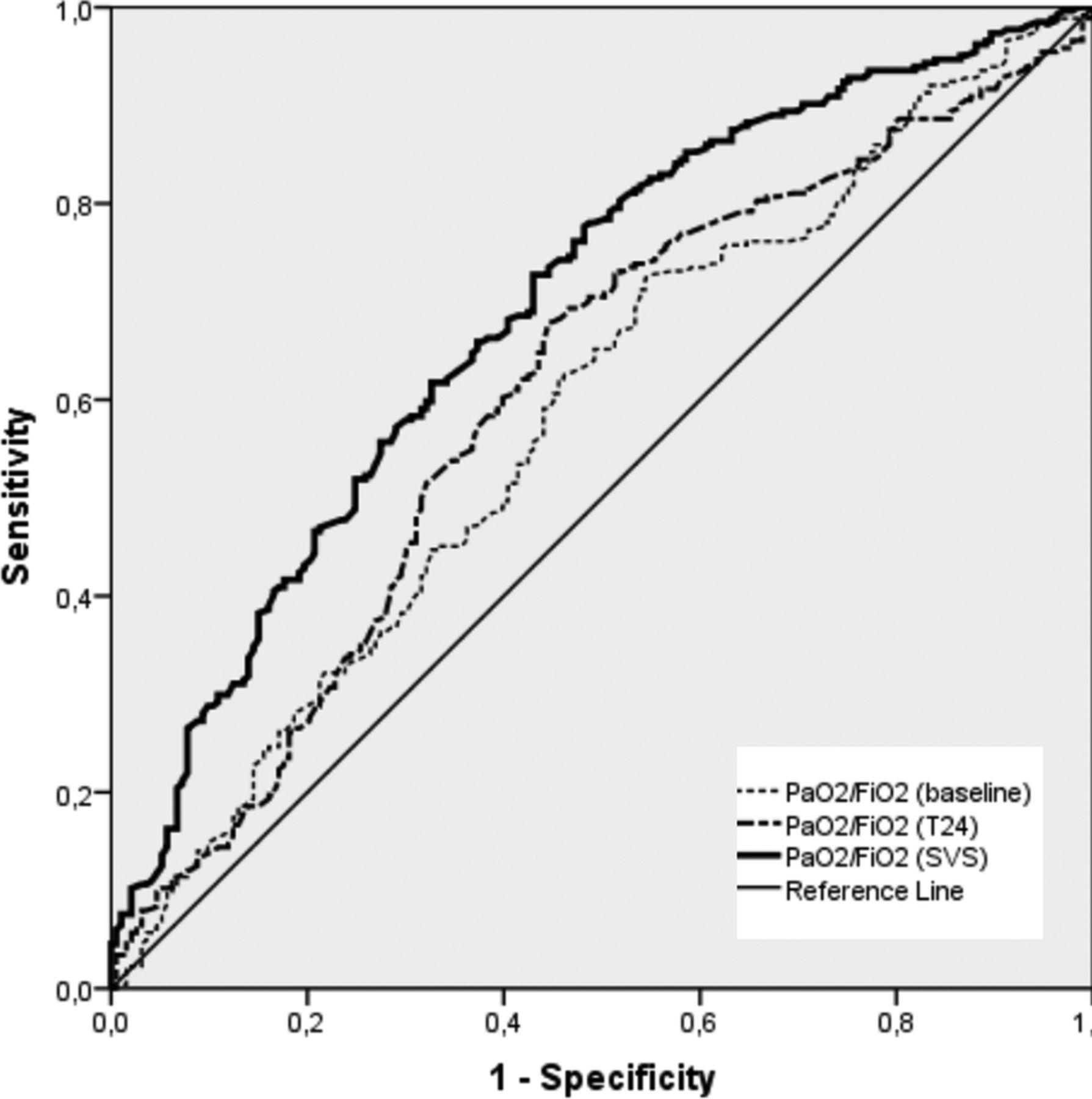
Results At ARDS onset, 173 patients had a PaO2/FiO2≤100 but only 38.7% met criteria for severe ARDS at 24 h under SVS. When assessed under SVS, 61.3% of patients with severe ARDS were reclassified as moderate, mild and non-ARDS, while lung severity and hospital mortality changed markedly with every PaO2/FiO2 category (p<0.000001). Our model of risk stratification outperformed the stratification using baseline PaO2/FiO2 and non-standardised PaO2/FiO2 at 24 h, when analysed by the predictive receiver operating characteristic (ROC) curve: area under the ROC curve for stratification at baseline was 0.583 (95% CI 0.525 to 0.636), 0.605 (95% CI 0.552 to 0.658) at 24 h without SVS and 0.693 (95% CI 0.645 to 0.742) at 24 h under SVS (p<0.000001).
