

Abstract
To minimize ventilator-induced lung injury, attention should be directed toward avoidance of alveolar over-distention and cyclical opening and closure of alveoli. The most impressive study of mechanical ventilation to date is the Acute Respiratory Distress Syndrome (ARDS) Network study of higher versus lower tidal volume (VT), which reported a reduction in mortality from 39.8% to 31.0% with 6 mL/kg ideal body weight rather than 12 mL/kg ideal body weight (number-needed-to-treat of 12 patients). To achieve optimal lung protection, the lowest plateau pressure and VT possible should be selected. What is most important is limitation of VT and alveolar distending pressure, regardless of the mode set on the ventilator. Accumulating observational evidence suggests that VT should be limited in all mechanically ventilated patients—even those who do not have ALI/ARDS. Evidence does not support the use of pressure controlled inverse-ratio ventilation. Although zero PEEP is probably injurious, an area of considerable controversy is the optimal setting of PEEP. Available evidence does not support the use of higher PEEP, compared to lower PEEP, in unselected patients with acute lung injury (ALI)/ARDS. However, results of a meta-analysis using individual patients from 3 randomized controlled trials suggest that higher PEEP should be used for ARDS, whereas lower PEEP may be more appropriate in patients with ALI. PEEP should be set to maximize alveolar recruitment while avoiding over-distention. Many approaches for setting PEEP have been described, but evidence is lacking that any one approach is superior to any other. In most, if not all, cases of ALI/ARDS, conventional ventilation strategies can be used effectively to provide lung-protective ventilation strategies.
- acute lung injury
- ALI
- acute respiratory distress syndrome
- ARDS
- lung-protective ventilation strategies
- mechanical ventilation
- PEEP
- ventilator-induced lung injury
Introduction
Many lives have been saved by the use of mechanical ventilation. But after years of targeting ventilation strategies to normalize arterial blood gases, it was realized that these strategies might result in ventilator-induced lung injury (VILI). Lung-protective ventilation strategies have recently received increasing attention and are now considered standard practice. There are 2 principal causes of VILI: alveolar over-distention, and cyclical opening and closing of alveoli. Injurious ventilation strategies cause increased permeability of the alveolar-capillary membrane and increased production of pro-inflammatory mediators within the lungs. Leakage of the inflammatory mediators into the bloodstream can result in downstream organ system failures, which can lead ultimately to multiple organ failure and death.1–6 Lung-protective ventilation strategies are directed primarily toward volume and pressure limitation during the inspiratory phase and maintenance of alveolar recruitment during the expiratory phase. The purpose of this paper is to review the evidence supporting lung-protective ventilation using conventional ventilation strategies.
Volume and Pressure Limitation
The ARDS Network Higher Versus Lower Tidal Volume Study
In the late 20th century, many experimental studies were published suggesting benefit from tidal volume (VT) limitation.7 Several patient studies reported that VT limitation was safe,8–10 and a single-center study from Brazil found that inspiratory volume and pressure limitation with higher PEEP was associated with a survival benefit.11 This led to funding by the National Institutes of Health for the Acute Respiratory Distress Syndrome (ARDS) Network to study ventilation with lower VT, as compared with traditional VT, for patients with acute lung injury (ALI) and ARDS.12,13 Patients were recruited from March 1996 through March 1999 at 10 university hospitals in the United States. Volume controlled continuous mandatory ventilation was used and VT was set based on ideal body weight (IBW). In the group treated with traditional VT the target VT was 12 mL/kg IBW. This was subsequently reduced, if necessary, to maintain plateau pressure (Pplat) ≤ 50 cm H2O. In the group treated with lower VT, the target VT was reduced to 6 mL/kg IBW and subsequently reduced, as necessary, to maintain Pplat ≤ 30 cm H2O. The minimum VT was 4 mL/kg IBW. If Pplat dropped below 25 cm H2O, VT was increased in steps of 1 mL/kg IBW until Pplat was at least 25 cm H2O or the VT was 6 mL/kg IBW. For patients with severe dyspnea, the VT could be increased to 8 mL/kg IBW.
The results of the ARDS Network study are impressive—perhaps the most impressive of any study of mechanical ventilation to date. The trial was stopped after the enrollment of 861 patients because mortality was lower in the group treated with lower VT than in the group treated with traditional VT (31.0% vs 39.8%, P = .007). Translated to the metrics of evidence-based medicine, the number of patients needed to treat with the lower VT to avoid a single death is 12 patients. The number of ventilator-free days during the first 28 days after randomization was greater in the lower-VT group (12 ± 11 d vs 10 ± 11 d, P = .007). The mean Pplat was 25 ± 6 cm H2O in the lower-VT group and 33 ± 8 cm H2O in the higher-VT group (P < .001). The results of this study clearly demonstrate that, in patients with ALI/ARDS, mechanical ventilation with a lower VT and Pplat decreases mortality and ventilator days.
Volume or Pressure Limitation?
Whether the actual VT used should be based on the individual patient's lung mechanics, specifically Pplat, rather than a VT of 4–8 mL/kg has been debated.14 The argument in favor of Pplat rather than VT limitation questions the value of VT reduction in patients with ALI/ARDS whose Pplat is < 30 cm H2O. To address this question, Hager et al15 performed a secondary analysis of data from the ARDS Network. They found a beneficial effect of VT reduction from 12 mL/kg to 6 mL/kg, regardless of the Pplat before the VT reduction (Fig. 1).16 Patients enrolled in the ARDS Network study were divided into quartiles of Pplat. Using a logistic regression model, lower Pplat quartile, and lower Acute Physiology and Chronic Health Evaluation III score were significant predictors of lower mortality. However, the interaction between VT and Pplat quartile was not significant. Thus, patients in the 12 mL/kg PBW VT group would have benefited from VT reduction in each of the quartiles, even those in which Pplat was already < 31 cm H2O.
