Article Text

Abstract
Objective: To evaluate the safety and prognostic capacity of cardiopulmonary exercise testing in patients ≥ 60 years old who are hospitalised with heart failure caused by left ventricular dysfunction.
Design: Prospective study.
Setting: University hospital.
Patients: Study participants were 67 patients (66% men) with clinical heart failure stabilised on medical treatment. The study is a part of a nursing intervention study. Mean (SD) age was 74 (6) years, New York Heart Association functional class II–III, and ejection fraction 0.36 (0.11).
Interventions: Cardiopulmonary exercise testing and echocardiography.
Main outcome measures: Peak oxygen consumption (V̇o2), peak ventilatory equivalents for carbon dioxide (V̇E/V̇co2) and oxygen (V̇E/V̇o2), left ventricular volumes, and mortality.
Results: Mean (SD) peak V̇o2 was 11.7 (3.7) ml/kg/min, peak V̇E/V̇co2 43 (9), and peak V̇E/V̇o2 46 (11). During 12–59 months of follow up, 14 patients died. In univariate analyses peak V̇o2, V̇E/V̇o2, and V̇E/V̇co2 were all strongly related (p < 0.01) to mortality. In a multivariate Cox regression analysis, peak V̇E/V̇co2 was the strongest predictor of mortality (p < 0.001), followed by left ventricular end systolic volume (p < 0.001). A cut off of peak V̇E/V̇co2 at ≥ 45 gave a univariate hazard ratio of 6.7 for death during follow up. No adverse events occurred during the exercise test.
Conclusion: These findings extend results found in selected middle aged patients to elderly patients with heart failure and show that ventilatory parameters from a cardiopulmonary exercise test, such as peak V̇o2, V̇E/V̇o2, and V̇E/V̇co2 are powerful predictors of mortality.
- heart failure
- exercise testing
- ventilatory parameters
- prognosis
- AVPD, atrioventricular plane displacement
- EF, ejection fraction
- NYHA, New York Heart Association
- OPTIMAL, optimising congestive heart failure outpatient clinical project
- V̇co2, carbon dioxide production
- V̇E, ventilatory equivalent
- V̇o2, oxygen consumption
Statistics from Altmetric.com
- AVPD, atrioventricular plane displacement
- EF, ejection fraction
- NYHA, New York Heart Association
- OPTIMAL, optimising congestive heart failure outpatient clinical project
- V̇co2, carbon dioxide production
- V̇E, ventilatory equivalent
- V̇o2, oxygen consumption
The prevalence of heart failure is increasing throughout the western world because the population is aging and management of patients suffering from acute coronary syndromes and their late complications is improving.1–3 Heart failure is associated with a high mortality rate, in particular in New York Heart Association (NYHA) functional classes III–IV. Indeed, one year after hospital discharge for treatment of heart failure, approximately 30% of the patients have died.4,5 Improvement in diagnostic procedures and the development of new drugs make it possible to tailor the treatment of heart failure in the individual patient. To do this and to monitor prognosis, functional assessment of patients with heart failure is of great importance. The classification of heart failure according to NYHA functional class provides a rough estimate of the physical status of the patient in activities of daily life and has been shown to be a useful predictor of mortality.6 The NYHA classification does not, however, provide objective measurement of physical capacity. The six minute walk test does not relate to cardiac function and relates only moderately to exercise capacity.7 In contrast, the cardiopulmonary exercise test gives important additional information by providing ventilatory parameters, such as oxygen uptake (V̇o2) and the ventilatory equivalents for oxygen (V̇E/V̇o2) and carbon dioxide (V̇E/V̇co2), at submaximal and at peak exercise. Previous studies have shown that patients with heart failure reach their anaerobic threshold at an earlier stage than healthy controls and that their peak V̇o2 is lower.8,9 However, the use of a cardiopulmonary exercise test has been restricted mainly to the prognostic evaluation of middle aged patients, often on the waiting list for a heart transplant.10
We hypothesised that the cardiopulmonary exercise test can provide useful prognostic information to a broader population of patients with heart failure. Thus, this study aimed at evaluating whether the test can be carried out safely and give information on the prognosis in a population representative of hospitalised patients with heart failure.