Conclusions Our findings support the need for patient assessment under SVS at 24 h after ARDS onset to assess disease severity, and have implications for the diagnosis and management of ARDS patients.
Trial registration numbers NCT00435110 and NCT00736892.
- RESPIRATORY MEDICINE (see Thoracic Medicine)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Our risk stratification approach has potential implications for diagnosis, for guiding therapy and for future design of clinical trials in patients with acute respiratory distress syndrome (ARDS).
-
We cannot expect that our approach for risk stratification will hold for patients ventilated in a non-lung protective manner since it is clear that ventilation with large tidal volumes and high end-inspiratory plateau pressures cause ventilator-induced lung injury in addition to the pre-existing ARDS.
Introduction
Acute respiratory distress syndrome (ARDS) is an inflammatory process of the lungs resulting in increased permeability and subsequent interstitial and alveolar protein-rich oedema.1 ARDS is characterised by severe hypoxaemia, reduced lung compliance and bilateral radiographic pulmonary infiltrates.1 ,2 Patients with ARDS require mechanical ventilation (MV) with positive end-expiratory pressure (PEEP) for decreasing the work of breathing and for improving oxygenation. Current hospital mortality approximates 40–50% in major epidemiological series.3 ,4
Since diagnosis is based on a combination of clinical, radiographic and physiologic criteria, these criteria allow the inclusion of a diverse group of patients. The original description of ARDS was incapable of identifying a uniform group of patients.5 A precise definition is crucial since the effects on outcome of MV and adjunctive techniques depend on the degree of lung injury.6 In 1994, an American-European Consensus Conference (AECC)7 formalised the diagnostic criteria for ARDS and acute lung injury (ALI) but these definitions have been challenged over the years.8 ,9 In 2012, a proposal for updating the ARDS definition (the Berlin criteria) was published.10 Three ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) cut-off values recorded at ARDS onset: severe (≤100 mm Hg), moderate (>100−≤200) and mild (>200−≤300), were proposed. By only considering patients who were on PEEP≥5 cm H2O at the time of study enrolment, the panel found that hospital mortality increased with every stage of PaO2/FiO2 severity.
Since the Berlin criteria, similar to the AECC criteria, did not mandate the assessment of hypoxaemia under standardised ventilator conditions, we hypothesised that PaO2/FiO2 values recorded at ARDS onset or at 24 h without standardisation of ventilatory management would not provide accurate assessment of ARDS severity. To test our hypothesis, we sought to characterise 478 consecutive patients with ARDS, most of them enrolled in two published multicentre observational studies,9 ,11 using the Berlin criteria at ARDS onset and reassessed after 24 h of routine clinical care and at 24 h under standardised levels of PEEP and FiO2.