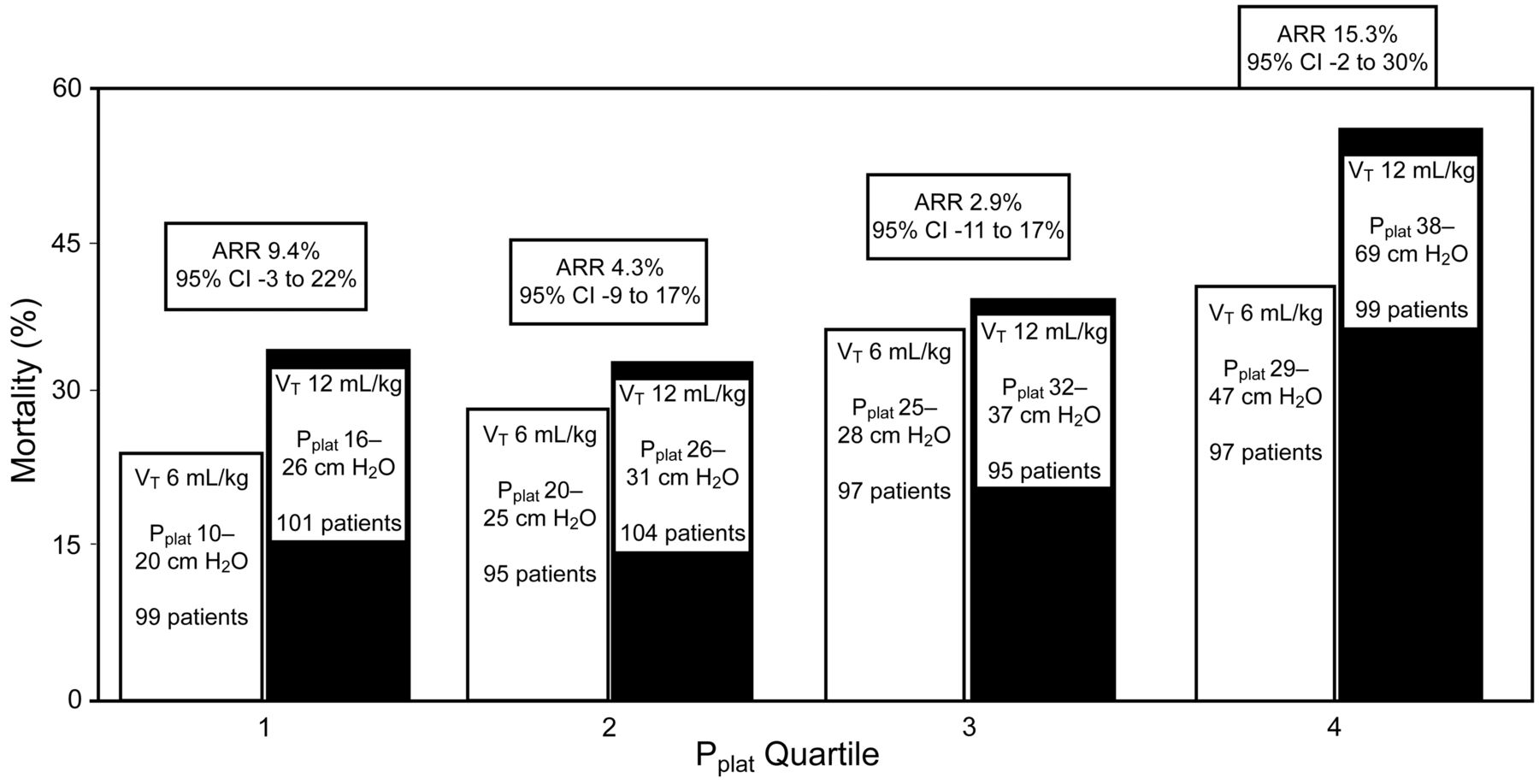
Mortality versus quartile of day-1 plateau pressure (Pplat) at tidal volume (VT) of 6 mL/kg ideal body weight (IBW) or 12 mL/kg IBW. The bars show the VT, the Pplat range, and the number of patients in each category. ARR = absolute risk reduction. (Data from Reference 76. Adapted from Reference 16, with permission.)
Terragni et al17 performed computed tomography (CT) at end-expiration and end-inspiration in 30 patients ventilated with a VT of 6 mL/kg IBW. They identified 20 of these patients in whom tidal inflation occurred largely in the normally aerated parts of the lungs, and 10 patients in whom tidal inflation occurred largely within the hyperinflated compartments. The non-aerated compartment was smaller and the normally aerated compartment was larger in the more protected patients than in the less protected patients. Pulmonary cytokines were lower in the more protected patients than in the less protected patients. Ventilator-free days were 7 ± 8 days and 1 ± 2 days in the more protected and less protected patients, respectively. Pplat was 25–26 cm H2O in the more protected patients and 28–30 cm H2O in the less protected patients. These results suggest that limiting VT to 6 mL/kg IBW and Pplat < 30 cm H2O may not be sufficient in patients characterized by a larger non-aerated compartment.
The findings of Hager et al15 and Terragni et al17 suggest that there might not be a safe Pplat in patients with ALI/ARDS. To achieve optimal lung protection, the lowest Pplat and VT possible should be selected. This is limited by the degree of permissive hypercapnia that the clinician is willing to accept. It has been suggested, primarily from experimental models, that permissive hypercapnia may be protective.18 Kregenow et al19 evaluated the effect of hypercapnic acidosis in a secondary analysis of the ARDS Network database. They found that hypercapnic acidosis was associated with reduced 28-day mortality in the 12 mL/kg IBW VT group, after controlling for comorbidities and severity of lung injury. However, this was not found when the further ongoing injury was reduced by 6 mL/kg predicted body weight VT.
Potential for Auto-PEEP
To prevent acidosis with low-VT ventilation, higher than normal respiratory rates are set—as high a 35 breaths/min in the ARDS Network study.13 This has raised concern about the development of auto-PEEP.20 However, when data from patients enrolled in the ARDS Network study were examined, the level of auto-PEEP was minimal.18 This, in fact, is predictable. Although a high respiratory rate is expected to shorten the expiratory time, the inspiratory time is shorter due to the smaller VT . In addition, the low compliance (high elastance) in ALI/ARDS results in a greater elastic recoil pressure pushing gas out of the lungs during exhalation.
Pressure Controlled Versus Volume Controlled Ventilation
One of the ongoing debates is whether pressure controlled ventilation (PCV) should be used a part of lung-protective ventilation strategy.21 There are advantages and disadvantages to either PCV or volume controlled ventilation (VCV) (Table 1). Purists will argue that the ARDS Network study was conducted with VCV; to achieve similar results, one should apply the evidence in the same way as was done in the predicate study. However, others will argue that some advantages might exist with PCV. With PCV, Pplat can never be greater than the peak inspiratory pressure. The square wave of inspiratory pressure with PCV will result in a higher mean airway pressure, which might improve ventilation/perfusion matching and PaO2. Moreover, the flow pattern is an exponential decay, which might improve distribution of ventilation, ventilation/perfusion matching, and PaO2. Finally, the variable inspiratory flow has the potential to improve patient-ventilator synchrony.