METHODS
Study design
The OPTIMAL (optimising congestive heart failure outpatient clinic project) is a prospective study in 208 patients hospitalised with heart failure between January 1996 and December 1999 in our institution. Participants were > 60 years old with heart failure (NYHA class II–IV) and left ventricular systolic dysfunction by echocardiography, defined as ejection fraction (EF) < 0.45 or atrioventricular plane displacement (AVPD) < 10 mm. Exclusion criteria were valve stenosis, an acute myocardial infarction or unstable angina pectoris within the previous three months, dementia, severe chronic lung disease, or other severe concomitant disease. In all, 285 patients were screened for participation in the study. Of those, 77 patients were not included in the study as they did not wish to participate (n = 32), did not have systolic dysfunction at screening echocardiography (n = 23), had valve stenosis (n = 5) or a recent ischaemic event (n = 4), or suffered from dementia (n = 4) or from other severe concomitant disease (n = 9).
The patients were randomly assigned to follow up in a nurse based outpatient clinic at the hospital or to conventional follow up and treatment, usually in primary care. The primary end point of the study is to assess whether a nurse based outpatient clinic leads to improvement of quality of life. Evaluation of cardiac function, morbidity, and mortality are secondary end points.
After stabilisation of their heart failure, all patients were asked to perform a cardiopulmonary exercise test with metabolic monitoring before discharge. We here report on the 67 subjects in this elderly population who underwent the test. The main reasons not to perform the exercise test (n = 141) were unwillingness to participate in the test (n = 46), other conditions such as asthma, blindness, and temporary confusion (n = 42), other diseases of the cardiovascular system such as arrhythmias, angina, and stroke (n = 21), non-availability of exercise equipment (n = 21), and joint diseases (n = 11).
Outcome on all cause mortality was determined from death certificates when all patients had a follow up of at least one year. Each patient gave informed consent to participate in the study, which was approved by the local ethics committee and conforms to the principles outlined in the Declaration of Helsinki.
Exercise test and protocol
The exercise test was performed on an electrically braked bicycle. The equipment used was a cardiopulmonary exercise system (Medical Graphics, St Paul, Minnesota, USA) for breath by breath measurements of V̇E, V̇o2, and V̇co2. Derived entities such as V̇E for O2 and CO2 (V̇E/V̇o2, V̇E/V̇co2), the respiratory quotient V̇co2/V̇o2, and respiratory rate per minute were presented on line. The equipment was calibrated before every test. A 12 lead ECG was monitored for possible arrhythmia and ST segment changes. The test began with two minutes of sampling at rest and was followed by two minutes of freewheeling exercise. A ramp test with a continuos increase of workload by 10 W/min was chosen. The exercise test was symptom limited, using a Borg scale from 0 to 10 for dyspnoea, fatigue, and chest pain.11 The patients were encouraged to exercise until they were exhausted. The physician interfered according to standard criteria. Blood pressure and heart rate were measured every other minute. All respiratory parameters were measured from plots over time, giving moving average values. Peak V̇o2, V̇E/V̇o2, and V̇E/V̇co2 were calculated as the last value of three during the last 30 seconds of exercise. If this last value was not the highest, the mean of the last three values was calculated. Slopes of V̇E/V̇o2 and V̇E/V̇co2 were calculated by linear regression analysis. The anaerobic threshold was calculated by the V slope method.12
Echocardiography
All examinations were performed with an Acuson 128 XP/10 (Mountain View, California, USA) with a 2.5–4.0 MHz (V4c) probe and the patient in the left semilateral position. Recordings were stored on videotape and analysed at the end of the study. Left ventricular dimensions in diastole and systole were measured by M mode technique. The EF was calculated according to the recommendations of the American Society of Echocardiography.13 Biplane volumes were calculated from area tracings using the disc summation method (modified Simpson's rule). Left ventricular systolic function was also evaluated with the AVPD method.14 The displacement was measured by M mode from an apical window. Mean values from four sites and three beats or more were used and the overall mean was calculated. Patients were enrolled into the study if a screening echocardiographic examination after medical stabilisation showed systolic dysfunction, defined as EF < 0.45 or AVPD < 10 mm. These measurements were not used further in the study. All echocardiographic findings presented in this paper are from an extensive baseline investigation, sometimes performed a few days after screening.
Statistical procedures
Data are presented as frequencies, median or mean (SD), as appropriate. The χ2 test was used for comparison of proportions. For correlations, Pearson's product–moment method was used. Survival curves were generated by the Kaplan-Meier method and the log rank test was used to assess differences in outcome between groups. The prognostic power of the variables for mortality was evaluated by Cox proportional hazard survival analysis, performed with Statistica 5.5 software (StatSoft, Tulsa, Oklahoma, USA) by a stepwise procedure. Hazard ratios and 95% confidence intervals were calculated, when appropriate. The final model was adjusted for age, sex, and NYHA functional class. A probability value of p < 0.05 was considered significant.