Methods
Data were derived from patients included in two independent, multicentre, observational cohorts that enrolled consecutive patients from 2004 to 2005 and from 2008 to 2010 in a network of intensive care units (see online supplementary appendix), under the Spanish Initiative for Epidemiology, Stratification and Therapies of ARDS (SIESTA) Program, as described previously.9 ,11
Study participants
Patients meeting criteria for ARDS using the AECC definition7 were considered for enrolment in the parent studies.9 ,11 Since all patients were on PEEP≥5 at study entry, they also met the recent Berlin criteria for moderate and severe ARDS.10 Although patient care was not strictly protocolised, physicians were asked to follow current standards for critical care management. For ventilatory management, it was recommended that patients be ventilated with a tidal volume (VT) of 5–8 mL/kg predicted body weight (PBW), at a ventilatory rate to maintain PaCO2 at 35–50 mm Hg, a plateau pressure <30 cm H2O, and PEEP and FiO2 combinations to maintain PaO2 >60 mm Hg or SpO2 >90%. During the enrolment period, none of the patients were included in any other clinical trial or managed with prone ventilation, high frequency ventilation or extracorporeal life support.
For the present study, onset of ARDS was defined as the day and time in which the patient first met ARDS criteria. Demographics, arterial blood gases, radiographic, haemodynamic and ventilator data were collected at study entry, at 24 h, at days 3, 7, 14 and last day of MV. ALI severity score12 and ventilator-free days (VFDs), were calculated and recorded. Total number of extrapulmonary organ failures included in the Sequential Organ Failure Assessment (SOFA) scale13 was documented daily. Patients were followed-up until hospital death or discharge. Approximately 24 h after meeting moderate/severe ARDS criteria, oxygenation was assessed under the following standardised ventilator settings (SVS): VT=7 mL/kg PBW, PEEP=10 cm H2O and FiO2=0.5. When patients required PEEP>10 or FiO2>0.5 and could not tolerate a decrease in PEEP or FiO2 for maintaining the oxygenation target, a set of rules for setting PEEP and FiO2 were applied only during the SVS assessment (table 1). At other times, the PEEP and FiO2 levels were up to the discretion of the managing clinician. Blood gases were obtained 30 min after the setting adjustment. Based on the PaO2/FiO2 ratio at study entry, patients were categorised as moderate or severe ARDS according to the Berlin criteria. Based on PaO2/FiO2 values at 24 h, patients were reclassified into four groups: severe ARDS (PaO2/FiO2 ≤100 mm Hg), moderate ARDS (100<PaO2/FiO2≤200), mild ARDS (200<PaO2/FiO2≤300) and non-ARDS (PaO2/FiO2>300).
Rules for setting PEEP and FiO2 during assessment on standardised settings at 24 h of ARDS diagnosis
Outcome data
We sought to determine whether the use of the baseline PaO2/FiO2 for stratifying patients at ARDS onset results in the identification of subgroups of patients with a distinct degree of lung injury. We also examined whether patients categorised as severe or moderate ARDS based on their baseline PaO2/FiO2 could evolve to less severe forms of lung injury after 24 h of usual care. In addition, we determined whether the stratification of patients after 24 h of routine clinical care or at 24 h under SVS could identify groups of patients for each PaO2/FiO2 category with different severity and hospital mortality.
Statistical analysis
Data are expressed as percentage, mean±SD, or median and IQR. Differences between categorical variables were analysed by χ2 or Fisher's exact tests. For continuous variables, data were analysed using the t test, analysis of variance, Mann-Whitney or the Kruskall-Wallis tests, depending on their distribution and number of variables. To assess the agreement of patient classification between baseline (Berlin criteria) and the stratification at 24 h under standardised ventilator settings, the Cohen's κ coefficient (κ) was calculated for severe and moderate ARDS. We determined the predictive hospital mortality receiver operating characteristic (ROC) curve using the values of PaO2/FiO2 ratio in each patient and compared the overall performance of our model of stratification at 24 h of ARDS onset under SVS with the classification at baseline and at 24 h under non-standardised measurement of PaO2/FiO2 ratio. A p value <0.05 was considered statistically significant (two tailed). All statistical analyses were conducted using SPSS V.20.
Results
Although the published parent studies enrolled 452 patients, the present study included 26 additional patients who had been enrolled at the time of finalisation of both observational periods and were followed-up until hospital discharge. Thus, the present analysis included a total of 478 patients with ARDS with complete data.