Volume Controlled Versus Pressure Controlled Ventilation
Despite many clinicians having a bias in favor of PCV in patients with ALI/ARDS, evidence supporting the superiority of PCV in this setting is weak. For the same VT, the same inspiratory time, and a descending ramp of flow with VCV, the differences in PaO2 between PCV and VCV are trivial.22 Experimental models of ALI/ARDS suggest that the high initial flow that occurs with PCV might be injurious rather than lung-protective.23–25
Whether synchrony is better with PCV than VCV is also debatable. Some have reported better synchrony with PCV,26,27 but this has not been confirmed by others.28 Adaptive pressure control modes might be particularly problematic, as they can take away support for the patient if respiratory drive is high and the resultant VT exceeds the target.29–33 Some clinicians are attracted to PCV because it allows the patient to increase VT if respiratory drive increases. However, this may make it difficult to avoid alveolar over-distention and maintain lung-protective ventilation.28,34 Indeed, Leray et al35 report a case in which a patient recovering from ARDS was switched from VCV (VT 6 mL/kg IBW) to pressure support ventilation. With pressure support ventilation the VT increased to 14 mL/kg and the patient developed air leaks. When VCV was restored, the air leaks resolved. This makes the point that VT can become excessive with pressure-targeted modes. Although PCV maintains a constant pressure applied to the airway, any additional effort from the patient will lower the pleural pressure, and the transpulmonary pressure will increase (Fig. 2).34

Estimation of transpulmonary pressure during spontaneous breathing on pressure-targeted ventilation. Note that the pressure across the alveolus is determined not only by the pressure applied to the airway, but also by the change in pleural pressure. Paw = proximal airway pressure. PS = pressure support. PR = pressure drop due to airways resistance. PA = alveolar pressure. ΔPA = transalveolar pressure. Patm = atmospheric pressure. Ppl = pleural pressure. (Adapted from Reference 34, with permission.)
In the hands of a skilled clinician, either VCV or PCV can probably be applied in a lung-protective manner. What is most important is limitation of VT and alveolar distending pressure, regardless of the mode set on the ventilator.
Synchrony
It is the perception of many clinicians that patient-ventilator asynchrony ensues when VT is reduced to 6 mL/kg. Why this should occur is unclear. A normal VT is 6–8 mL/kg, so it would seem that this VT should be comfortable during mechanical ventilation. There are several potential reasons why a VT of 6–8 mL/kg might not be comfortable with ALI/ARDS. First, dead space is increased with ALI/ARDS, and thus respiratory acidosis will occur unless minute ventilation is increased.36–40 In the ARDS Network study,13 respiratory rates up to 35 breaths/min were used in an attempt to avoid acidosis. Other potential reasons for asynchrony are pain and anxiety due to endotracheal intubation and the disease process. Thus, adequate attention should be given to address these discomforts.
With low-VT ventilation the inspiratory time may be very short. This can produce an inspiratory time set on the ventilator that is less than the neural inspiratory time of the patient. The result is that the patient will double-trigger the ventilator. During VCV, a double-trigger can result in breath stacking and double the desired VT. This effectively negates the intent of volume and pressure limitation. In one study it was reported that double-triggering is common during low-VT ventilation.41
A number of strategies can be used to improve patient-ventilator synchrony during lung-protective ventilation (Table 2).42,43 A recent study44 reported improved outcomes with paralysis for the first 48 hours following intubation in patients with ARDS. The mechanism to explain this benefit is unclear, but may be related to improved ability to apply lung-protective ventilation strategies in the early phase of the disease process. A common perception of clinicians is that there is a greater requirement for sedation with low-VT ventilation. That sedative doses were found to be similar for patients randomized to 6 mL/kg versus 12 mL/kg VT in 2 ARDS Network centers supports the conclusion that sedative needs may be largely determined by clinical factors other than ventilation strategy.45,46
Approaches to Patient-Ventilator Asynchrony
Tidal Volume Limitation in Patients Who Do Not Have ALI/ARDS
Although the evidence is clear and conclusive for volume and pressure limitation in patients with ALI/ARDS, should we limit the VT in all patients? There are currently no randomized controlled trials that address this question, but accumulating observational evidence suggests that VT should be limited in all mechanically ventilated patients.47–51
Yilmaz et al51 reported the results of a quality-assurance project in which an interdisciplinary team of intensivists and respiratory therapists designed a protocol to limit VT to a maximum of 10 mL/kg IBW in all patients receiving invasive ventilation, with a recommendation to use 6–8 mL/kg for patients at any risk of ALI/ARDS. A chart with calculated values of IBW was attached to each ventilator and it was also provided online. Comprehensive didactic and Web-based teaching was provided to physicians, nurses, and respiratory therapists involved in the care of mechanically ventilated patients. This protocol was implemented along with a protocol to limit transfusions. With implementation of this protocol the frequency of ALI decreased from 28% to 10%, the duration of mechanical ventilation decreased from a median of 5 days to 4 days, and, in a multivariate logistic regression analysis, the intervention was associated with a reduction in the frequency of new ALI (odds ratio 0.21, 95% CI 0.10–0.40). These results suggest that ALI may be, to a large extent, iatrogenic and might be preventable through relatively simple interventions such as limitation of VT. Recent studies have also reported benefit for VT limitation in patients with severe brain injury52,53 and in potential organ donors with brain death,54 where it increased the number of eligible and harvested lungs compared with a conventional strategy using higher VT.
Is Volume and Pressure Limited Ventilation Widely Applied?
Volume and pressure limitation, at least for ALI/ARDS, should be standard practice. Some reports published soon after publication of the ARDS Network study found only a modest change in the prescribed VT.55,56 However, more recent studies have not confirmed those findings. Esteban et al57 reported that in 2004, compared with 1998, VT decreased significantly in patients with ARDS (7.4 mL/kg vs 9.1 mL/kg, P < .001). Checkley et al58 reported a gradual and ultimately substantial effect on lowering of VT at ARDS Network hospitals after completion of the study. However, these findings may not be generalizable to non-enrolled patients or to patients from other hospitals.
Adoption of lower-VT ventilation may be improved with feedback and education on lung-protective mechanical ventilation. Even a costly intervention to improve adherence to low-VT ventilation in patients with ALI reduces death and is cost-effective by current societal standards.59 Recording VT in mL/kg IBW rather than the more traditional approach of absolute VT might draw clinician attention to excessive VT. Similarly, recording Pplat rather than peak inspiratory pressure alone may draw clinicians' attention to excessive distending pressure. A recent study described the use of a computer system to alert bedside providers (respiratory therapists and critical care fellows) by text paging notification about potentially injurious ventilator settings. This was associated with decreased patient exposure to potentially injurious settings.60
Prolonged Inspiratory Time and Inverse Inspiratory-Expiratory Ratio
In the mid-1980s there were reports of improved oxygenation with pressure controlled inverse-ratio ventilation (PCIRV),61–65 and for some time in the decade thereafter there was enthusiasm for this method. With PCIRV, an inspiratory time greater than the expiratory time is used to increase mean airway pressure and thus improve arterial oxygenation. Although inverse-ratio ventilation is most often used with PCV, VCV with inverse ratio has also been described.66 Following the initial enthusiasm for this approach, a number of subsequent controlled studies reported no benefit or marginal benefit of PCIRV over more conventional approaches to ventilator support in patients with ARDS.67–71 A disadvantage of this approach is that the auto-PEEP that occurs with PCIRV may adversely affect hemodynamics. Because this approach is uncomfortable for the patient, sedation and paralysis are often required. Based on the available evidence, there is no clear benefit for PCIRV in the management of patients with ARDS. The improvement in oxygenation PCIRV is small and the risk of auto-PEEP and hemodynamic compromise is great.72–74
Setting PEEP for ALI and ARDS
Most patients who require mechanical ventilation for ALI/ARDS receive PEEP of 5–12 cm H2O.57,75 PEEP < 5 cm H2O is probably harmful, at least in the early stages of the disease process.76 Higher PEEP may improve oxygenation and reduce VILI, due to better alveolar recruitment. But higher PEEP may also cause lung injury from over-distention. A matter of controversy is how to set PEEP for patients with ALI/ARDS.