RESULTS
Table 1 gives demographic characteristics and medication of the patients who underwent exercise testing. The mean daily doses at baseline of angiotensin converting enzyme inhibitors were 55 mg of captopril, 4 mg of ramipril, and 14 mg of enalapril. The mean daily furosemide dose was 128 mg. When the study group was compared with the remaining patients in the entire OPTIMAL study who did not perform a cardiopulmonary exercise test, the latter group were somewhat older but the groups were otherwise comparable.
Demographic data at baseline (n=67)
Cardiopulmonary exercise test
Table 2 and fig 1 show the results of the exercise test of 67 patients. No adverse events occurred during the tests. The anaerobic threshold was not always reached or possible to detect but was determined in 49 patients (73%). The peak respiratory quotient was > 1 in 53 patients (79%). While V̇E/V̇o2 increased between the anaerobic threshold and the maximal effort, the corresponding V̇E/V̇co2 was relatively unchanged throughout the test. Table 2 shows that the anaerobic threshold was reached at approximately 30% of peak work rate. The threshold probably is low because some patients (n = 13) reached the anaerobic threshold very early, during the two minutes of rest on the bicycle or the following two minutes working without load. All of these 13 patients continued to exercise, though, reaching a mean peak work load of 51 W. Forty eight patients chose to stop the test because of exhaustion (n = 21), dyspnoea (n = 14), or both in combination (n = 13). The physician discontinued the test because of a fall in blood pressure (n = 12), angina pectoris or arrhythmia in one patient each, and pronounced ST segment depression in the remaining five subjects. The physician did not stop any test because of conductance disorders or depressed heart rate responses.
Results from the cardiopulmonary exercise test

Relations between mortality and peak oxygen uptake (peak V̇o2), peak work load, and the quotients of ventilation to oxygen uptake (V̇E/V̇o2) and ventilation to carbon dioxide production (peak V̇E/V̇co2). Mean values for 67 patients.
Echocardiography
The baseline ejection fraction was 0.36 (0.11) and atrioventricular plane displacement 6.9 (2.0) mm. The baseline left ventricular end systolic diameter was 47 (13) mm, left ventricular end diastolic diameter 57 (10) mm, end systolic volume 89 (51) ml, and end diastolic volume 132 (61) ml. Table 3 shows echocardiographic characteristics in relation to mortality. Table 4 shows the correlations between ventilatory and echocardiographic data. The strongest correlation was between peak V̇o2 and atrioventricular plane displacement.
Characteristics of surviving and non-surviving patients at follow up
Correlations between ventilatory and echocardiographic variables
Predictors of survival
Table 3, fig 1, and fig 2 show patient characteristics, and exercise and echocardiographic results in relation to mortality in December 2000, when all patients had been followed up for at least one year. During follow up 14 patients died (median survival 11.8 months). Median follow up time for the survivors was 30.8 months. In univariate analyses, mortality was positively related, in declining order of significance, to peak V̇E/V̇co2 (50.8 v 40.9, p < 0.001), peak V̇E/V̇o2 (54.9 v 43.3, p < 0.001), slope V̇E/V̇o2 (46.8 v 39.7, p = 0.006), and slope V̇E/V̇co2 (49.7 v 43.8, p = 0.02), and inversely related to peak V̇o2 (9.3 v 12.4 ml/kg/min, p = 0.004). As expected, peak and slope V̇E/V̇o2 (r = 0.8) and V̇E/V̇co2 (r = 0.9) were highly correlated. Thus, in univariate analysis, peak V̇E/V̇co2 and V̇E/V̇o2 were stronger prognostic predictors than slope. Furthermore, a low ejection fraction (p < 0.05) and large left end systolic (p < 0.001) and end diastolic (p < 0.05) ventricular volumes predicted mortality. The strongest univariate predictor of mortality in Cox regression analysis was peak V̇E/V̇co2, (Wald χ2 = 15.3, p < 0.001), followed by peak V̇E/V̇o2 (Wald χ2 = 11.7, p < 0.001) and left ventricular end systolic volume (Wald χ2 = 11.0, p < 0.001). In the final multivariate model, peak V̇E/V̇co2 was the strongest independent prognostic predictor (Wald χ2 = 11.3, p < 0.001), followed by left ventricular end systolic volume (Wald χ2 = 10.6, p = 0.001) when adjusted for age, sex, and NYHA class (global χ2 = 30.3, p < 0.001). Peak V̇o2 had no independent prognostic value in addition to either peak V̇E/V̇co2 or left ventricular end systolic volume.
