Article Text

Abstract
Objective: To determine the agreement between arterial and venous samples in a pathologically diverse patient population presenting at an emergency department (ED) with a view to obviating the need for arterial blood gas (ABG) analysis in initial ED evaluation.
Methods: Prospective study of 95 patients (69 males, 26 females, mean (SD) age 52 (1.6) years) with diverse medical conditions, presenting at a tertiary health centre ED and deemed by the treating physician to require an ABG analysis. Arterial and venous samples for gas analysis were taken as close in time to each other as possible. The data thus obtained were analysed for agreement between pH, Pco2, Po2 and bicarbonate using the Bland–Altman method.
Results: The arterial and venous values of pH, bicarbonate and Pco2 show acceptably narrow 95% limits of agreement using the Bland–Altman method (0.13 to −0.1, 4.3 to −5.8 and 6.8 to −7.6, respectively). Agreement in Po2 measurements was poor (95% limits of agreement 145.3 to −32.9).
Conclusion: Venous blood gas analysis for pH, bicarbonate and Pco2 may be a reliable substitute for ABG analysis in the initial evaluation of an adult patient population presenting to the ED.
- ABG, arterial blood gas
- ED, emergency department
- Pco2, partial pressure of carbon dioxide
- Po2, partial pressure of oxygen
- VBG, venous blood gas
Statistics from Altmetric.com
- ABG, arterial blood gas
- ED, emergency department
- Pco2, partial pressure of carbon dioxide
- Po2, partial pressure of oxygen
- VBG, venous blood gas
Arterial blood gas (ABG) analysis is commonly performed for clinical evaluation, but the procedure has certain limitations in the form of reduced patient acceptability (because the procedure can be painful) and the potential to cause complications such as arterial injury, thrombosis with distal ischaemia, haemorrhage, aneurysm formation, median nerve damage and, rarely, reflex sympathetic dystrophy.1,2 Venous blood gas (VBG) analysis is a relatively safer procedure as fewer punctures are required, thus also reducing the risk of needle stick injury to the health care worker.
Although various studies suggest that a venous sample is relatively accurate for acid–base assessment,3–9 VBG analysis has not gained much acceptance as a substitute for ABG analysis.
The present study attempts to describe the agreement between arterial and venous blood values (pH, bicarbonate, partial pressures of carbon dioxide (Pco2) and oxygen (Po2)) in order to determine whether VBG could replace ABG in the initial assessment of adult patients in an ED where diverse pathological conditions are encountered.
PATIENTS AND METHOD
A convenience sample of adult patients presenting to the ED of a tertiary care 1000 bed teaching hospital in Northern India, from September to December 2006, were enrolled. Patients were eligible if the on-duty emergency physician decided to obtain an ABG sample for the initial assessment. After having the study explained, a verbal consent was obtained from the patient or the relative, and patients were sampled for arterial and venous blood with minimum delay (always <2 min) between the samples. For arterial samples (0.5–1 ml), a minimally heparinised plastic syringe with 24 G needle was used to puncture the radial artery. For venous sampling, blood was obtained at the time of intravenous cannula placement or using peripheral venepuncture. The two samples were taken as close as possible in time and before the initiation of any form of treatment. The samples were analysed as quickly as possible using the blood gas analyser located in the ED.
Data were analysed using SPSS version 10.0.1.299 and Prism 5 for Windows (Graph pad, version 5). The Bland-Altman method was used to calculate agreement between arterial and venous measurements.
The study was approved by the ethics committee of the All India Institute of Medical Sciences, New Delhi, India.
RESULTS
The study involved 95 patients (69 males, 26 females, mean (SD) age 52 (1.6) years).The presenting diagnosis of the patients were: chronic obstructive airway disease (17.9%), pneumonia (17.8%), sepsis (15.8%), acute on chronic renal failure (10.5%), acute coronary syndrome (9.4%), diabetic ketoacidosis (8.4%), systemic malignancy (7.4%), acute gastroenteritis (6.3%), systemic lupus (4.2%), and suspected organophosphorus or phosgene poisoning (2.2%). Three patients (3.2%) had hypotension (systolic pressure <90 mm Hg) at presentation. Table 1 shows the mean ABG and VBG values of the four parameters measured and their 95% limits of agreement.
Results of arterial and venous blood gas analyses (n = 95)
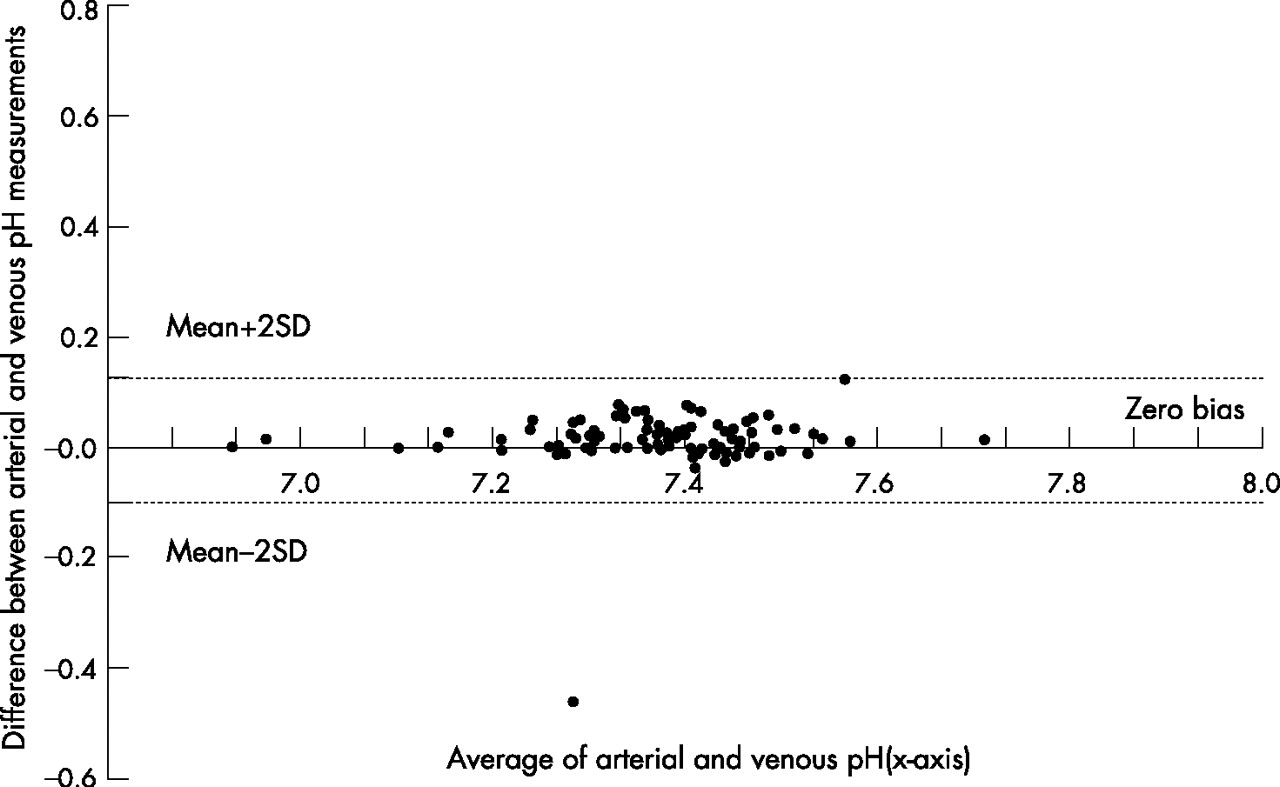
As shown in the bias plots (figs 1, 2 and 3), there is acceptable agreement between the arterial and venous values of pH, Pco2 (mm Hg) and bicarbonate (mEq/l), respectively, and poor agreement in Po2 (mm Hg, fig 4).