The Randomized Controlled Trials
To date, 6 clinical trials have assessed the application of lower versus higher PEEP in patients with ALI/ARDS.11,77–81 Of these, only 2 reported a significant mortality reduction with higher PEEP.11,81 In both of the studies, however, 2 interventions were applied. That is, a higher PEEP was combined with a lower VT. Therefore, it is unknown whether the mortality benefit was related to the higher PEEP, lower VT, or a combined effect of the 2 interventions.
In an ARDS Network study, Brower et al77 randomly assigned 549 patients with ALI/ARDS to receive either lower or higher PEEP. All patients received volume and pressure limitation according to the original ARDS Network study.13 The PEEP was selected according to different tables of predetermined combinations of PEEP and FIO2, selected to maintain PaO2 in the range of 55–80 mm Hg or SpO2 in the range of 88–95% (Table 3). The mean ± SD PEEP on days 1 through 4 were 8.3 ± 3.2 cm H2O in the lower-PEEP group and 13.2 ± 3.5 cm H2O in the higher-PEEP group. Not surprising, the PaO2/FIO2 was significantly greater in the higher-PEEP group (P < .01). The rates of death before hospital discharge were 24.9% and 27.5%, respectively (P = .48). There were 14.5 ± 10.4 ventilator free days in the lower-PEEP group and 13.8 ± 10.6 ventilator free days in the higher-PEEP group (P = .50). The data and safety monitoring board stopped the study at the second interim analysis, after 549 patients had been enrolled, on the basis of futility. The authors concluded that, in patients with ALI/ARDS who receive mechanical ventilation with a VT goal of 6 mL/kg of IBW and a Pplat ≤ 30 cm H2O, clinical outcomes are similar whether lower or higher PEEP is used.
Tables Used to Set Combinations of FIO2 and PEEP in the ARDS Network Study
Meade et al78 reported a study to compare a low-VT ventilation strategy with an experimental strategy designed as an open-lung approach, which combines low VT, lung-recruitment maneuvers, and high PEEP. This was a randomized controlled trial with concealed allocation and blinded data analysis conducted in 30 intensive care units in Canada, Australia, and Saudi Arabia. The study enrolled 983 patients with ALI and PaO2/FIO2 ≤ 250 mm Hg; 85% of the subjects met the criteria for ARDS at enrollment. The control strategy included a target VT of 6 mL/kg IBW, Pplat ≤ 30 cm H2O, and a conventional PEEP level (n = 508). The open-lung strategy included target VT of 6 mL/kg IBW, Pplat ≤ 40 cm H2O, recruitment maneuvers, and higher PEEP (n = 475). The mean PEEP was 14.6 ± 3.4 cm H2O in the open-lung group and 9.8 ± 2.7 cm H2O in the control group during the first 72 hours (P < .001). All-cause hospital mortality rates were 36.4% and 40.4%, respectively (P = .19). Barotrauma rates were 11.2% and 9.1% (P = .33). The open-lung group had lower rates of refractory hypoxemia (4.6% vs 10.2%, P = .01), death with refractory hypoxemia (4.2% vs 8.9%, P = .03), and use of rescue therapies (5.1% vs 9.3%, P = .045). The authors concluded that, for patients with ALI/ARDS, a ventilation strategy designed to recruit and open the lungs resulted in no significant difference in hospital mortality, compared with an established low-VT ventilation strategy. This open-lung strategy did appear to improve secondary end points related to hypoxemia and use of rescue therapies.
Mercat et al79 designed a study to compare the effect on outcome of a strategy for setting PEEP aimed at increasing alveolar recruitment while limiting hyperinflation to one aimed at minimizing alveolar distention in patients with ALI. This was a multicenter randomized controlled trial of 767 adults conducted in 37 intensive care units in France. The VT was set at 6 mL/kg IBW in both strategies. Patients were randomly assigned to a moderate PEEP strategy of 5–9 cm H2O (n = 382) or to a PEEP set to reach a Pplat of 28–30 cm H2O (n = 385). The 28-day mortality rate in the minimal-distention group was 31.2% versus 27.8% in the increased-recruitment group (P = .31). The hospital mortality rate in the minimal-distention group was 39.0% versus 35.4% in the increased-recruitment group (P = .30). The increased-recruitment group, compared with the minimal-distention group, had a higher median number of ventilator-free days (7 d, interquartile range [IQR] 0–19 d vs 3 d, IQR 0–17, P = .04) and organ-failure-free days (6 d, IQR 0–18 vs 2 d, IQR 0–16, P = .04). This strategy also was associated with higher compliance values, better oxygenation, less use of adjunctive therapies, and larger fluid requirements. The authors concluded that a strategy for setting PEEP aimed at increasing alveolar recruitment while limiting hyperinflation did not significantly reduce mortality. However, it did improve lung function and reduced the duration of mechanical ventilation and the duration of organ failure.
The reason why these 3 trials were negative with respect to a survival benefit has been the source of much speculation and debate. Perhaps a higher level of PEEP in patients with ALI/ARDS is not effective. Perhaps the methods used to set PEEP were not the correct approaches. Perhaps higher PEEP is not effective in unselected patients with ALI/ARDS, but might be effective in patients with ARDS but not ALI, or in patients with a higher potential for recruitment. Or perhaps these studies, although relatively large, were underpowered to show a difference in outcome.82
PEEP and Potential for Recruitment
An important issue with the use of higher PEEP is the associated increase in Pplat.43 This is more likely to occur when higher PEEP is added to patients who have nonrecruitable lung regions. Patients who have recruitable lungs have proportionally less increase in Pplat when PEEP is raised, and such patients may benefit from PEEP with less risk of over-distention. It is likely that the trials of higher versus lower PEEP77–79 enrolled patients who had both a lower and a greater potential for alveolar recruitment.
In 68 patients with ALI/ARDS, Gattinoni et al83 evaluated the relationship between the percentage of potentially recruitable lung and the clinical and physiologic effects of PEEP. Patients underwent whole-lung CT at airway pressures of 5, 15, and 45 cm H2O. The potential for recruitment was defined as the proportion of lung tissue in which aeration was restored at airway pressures between 5 and 45 cm H2O. They found that the percentage of potentially recruitable lung ranged widely in these patients, with a mean of 13 ± 11% of the lung weight. An average of 24% of the lung could not be recruited. Patients with a higher percentage of potentially recruitable lung, greater than the median value of 9%, had greater total lung weights, lower PaO2/FIO2 and respiratory-system compliance, higher dead space, and higher mortality. CT was better than physiologic variables for predicting the amount of recruitable lung, Clinically relevant changes in physiologic markers with higher PEEP, such as reduced physiologic dead space (or a decrease in PaCO2 at a fixed minute ventilation) or an increase in respiratory-system compliance, may be helpful indicators of lung recruitability.