{kind=link}
{kind=link}
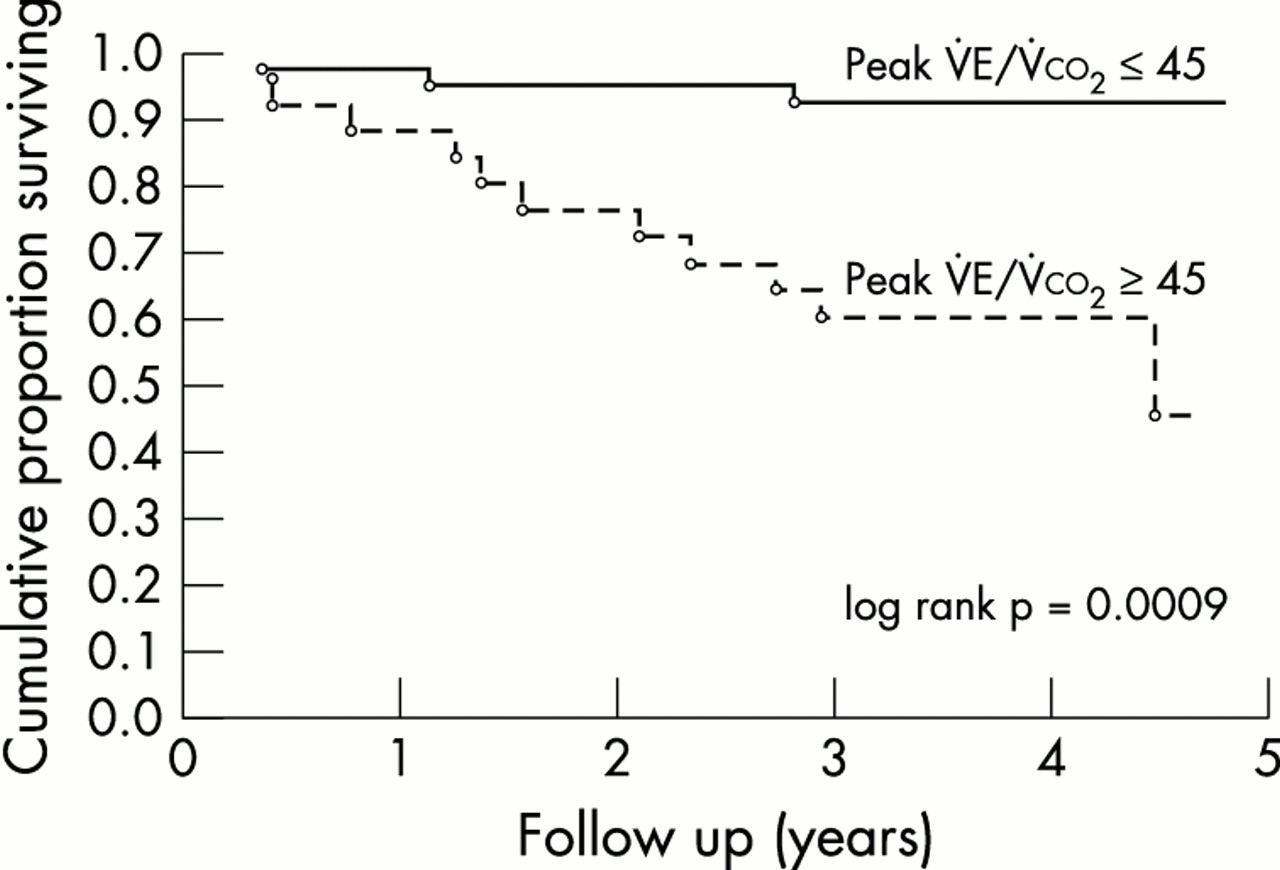
Kaplan-Meier survival curve with a V̇E/V̇co2 cut off of ≥ 45. Odds ratio 6.7 (95% confidence interval 1.9 to 24.2).
With a cut off for peak V̇E/V̇co2 of ≥ 45, the univariate hazard ratio of survival was 6.7 (95% confidence interval 1.9 to 24.2, log rank p < 0.001) (fig 2). Adjusted for age, sex, left ventricular end systolic volume, and NYHA class, the hazard ratio of survival was 4.3 (p < 0.05). Sensitivity was 79% for mortality, specificity was 70%, the positive predictive value was 44%, the negative predictive value was 92%, and the positive likelihood ratio was 2.6. We did not find age, sex, aetiology of heart failure, presence of atrial fibrillation, or medication to have an impact on mortality.