Baseline characteristics of patients are displayed in table 2. Pneumonia, sepsis and trauma were the most common causes of ARDS. No significant differences were found in ventilation and oxygenation parameters at study entry between survivors and non-survivors, although non-survivors were older, had a higher APACHE II score and more organ dysfunctions (table 3). The overall hospital mortality was 42.2% (95% CI 37.8% to 46.6%). At study entry, most patients (305/478, 63.8%) had a baseline PaO2/FiO2>100 mm Hg but their FiO2 and PEEP levels varied widely ranging from 0.4 to 1.0 and from 5 to 20 cm H2O, respectively. Although patients initially categorised as severe ARDS had a higher overall hospital mortality than patients classified as moderate ARDS: 93/173 (53.7%, 95% CI 46.2% to 61.1%) vs 109/305 (35.7%, 95% CI 30.5% to 41.3%) (p=0.002), there were no significant differences in lung injury score, PEEP, VT and number of failing organs between severe and moderate ARDS when patients were classified using baseline PaO2/FiO2 (table 4).
Demographics, physiological and clinical parameters at study entry in 478 patients with moderate/severe ARDS
Baseline characteristics of 478 survivors and non-survivors with ARDS
Demographics, physiological and clinical parameters of 478 patients with ARDS categorised by the Berlin criteria (baseline PaO2/FiO2)
At 24 h of usual clinical care, PaO2 values recorded by physicians were also measured under a wide range of FiO2 (0.3–1) and PEEP [0 (only temporarily in 2 patients with bronchopleural fistula) to 22 cm H2O]. Based on those values, patients with a PaO2/FiO2≤100 had a hospital mortality of 53.0%, patients with a 100<PaO2/FiO2<200 had a mortality of 39.8%, patients with a 200<PaO2/FiO2<300 had a mortality of 39.8% and those with a PaO2/FiO2>300 had a mortality of 16.7% (p=0.064). When patients were reassessed under the SVS used in our study, PaO2/FiO2 values changed and moved patients from one category to another.
Despite 173 patients having a PaO2/FiO2≤100 mm Hg at ARDS onset, only 38.7% of them maintained the PaO2/FiO2≤100 mm Hg when assessed at 24 h under SVS (figure 1). Most patients diagnosed as severe ARDS by the Berlin criteria (106/173, 61.3%) were reclassified as moderate, mild and non-ARDS, when assessed after 24 h. Only 114 (23.8%) patients could not have their PEEP or FiO2 level decreased to 10 cm H2O and 0.5 at the time of assessment, and their assignment was based on the PaO2/FiO2 value under the clinician-selected PEEP and FiO2 settings. Cohen's κ analysis showed a very high disagreement between a patient's classification using Berlin criteria and assessment at 24 h under SVS: κ=0.03 for moderate ARDS and κ=0.29 for severe ARDS. Of note, 27.6% (132/478) of patients categorised at baseline as severe or moderate ARDS progressed with usual care to mild ARDS or non-ARDS when assessed under SVS, while 11.8% (36/305) of patients categorised as moderate ARDS by Berlin criteria progressed to severe ARDS when assessed under SVS. Significant differences for lung injury score, PEEP, plateau pressure, number of failing organs and VFDs were found in each category (table 5). Patients who evolved to non-ARDS were significantly younger than the other categories. Hospital mortality decreased 1.9–1.6-fold with every stage of PaO2/FiO2 severity. The lower the PaO2/FiO2 category, the higher the hospital mortality: 69/103 (67%, 95% CI 57.5% to 75.5%) vs 104/243 (42.8%, 95% CI 36.7% to 49.1%) vs 26/108 (24.1%, 95% CI 16.7% to 32.8%) vs 3/24 (12.5%, 95% CI 3.2% to 30%) for severe, moderate, mild and non-ARDS categories, respectively (p<0.000001) (table 6).