To investigate how lung recruitability influences alveolar strain and cyclical opening and closing after the application of high PEEP, Caironi et al84 analyzed data from the 68 patients with ALI/ARDS in the previously described paper by Gattinoni.83 Alveolar strain and opening and closing lung tissue were computed at 5 and 15 cm H2O PEEP. In patients with a higher percentage of potentially recruitable alveoli, the increase in PEEP reduced the amount of opening and closing lung tissue (P < .001). However, no differences were observed in patients with a lower percentage of potentially recruitable alveoli. Alveolar strain similarly increased in the 2 groups. Opening and closing lung tissue was distributed mainly in the dependent and hilar lung regions, and it was an independent risk factor for death. The authors concluded that, in patients with higher alveolar recruitability, the beneficial impact of reducing cyclical alveolar opening and closing by increasing PEEP prevails over the effects of increasing alveolar strain.
Because the effects of high PEEP depend on lung recruitability, which varies widely among patients with ARDS, increasing PEEP may lead to alveolar over-distention (harm), or to less cyclical alveolar opening and closing (benefit). This is illustrated in Figure 3. If the increase in PEEP is greater than the increase in Pplat, presumably alveolar recruitment has occurred, the respiratory system is improved, and the benefit of higher PEEP may be greater than the potential harm of the small increase in Pplat. On the other hand, if the increase in Pplat is greater than the increase in PEEP, particularly if the resulting Pplat is > 30 cm H2O, then it can be argued that the harm of over-distention is greater than the benefit of alveolar recruitment with PEEP. Because the 3 PEEP studies probably enrolled some patients with higher potential for recruitment and other patients with a lower potential for recruitment, this may explain the negative results.

Potential effects of an increase in PEEP. If the potential for recruitment is low, an increase in PEEP results in a large increase in plateau pressure (Pplat) (increased driving pressure), to an unsafe level. In this case, the potential harm from over-distention probably outweighs any benefit resulting from increased alveolar recruitment. If the potential for recruitment is high, an increase in PEEP results in little increase in Pplat. In this case, the potential benefit of increased PEEP probably outweighs the harm due to the small increase in Pplat.
A higher PEEP potentially increases the risks of hemodynamic compromise and barotrauma. Pneumothorax rate does not appear to be greater in patients receiving higher PEEP.85 The risk of complications is probably related to over-distention rather than PEEP per se.
The Meta-Analyses
The value of a meta-analysis is that, by pooling data from several studies, statistical power is improved. Thus, results from smaller negative studies might prove positive when combined in a meta-analysis. There are 5 meta-analyses published on the topic of higher versus lower PEEP in patients with ALI/ARDS (Table 4).85–89 Of these, 4 found no effect on mortality from higher PEEP, compared with moderate PEEP, in unselected patients with ALI/ARDS.85,87–89
Meta-analyses of Studies That Compared Higher Versus Lower PEEP
The meta-analysis by Briel et al86 is of particular interest. Data from 2,299 individual patients in 3 trials were analyzed, using uniform outcome definitions. The mortality rate was 32.9% for patients assigned to treatment with higher PEEP, and 35.2% for patients assigned to lower PEEP (adjusted relative risk 0.94, 95% CI 0.86–1.04, P = .25). However, treatment effects varied with the presence or absence of ARDS (PaO2/FIO2 ≤ 200 mm Hg). In patients with ARDS the mortality was 34.1% in the higher-PEEP group and 39.1% in the lower-PEEP group (adjusted relative risk 0.90, 95% CI 0.81–1.00, P = .049). In patients without ARDS the mortality was 27.2% in the higher-PEEP group and 19.4% in the lower-PEEP group (adjusted relative risk 1.37, 95% CI 0.98–1.92, P = .07). The results of this meta-analysis suggest that treatment with higher versus lower PEEP was associated with improved survival among the subgroup of patients with ARDS (PaO2/FIO2 ≤ 200 mm Hg). Interestingly, there was a trend toward worse outcomes with higher PEEP in the subgroup with ALI (PaO2/FIO2 > 200 mm Hg).
Approaches to Setting PEEP
Zero PEEP is probably harmful during mechanical ventilation of patients with ALI/ARDS.76 Higher PEEP is probably better in patients with ARDS, and moderate PEEP may be better for patients with ALI. The challenge at the bedside is to select the PEEP that is appropriate for the individual patient, and a number of approaches have been described in the literature (Table 5).
Methods for Selecting PEEP
In the ARDS Network studies13,77 and the study by Meade et al,78 PEEP was individually titrated according to a table, with combinations of PEEP and FIO2 selected for a target arterial oxygenation (see Table 3). These tables have been widely criticized as arbitrary and not fitted to the lung mechanics of an individual patient. Despite the criticism of these tables, they have been used successfully in all of the trials conducted by the ARDS Network and thus have high face validity.16 But because these tables do not select PEEP based on potential for alveolar recruitment, their use might lead to over-distention in patients who have less potential for recruitment.90–92
The method used by Mercat et al79 is simple and attractive. They adjusted PEEP based on airway pressure, and PEEP was set as high as possible without increasing the Pplat above 28–30 cm H2O. PEEP was individually titrated based on Pplat, regardless of its effect on oxygenation. Using this approach, higher PEEP will probably be set when there is much potential for recruitment, because there will be less increase in Pplat when the application of PEEP increases alveolar recruitment. On the other hand, if there is less potential for recruitment, the Pplat limit will be reached quickly when the PEEP is increased.79
In a classic paper published in 1975, Suter et al93 studied 15 normovolemic patients who required mechanical ventilation for acute pulmonary failure. The PEEP that resulted in the maximum oxygen delivery and the lowest dead-space fraction also resulted in the greatest respiratory-system compliance. The optimal PEEP ranged between 0 and 15 cm H2O. Mixed venous PO2 increased between 0 PEEP and the PEEP that resulted in maximum oxygen delivery, but then decreased at higher PEEP. The authors concluded that respiratory-system compliance can be used to determine the optimal PEEP. Because compliance = VT /(Pplat – PEEP), the optimal PEEP is that which results in the lowest driving pressure (Pplat –PEEP) if VT is kept constant. What is most attractive about this approach is that it is easy to evaluate at the bedside.