DISCUSSION
The present prospective study is the first to assess the usefulness of a cardiopulmonary exercise test in elderly patients hospitalised with heart failure. We found peak V̇o2 to be severely impaired among these patients, reaching only 62% of the predicted value. The peak V̇E/V̇co2 reached high values and was the strongest predictor of mortality in univariate and in multivariate analyses. Our finding support and extend recent observations by Davies et al from exercise testing in ambulatory elderly patients with heart failure.15 They included patients with a mean age of 75.9 years and found a mean peak V̇o2 of 15.2 ml/kg/min, a mean slope V̇E/V̇co2 of 38.7, and both to predict the prognosis. The slightly better performance in their patients probably is a result of the difference between ambulatory and hospitalised patients with heart failure. Indeed, peak V̇o210 and other measurements, particularly V̇E/V̇co2, have been shown to predict mortality in patients with heart failure.16–18 In a study of 60 male patients with heart failure in NYHA class II and III, Bol et al found that the slope of V̇E/V̇o2 was the strongest prognostic predictor of all cause mortality.19 Both peak and slope V̇E/V̇o2 and V̇E/V̇co2 have been used. It may be argued that slope is less effort dependent, as the peak depends on the level of exercise. In our study, however, the predictive power of the peak value was stronger.
Mancini et al divided middle aged patients with heart failure into four classes according to the cardiopulmonary exercise test results of peak V̇o2.10 Not always compatible with the NYHA classes, this classification has been shown to be useful as a prognostic tool for patients on the waiting list for a heart transplant. Thus, a patient with peak V̇o2 > 14 ml/kg/min has a good prognosis and can often be deferred from the transplant waiting list. Interestingly, when we applied this cut off to our subjects representing a different group of patients with heart failure, we found 95% survival in subjects with peak V̇o2 > 14 ml/kg/min. However, our results show that peak V̇E/V̇co2 provides the strongest predictive information. Thus, in a multivariate analysis also including left ventricular end systolic volume, we show V̇E/V̇co2 to be superior. A cut off for V̇E/V̇co2 of ≥ 45 may be most useful in assessing mortality risk in clinical practice.
The prognostic value of echocardiography in elderly patients with heart failure is unclear. Taffet et al showed that in male patients with heart failure who were 75 years or older, the ejection fraction was not related to one year survival.20 However, many elderly patients may have heart failure caused by diastolic dysfunction and systolic function is often preserved.21 In the present study, confined to patients with systolic left ventricular dysfunction, left ventricular end systolic volume was an independent strong prognostic indicator. Furthermore, there was a correlation between ventilatory variables and echocardiographic findings, in particular systolic left ventricular function. Few studies have investigated relations between V̇o2 and echocardiographic findings. In the study of Bol et al19 the combination of a high V̇E/V̇o2 slope and a relatively high left ventricular ejection fraction was particularly unfavourable for prognosis. Florea et al described changes in peak V̇o2 but not ejection fraction over time to predict outcome.22 In another study in middle aged patients with dilated cardiomyopathy, peak V̇o2 correlated with left ventricular dimensions, filling patterns, and ejection fraction.23 Thus, left ventricular size and in particular end systolic volume provide independent prognostic information in elderly patients with heart failure, whereas ejection fraction fails to do so in this context. However, peak V̇E/V̇co2 provides stronger prognostic information.
There are potential limitations to this study. Firstly, only one in three of these elderly hospitalised patients with heart failure eventually performed the cardiopulmonary exercise test. Cardiac patients unable to perform a provocation test probably have a worse prognosis.24 This would decrease the predictive value of the provocation test in the current study. In our study, the patients who underwent the cardiopulmonary exercise test had a prognosis similar to those of the other patients in OPTIMAL. Secondly, this study included only patients with systolic left ventricular dysfunction. The prognostic information of the cardiopulmonary exercise test in patients with diastolic dysfunction remains to be studied.
The cardiopulmonary exercise test has been used for several years in middle aged patients, often on the transplant waiting list. We show that it can be used safely in elderly hospitalised patients with heart failure and can provide strong and independent prognostic information.
Acknowledgments
This study was supported by The Swedish Society of Medicine, Karolinska Institutet, The Vardal Foundation, and the Swedish Heart-Lung Foundation. The authors are grateful to Ms Margret Lundström, and Ms Inger Bergbom for technical assistance.