Demographics, physiological and clinical parameters of 478 patients with the acute respiratory distress syndrome (ARDS) at 24 h of ARDS onset after being categorised by assessment of PaO2/FiO2 on PEEP≥10 cm H2O with FiO2≥0.5
Mortality rates of 478 patients with ARDS when classified at baseline based on the values of PaO2/FiO2 at ARDS onset (Berlin criteria), after 24 h of usual care and at 24 h under a SVS

Flow diagram of the study. The percentages are a proportion of the total patients initially classified as moderate and severe, respectively. AECC, American-European Consensus Conference; ARDS, acute respiratory distress syndrome; PaO2/FiO2, ratio of arterial partial pressure of oxygen to fraction of inspired oxygen; PEEP, positive end-expiratory pressure; SVS, standardised ventilator setting.
Our model of risk stratification based on the measurement of PaO2/FiO2 under SVS outperformed risk stratification using baseline PaO2/FiO2 or non-standardised PaO2/FiO2 at 24 h. The area under the ROC curve for stratification at baseline was 0.583 (95% CI 0.525 to 0.636), at 24 h without standardisation it was 0.605 (95% CI 0.552 to 0.658), and at 24 h under SVS it was 0.693 (95% CI 0.645 to 0.742) (p<0.000001) (figure 2).

{kind=link}
{kind=link}
Receiver operating curves for risk assessment using the ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) ratio of each patient under standardised ventilator setting (SVS) at 24 h, and compared to risk stratification at ARDS onset (baseline) and at 24 h (T24) without standardising the measurement of PaO2/FiO2 values.
Discussion
Our present investigation in a large population of consecutive patients with moderate and severe ARDS who were managed with a low-VT strategy in the context of two observational studies revealed that: (1) the value of PaO2/FiO2 ratio at the time of ARDS diagnosis failed to identify subgroups of patients with a distinct degree of lung injury, and (2) a standardised ventilatory method based on preset PEEP and FiO2 levels is more precise than the use of PaO2/FiO2 at ARDS onset or after 24 h of usual care in assessing risk stratification of patients with ARDS. Our study suggests that patients within an identical PaO2/FiO2 range at baseline or after 24 h may not have similar degrees of lung injury or prognosis. We found that there was a marked PaO2/FiO2 variability within the first 24 h of ARDS diagnosis since patients could have the same range of PaO2/FiO2 but calculated under different levels of ventilatory support.
If assessment of ARDS severity is of crucial importance, it should be appropriate to set standardised rules for quantifying the severity of lung injury. The Berlin proposal of using the value of PaO2/FiO2 at the time of ARDS onset does not mandate standardisation of PEEP and FiO2 levels. The PaO2/FiO2 is generally calculated under a wide range of applied PEEP and FiO2, and can be easily manipulated by changing the PEEP and FiO2. Thus, if the measurement of PaO2 is not standardised, the calculated PaO2/FiO2 may mask the severity of the underlying lung pathology in a substantial proportion of patients. Although baseline PEEP could not predict outcome,11 ,14 baseline FiO2 does predict mortality.11 ,15 The key issue unmasked by our analyses is that many patients with severe lung disease evolved with usual care to less severe forms of lung injury within 24 h while others evolved to more severe forms of ARDS, as clearly demonstrated by the lack of concordance between the Berlin criteria and data at 24 h under SVS. The use of 24 h non-standardised PaO2/FiO2 was also inferior to PaO2/FiO2 assessment for risk stratification under SVS at 24 h. Since clinical practice introduces bias in the assessment of lung injury severity, our study clearly supports that it is the standardisation of ventilatory settings at 24 h that is crucial for appropriate stratification. Our model of risk stratification supports the fact that all cases of severe hypoxaemia are not ARDS. Patients whose oxygenation status changes dramatically in 24 h under a standardised assessment method would not be expected to have severe generalised lung inflammation as in ARDS, and should not be classified as ARDS.