The pressure-volume (PV) curve has been used to select optimal PEEP (Fig. 4).94 With this approach, the relationship between volume and pressure as the lungs are inflated or deflated is evaluated. By assessing the shape of this relationship, the pressure at which alveoli are recruited or derecruited is identified. This approach has been used in several randomized controlled trials of lung-protective ventilation.11,81 Measurement of the PV curve, however, requires sedation and often paralysis, because even minimal patient effort may confound measurements of inflection points. There can be considerable inter-observer variability in interpreting PV curves.95 Separation of the effect of the chest wall from the effect of the lungs on the PV curve is not possible without measuring esophageal pressure.96–98 The shape of the PV curve may be affected by the starting pressure (ie, PEEP).99,100 Finally, it is now accepted that recruitment may occur throughout the entire inflation PV curve. As such, attention has focused more recently on the deflation limb of the PV curve, where the upper inflection point may represent the beginning of derecruitment.101 The traditional method for determining the PV curve is to use a calibrated syringe, with measures of pressure for each step change in volume. Dynamic PV curves plotted on the ventilator screen are potentially useful only if the lungs are inflated with a constant slow flow.94 Dynamic PV curves measured during PCV or descending-ramp VCV are not useful. Although automated procedures integral to the ventilator system have made it easier to construct a PV curve,102 more evidence is needed before the PV curve can be recommended for routine use to determine optimal PEEP.

The pressure-volume curve of a normal subject (dashed curve) and a patient with acute respiratory distress syndrome (ARDS) (solid curve). The pressure-volume curve is shifted downwards on the volume axis and has a reduced total lung capacity (TLC). The sigmoid shape of the curve is much more evident in ARDS. Note the small amount of pressure at the start of the ARDS pressure-volume curve, indicating a small amount of intrinsic PEEP (PEEPI) at end-expiratory lung volume (EELV). Some investigators divide the curve into linear segments: Cstart, Cinf or Clin, and Cend (thin lines, explained below). Using these segments, the upper and lower Pflex (the pressure at the intersection of 2 lines: a low-compliance region at low lung volumes [Cstart] and a higher-compliance region at higher lung volumes [Cinf]) were defined by the intersection of these lines. The lower inflection point (LIP) and upper inflection point (UIP) are defined by where the curve first begins to deviate from the line Clin. Mathematically these are not inflection points; the true inflection point (where concavity changes direction) is marked by the solid dot. (Adapted from Reference 94.)
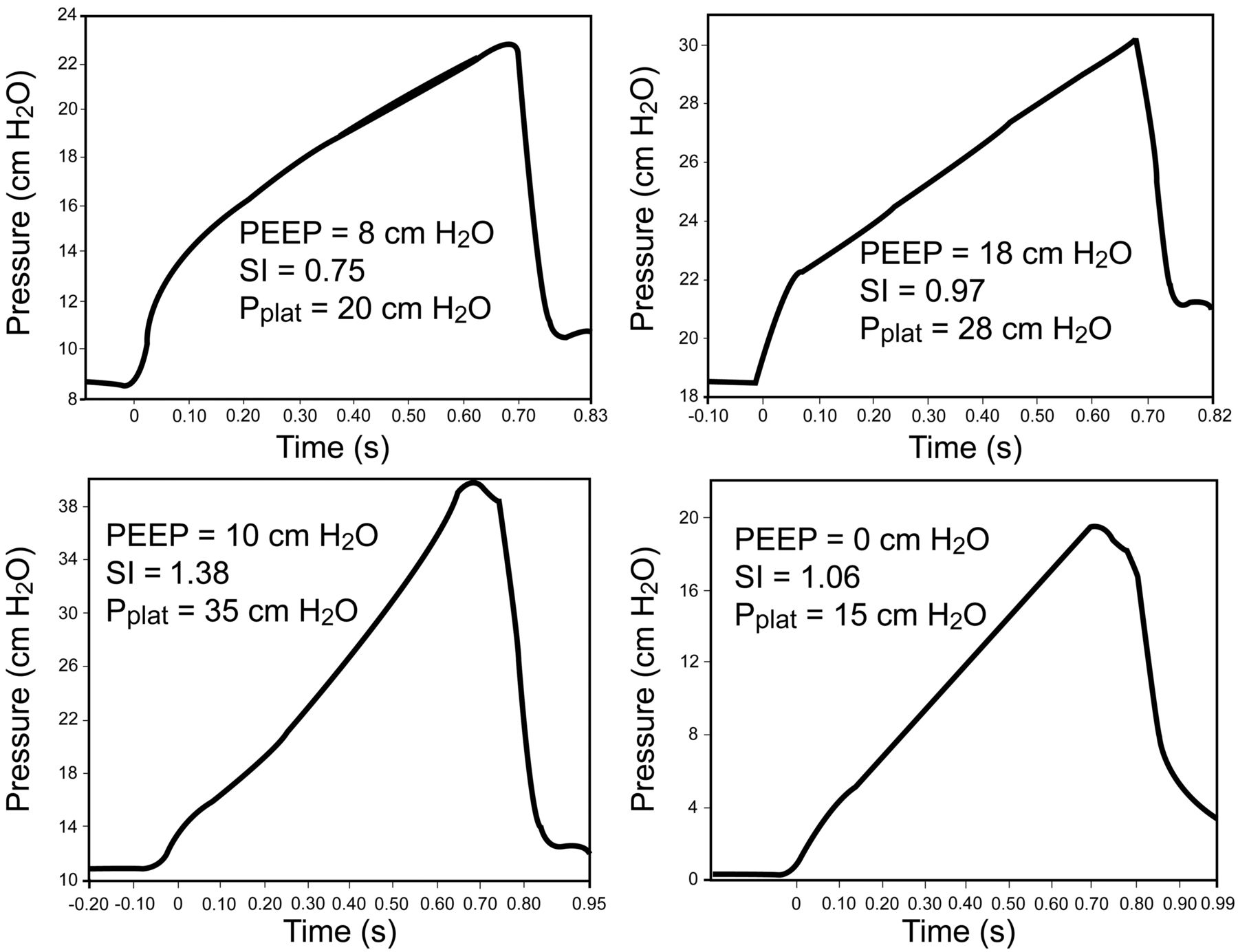
The stress index has been proposed to assess the level of PEEP to maximize recruitment yet avoid over-distention.91,103 This approach uses the shape of the pressure-time curve during constant-flow VCV. A linear increase in pressure suggests adequate recruitment without over-distention. If compliance is worsening as the lungs are inflated (upward concavity, stress index > 1), this suggests over-distention and the recommendation is to decrease PEEP. If the compliance is improving as the lungs are inflated (downward concavity, stress index < 1), this suggests tidal recruitment and potential for additional recruitment, and thus a recommendation to increase PEEP. Examples of changes in stress index in patients with ARDS are shown in Figure 5.

Top: Stress index in a patient early in the course of acute respiratory distress syndrome (ARDS) secondary to H1N1 infection. In this case the stress index improved as PEEP was increased. Bottom: Stress index (SI) in a patient late in the course of ARDS. In this case the stress index improved as PEEP was decreased.