Bland-Altman plot of arterial and venous blood pH showing the 95% limits of agreement.

Bland-Altman plot of arterial and venous blood pO2 showing the 95% limits of agreement.

Bland-Altman plot of arterial and venous blood bicarbonate showing the 95% limits of agreement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bland-Altman plot of arterial and venous blood pCO2 showing the 95% limits of agreement.
DISCUSSION
There is plenty of reported evidence on agreement in ABG and VBG values.3–9 Still, the popularity of VBG is low and few studies have even expressed reservations regarding the accuracy of VBG values in patient evaluation.7,10,11 The present study was carried out to determine whether VBG values can replace ABG values (pH, bicarbonate, Pco2 and Po2) in the initial ED evaluation of patients.
As shown in the results, agreement is excellent in pH values (95% limits of agreement 0.13 to −0.1), and acceptably narrow in Pco2 and bicarbonate values. In the present study, values in Pco2 show better agreement than reported earlier.7 As expected, venous Po2 and arterial Po2 did not show good agreement in our study.
Most of the previous studies have either sampled only specific patient groups (for example, diabetic ketoacidosis and renal failure) or if they sampled a diverse patient population, the presenting diagnosis was not explicitly stated and not all commonly used parameters were analysed. The diverse pathology profile and the parameters studied in the present study are more likely to be encountered in a typical ED.
One limitation of the study is that it did not strictly involve random patient recruitment, as the patient enrolment was based on convenience and availability of the investigator. This, however, is unlikely to have introduced any systemic bias in the patient profile sampled, which includes most presentations in a typical ED setting. Another limitation is that only two of the patients had severe acidosis (pH <7) and so agreements at the extremes of pH cannot be estimated from this study.
In conclusion, venous pH, bicarbonate and Pco2 estimation can replace ABGs in initial ED assessment.
Acknowledgments
We are thankful to the physicians and nursing staff of the New Emergency Ward, All India Institute of Medical Sciences, New Delhi, for their support.
REFERENCES
Footnotes
-
Sources of funding: None
-
Conflicts of interest: The authors G Malatesha, Nishith K Singh, Ankur Bharija, Bhavya Rehani and Ashish Goel have no interests to declare