Our findings have implications for clinical trials design and patient enrolment. ALI has a range of severity from mild pulmonary insult to full blown ARDS. The assessment of PaO2/FiO2 at 24 h after ARDS diagnosis on SVS can be used to insure a better categorisation of patients by disease severity. As our data suggest, the use of the Berlin criteria or the PaO2/FiO2 at 24 h under non-standardised conditions is inadequate for enrolling patients with similar degrees of lung injury into clinical trials. The use of baseline or non-standardised PaO2/FiO2 values for fast enrolment into therapeutic clinical trials may be responsible for patient selection bias, as a treatment that might benefit a subgroup of patients with ARDS is also tested in patients who are unresponsive to the experimental treatment. Some clinicians are concerned about a mandatory waiting period for reassessment of oxygenation before enrolling patients with ARDS into clinical trials.16 However, all trials performed to date in ARDS have enrolled patients within 24–72 h of ARDS onset17–22 and up to 7 days after meeting the AECC criteria.23 ,24 It is possible that similar results could be obtained if patients were assessed after 12 or 18 h of routine clinical care, but our study design precludes us to speculate further. It is well accepted that in a high proportion of patients, lung function improves dramatically within the initial 24 h of usual care. Also, it is likely that within the initial 24 h, patients are not stable when routine therapies (ie, fluid resuscitation, sedation, muscle paralysis, antibiotics, insulin, catecholamine, blood transfusion, body positioning, intravascular catheterisation, repetitive and aggressive suctioning or secretions, insertion of chest tubes, selection of the best ventilatory pattern, etc) are implemented.
This study demonstrated that risk stratification of patients with ARDS based on PaO2/FiO2 ratios recorded at ARDS onset or diagnosis (baseline) or measured without standardising PEEP and FiO2 after 24 h of usual care, is not clinically useful. If patients in a trial have a low risk of the condition that the intervention is hypothesised to prevent, the trial will not demonstrate the efficacy of the intervention, regardless of the trial size.25 Stratification of enrolled patients can reduce the necessary sample size, since it makes larger treatment effects easier to detect.26 That could explain why only one randomised controlled trial in patients with ARDS has been positive27 since the publication of the ARDS net trial. In that study, only patients with a PaO2/FiO2 threshold that persisted after 12–24 h under a specific level of PEEP and FiO2 were enrolled. Recent high-frequency ventilation trials have been either ineffective or worse than usual care,28 ,29 potentially due to a patient selection bias: both trials enrolled patients based on baseline PaO2/FiO2. These trials support the importance of PaO2/FiO2 assessment after 24 h of making the initial diagnosis of ARDS. If severe ARDS is characterised by profound hypoxaemia that responds to traditional management, our findings demonstrated that a high rate of misclassification occurred because patients were not reassessed after 24 h of usual care when many patients responded to a stepwise escalation of traditional therapies. If patients are identified as severe ARDS by the Berlin criteria only, they could be forced to receive highly invasive and aggressive therapies that provide no benefit (useless) or could be harmful (worse than usual care), since after 24 h of usual care a high percentage of patients have milder forms of ARDS. We would recommend attempting to enrol patients who met the Berlin definition at ARDS onset but only randomising those patients who sustained the desired level of injury after 24 h of usual care while confirming established hypoxaemia on SVS.