Particularly in patients with extrapulmonary ARDS, the chest-wall compliance may be reduced.104 Chest-wall compliance is reduced with abdominal-compartment syndrome, chest-wall edema, pleural effusion, or obesity.105,106 This can result in an increase in pleural pressure and, if pleural pressure is high relative to alveolar pressure, there may be potential for alveolar collapse (Fig. 6). In that case it is desirable to keep PEEP greater than pleural pressure. The use of an esophageal balloon to assess intra-pleural pressure has been advocated to allow more precise setting of PEEP (Fig. 7).80,106–108 Unfortunately, artifacts in esophageal pressure, especially in supine critically ill patients, make it difficult to measure absolute pleural pressure accurately.109 In patients with abdominal-compartment syndrome, bladder pressure may be useful to assess intra-abdominal pressure, the potential collapsing effect on the lungs, and the amount of PEEP necessary to counterbalance this effect.105,107
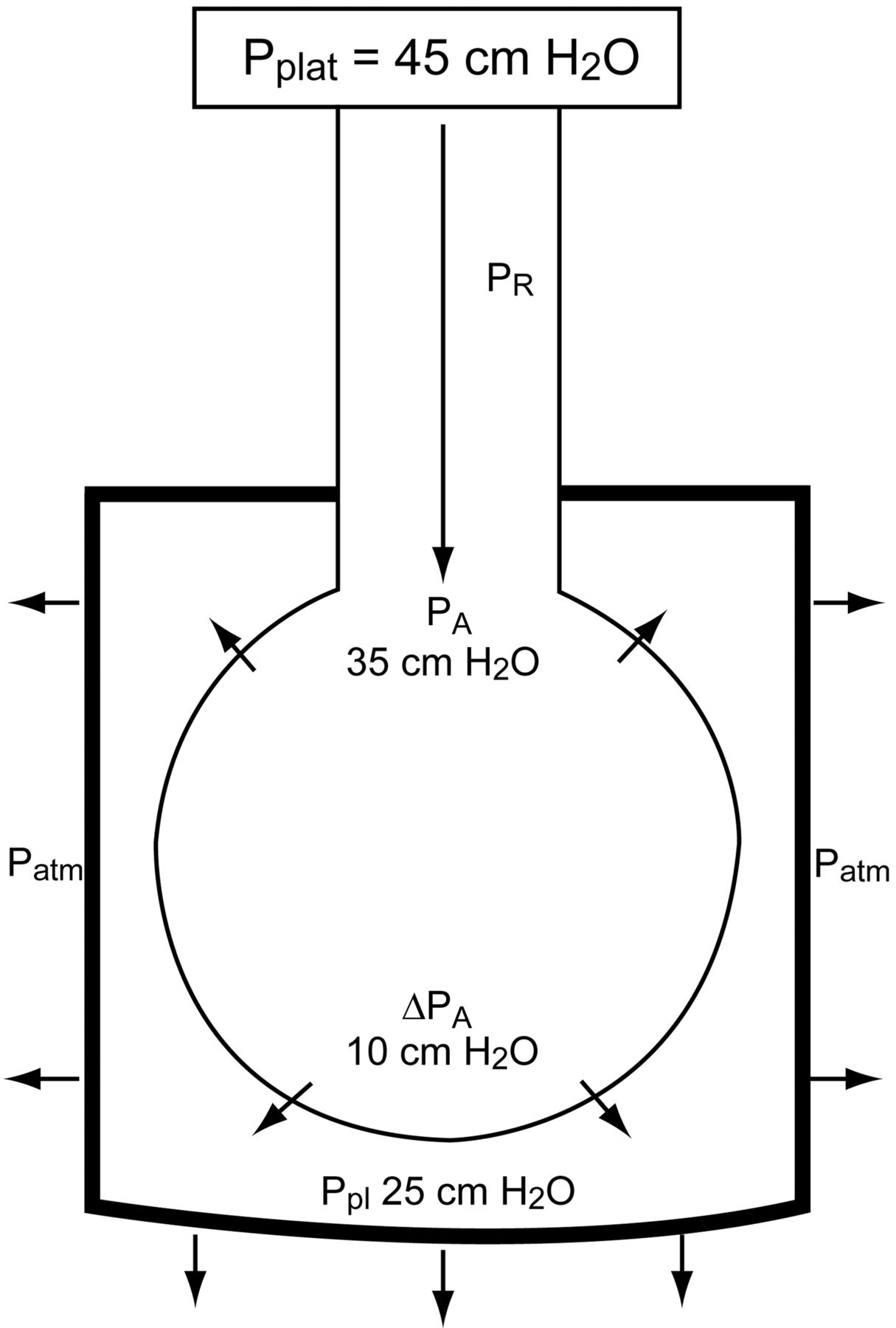
Effect of a stiff chest wall on transpulmonary pressure. In this example, although the plateau pressure (Pplat) is 35 cm H2O, the distending pressure across the alveolus is only 10 cm H2O because the pleural pressure is 25 cm H2O. PR = pressure drop due to airways resistance. PA = alveolar pressure. ΔPA = transalveolar pressure. Patm = atmospheric pressure. Ppl = pleural pressure.
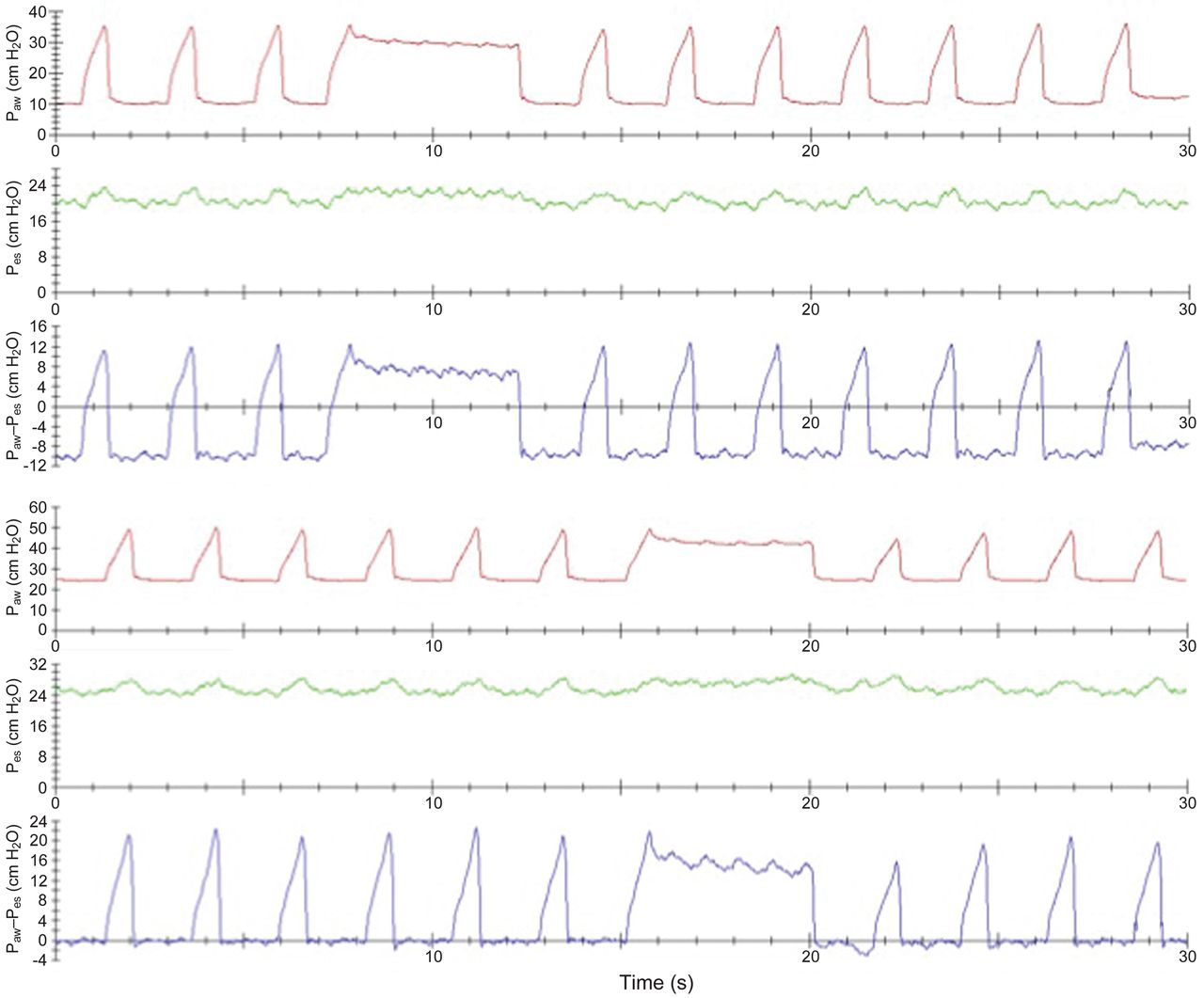
Example of PEEP titration in a patient with morbid obesity. Top: Esophageal pressure (Pes), as a surrogate for pleural pressure, is greater than the setting on PEEP. Bottom: PEEP setting is increased so that the collapsing effect of the intrapleural pressure is counterbalanced. Note that, despite the plateau pressure of 40 cm H2O, the alveolar distending pressure is only 14 cm H2O.