In an attempt to validate the modification of the AECC ARDS definition by the Berlin criteria, Hernu et al30 and Caser et al31 found that neither definition was able to identify subgroups with different levels of lung injury based on non-standardised baseline PaO2/FiO2 values. Those studies reported that the Berlin criteria were incapable of separating patients into distinct categories of severity with significantly different mortalities. Furthermore, a recent autopsy study revealed that the Berlin criteria did not correlate with the presence of diffuse alveolar damage in more than 50% of patients categorised as moderate and severe ARDS.32 However, this correlation improved significantly only when patients met PaO2/FiO2 criteria beyond 24 h of persistence of ARDS criteria. Despite the fact that changes in the applied FiO2 and PEEP induce profound variations in PaO2/FiO2,9 ,33 by leaving the assessment of PaO2/FiO2 criteria essentially unchanged, the AECC definition and the Berlin criteria are essentially identical.2 ,34 The requirement of a minimum PEEP level of 5 cm H2O has no impact on the definition9 since it is hard to conceive that an patient with ARDS would be managed with PEEP<5 cm H2O.19
Our study has several strengths. First, our study design included all consecutive patients who met the criteria for moderate and severe ARDS, so we believe that our patients closely represented routine patients with ARDS. Second, patients were enrolled in a multidisciplinary network of teaching hospitals, not just one institution. Third, our stratification approach outperformed categorisation at baseline and categorisation at 24 h without standardisation of the measurement of PaO2/FiO2. On the other hand, we acknowledge a couple of limitations to this study. First, we did not enrol patients with mild ARDS under the Berlin criteria (PaO2/FiO2>200mm Hg). However, we do not believe that the exclusion of these patients weakens our results. Those meeting criteria for mild ARDS constitute a very heterogeneous group of patients who are usually underdiagnosed, representing a case-mix in which many do not require endotracheal intubation and invasive MV. Also, since PaO2/FiO2 values in patients under non-invasive MV are not comparable with those on conventional MV, it is not clear whether patients meeting criteria for mild ARDS on non-invasive ventilation would meet those criteria after intubation and conventional MV. However, we are confident that no patients with mild ARDS were excluded during our observational periods if they moved to a more severe category, although we do not have data on the precise number of these patients. Second, we cannot expect our approach of risk stratification to hold for patients ventilated in a non-lung protective manner since it is clear that ventilation with large VT and high end-inspiratory plateau pressures causes ventilator-induced lung injury in addition to the pre-existing ARDS, and we do not expect our approach to predict outcomes in this setting.
In conclusion, the stratification of patients with ARDS based on the value of PaO2/FiO2 ratio at the time of ARDS diagnosis, as proposed by the Berlin criteria, or based on the non-standardised value of PaO2/FiO2 at 24 h after usual clinical care, is not useful for assessing severity of lung injury or for enrolling appropriate patients with ARDS into clinical trials. Assessment of ARDS should be a two-step process. The initial assessment at ARDS onset followed by a second assessment at 24 h under SVS represents a better method for optimising risk stratification of patients with ARDS. Since there is no biomarker to identify patients as having ARDS or to identify the severity of illness, we must continue to search for methods to better define and stratify ARDS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators Additional investigators (collaborators) from the SIESTA Network are listed in the online supplementary appendix.
-
Contributors JV and RMK contributed to the initial study concept and design. JB, RdC, DA-O, FJD-D, AM, VC, FS-S, CT, EG-H, JL, LB and RLF contributed to the final study design. JB, RdC, DA-O, FJD-D, AM, VC, FS-S, CT, EG-H, JL and LB contributed with data collection. JV, RLF, LP-M and RMK analysed and interpreted the data. RLF, LP-M and JV performed the statistical analysis. JV and RMK drafted the article and all other authors critically revised it for important intellectual content. JV, LP-M and RLF had full access to all the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analyses. All authors gave final approval of the manuscript version to be published.
-
Funding JV obtained grants from the Instituto de Salud Carlos III, Madrid, Spain (PI 07/0113, PI10/0393, CB06/06/1088) and Asociación Científica Pulmón y Ventilación Mecánica, Las Palmas, Spain. All researchers are independent of the funding bodies.
-
Competing interests JV has received research grants from Maquet. RMK is a consultant for Covidien and has received honorarium from Maquet for lecturing.
-
Ethics approval The study was conducted in accordance with the amended Declaration of Helsinki and approved by the Ethics Committees at the coordinating centres [Hospital Universitario NS de Candelaria, Tenerife, Spain (#2004/22), Hospital Universitario Dr Negrín, Las Palmas, Spain (#2008/1029) and Hospital Virgen de La Luz, Cuenca, Spain (#2008/0715)].
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.