Some advocate opening the lung with recruitment maneuvers, with subsequent stepwise reduction of PEEP until evidence of derecruitment (eg, respiratory-system compliance change) is identified on the deflation limb of the PV curve, with a decremental, rather than an incremental, PEEP trial.110,111 Using this approach, PEEP is set ≥ 20 cm H2O and then decreased to identify the level that produces the best PaO2 and compliance. However, a recent study was unable to show differences in patient outcomes when setting PEEP with a table was compared to a method that used recruitment maneuvers and decremental PEEP.112
Dead-space measurements may be helpful to determine the optimal PEEP.93 As PEEP is increased, the ratio of dead space to VT (VD/VT) should decrease as alveoli are recruited. If PEEP results in alveolar over-distention, however, VD/VT should increase. It should be possible, however, to assess these effects by evaluating PaCO2 with fixed minute ventilation; a decrease in PaCO2 is consistent with a lower VD/VT, and vice versa. Methods are now available to measure functional residual capacity at the bedside in patients with ARDS.113,114 However, it is difficult to know whether an increase in lung volume with an increase in PEEP is due to alveolar recruitment or over-distention.
Imaging techniques have been used to evaluate PEEP settings. But CT is not practical. Ultrasound115 and electrical impedance tomography116,117 need additional validation. One issue with these imaging techniques is that it can be difficult to differentiate recruitment from over-distention.
It is unclear whether any one of the methods to set PEEP is superior to the others. Use of higher PEEP, when compared to use of moderate PEEP, does not lead to lower mortality in groups of unselected patients with ALI/ARDS. It is becoming increasingly recognized that different PEEP strategies may be needed for different types of ARDS; for example, when the lungs are highly recruitable versus poorly recruitable. Unfortunately, given the complexity of conducting clinical trials in patients with ALI/ARDS, it is unlikely that high-level studies of higher versus moderate PEEP will be conducted in patients selected on the basis of alveolar recruitment potential.
PEEP is good for patients with ALI/ARDS. The debate is not whether PEEP should be used, but rather how much PEEP should be used. Second, the available evidence suggests that a modest PEEP may be more appropriate for ALI (PaO2/FIO2 > 200 mm Hg), whereas higher PEEP should be used for ARDS (PaO2/FIO2 ≤ 200 mm Hg). Higher PEEP should be reserved for patients in whom alveolar recruitment can be demonstrated. Increasing PEEP while driving up the Pplat to a harmful level makes no sense.
Stress and Strain
The primary determinants of VILI are stress and strain.118 Stress is the internal distribution of the counterforce per unit of area that balances and reacts to an external load. The associated deformation of the structure is strain, defined as the change in size or shape in reference to the initial status. The clinical equivalent of stress is transpulmonary pressure (ΔPL), and the clinical equivalent of strain is the ratio of volume change (ΔV) to the functional residual capacity (FRC):
ΔV is the change in lung volume above resting FRC with the addition of PEEP and VT. Specific lung elastance is relatively constant at about 13.5 cm H2O. A harmful threshold of strain is about 2. Thus, the harmful threshold of stress (transpulmonary pressure) is approximately 27 cm H2O. The recommended Pplat below 30 cm H2O is thus reasonable for most patients with ALI/ARDS. However, a higher Pplat may be safe when transpulmonary pressure is reduced due to an increase in pleural pressure. This makes a case for measurement of esophageal pressure (as a surrogate for pleural pressure) in a patient with a stiff chest wall.
This concept can be illustrated from Figure 7. When the PEEP is set at 24 cm H2O, the end-inspiratory transpulmonary pressure (stress) is 14 cm H2O. From the equation above, strain is about 1. In this case, stress at 14 cm H2O and strain at 1 are both in the safe range (< 27 cm H2O and < 2, respectively), despite the Pplat of 40 cm H2O.
Summary
Lung-protective ventilation strategies are now widely accepted in the management of patients with ALI/ARDS. In most, if not all, cases of ALI/ARDS, conventional ventilation strategies can be used effectively, as described in this paper. A suggested approach is given in Table 6.
Ventilator Settings for ALI/ARDS
Footnotes
- Correspondence: Dean R Hess PhD RRT FAARC, Respiratory Care, Ellison 401, Massachusetts General Hospital, 55 Fruit Street, Boston MA 02114. E-mail: dhess{at}partners.org.
Dr Hess presented a version of this paper at the 26th New Horizons Symposium, “ARDS Update,” at the 56th International Respiratory Congress of the American Association for Respiratory Care, held December 6–9, 2010, in Las Vegas, Nevada.
Dr Hess has disclosed relationships with Philips Respironics, Covidien, ResMed, Pari, and Breathe Technologies.
- Copyright © 2011 by Daedalus Enterprises Inc.
References
- 1.↵
- 2.
- 3.
- 4.
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.
- 38.
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.
- 49.
- 50.
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.
- 63.
- 64.
- 65.↵
- 66.↵
- 67.↵
- 68.
- 69.
- 70.
- 71.↵
- 72.↵
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}