

Abstract
An increasing number of patients, mainly COPD and overlap-syndrome patients, simultaneously use home oxygen therapy and noninvasive ventilation (NIV) at night. Usually the oxygen source is a stationary concentrator. We report a patient who, without a medical recommendation, was using a portable oxygen concentrator during nocturnal NIV. In the laboratory, with the patient, we tested the portable oxygen concentrator's triggering and oxygen delivery, with the supplemental oxygen connected at 3 different positions: near the ventilator, near the exhalation valve, and on the nasal mask port. We also tested the concentrator's triggering capacity by placing the nasal prongs and the nasal mask independently. We tested ventilator inspiratory pressures of 10, 14, and 18 cm H2O, and expiratory pressures of 4 and 6 cm H2O. The portable oxygen concentrator did not detect the patient's inspiratory effort or deliver the required oxygen flow at any of the tested settings. We recommended that the patient not use the portable oxygen concentrator during nocturnal NIV.
Introduction
Long-term oxygen therapy can be administrated from gaseous oxygen, portable liquid oxygen systems, and stationary oxygen concentrators. A recent addition to the market was the portable oxygen concentrator, which allows much greater freedom of movement to chronic respiratory insufficiency patients, and is now considered a standard practice in stable home-oxygen patients. High-quality concentrators have been designed to be used 24 hours a day, 7 days a week,1,2 and have been clinically proven to provide the necessary oxygen for most ambulatory patients during all phases of daily activity and sleep. Most portable concentrators incorporate pulse-dose technology.3
In our experience, an increasing number of patients, mainly COPD and overlap-syndrome patients, are simultaneously using home oxygen therapy and noninvasive ventilation (NIV) at night. The patient must connect the ventilator to the oxygen source before going to bed. Although we found no evidence in the literature about the prevalence of this practice, in our experience 30% of patients add oxygen to nocturnal NIV. Usually the oxygen source is a stationary concentrator. The efficacy of portable pulse-dose oxygen concentrator during nocturnal NIV has not been studied. We studied a patient who, without a medical recommendation, was using a portable oxygen concentrator during nocturnal NIV.
Case Summary
The patient was a 69-year-old male with obesity hypoventilation syndrome and severe COPD (Global Initiative for Chronic Obstructive Lung Disease stage IV). He was using nocturnal NIV (Trilogy100, Philips Respironics, Murrysville, Pennsylvania) and home oxygen from a stationary concentrator, for more than 20 hours a day. Every night before going to bed, he connected the oxygen tube to the ventilator circuit and so was receiving NIV and oxygen simultaneously. He had an active life, including traveling from Madrid to Geneva by plane once a month, for 3–4 days. He traveled without oxygen, due to bureaucratic and logistical difficulties, and slept with only nocturnal NIV during his stays in Geneva. Recently, the stationary concentrator was changed to a portable pulse-dose concentrator (Inogen One, Inogen, Goleta, California) by the patient's home respiratory therapy supplier (Fig. 1). He supposed he could use the portable concentrator inside the plane and attach it to the ventilator, day and night. He used the portable concentrator during the day without any problems, but he complained about the absence of the pulse-dose noise from the concentrator when the oxygen tube was connected to the NIV circuit at night and the continuous presence of the “no oxygen delivery” alarm on the concentrator.

Trilogy100 noninvasive ventilator (left) and Inogen One pulse-dose oxygen concentrator (right).
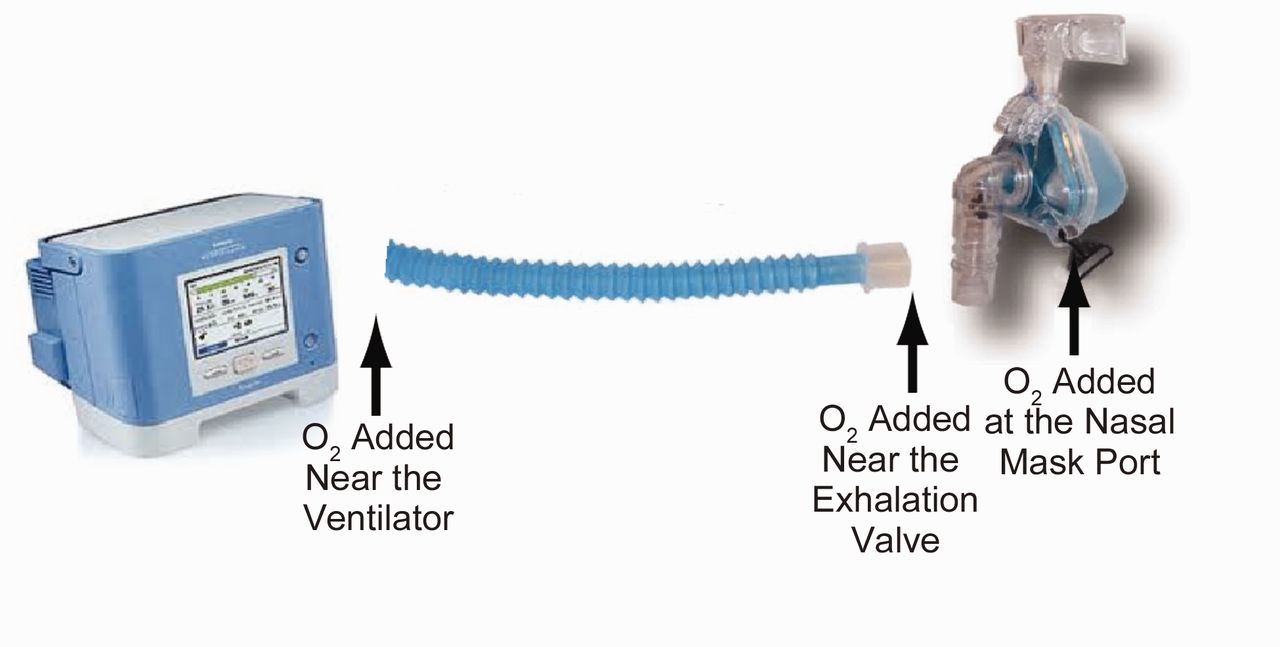
He informed us about this problem. We suspected that NIV could hinder the concentrator's triggering, so we tested the concentrator and oxygen flow while he simultaneously used the concentrator and ventilator. We tested adding oxygen at 3 places in the ventilator circuit: near the ventilator, near the exhalation valve, and at the nasal mask port (Fig. 2). The concentrator did not detect the patient's inspiratory effort or deliver the preset oxygen flow at any of the tested settings.

We connected the supplemental oxygen supply at 3 places: near the ventilator, near the exhalation valve, and on the nasal mask port. The patient was unable to trigger the oxygen concentrator at any of the tested inspiratory or expiratory pressures or oxygen connection points.
We also tested the concentrator's triggering with the patient simultaneously using his usual nasal cannula and the NIV nasal mask (Fig. 3), and we obtained the same results: the concentrator did not detect the patient's inspiratory efforts. We tested ventilator inspiratory pressures of 10, 14, and 18 cm H2O, and expiratory pressures of 4 and 6 cm H2O, and obtained the same results. Therefore we recommended that he not use the portable oxygen concentrator during NIV.

Patient receiving oxygen via nasal prongs and noninvasive ventilation via nasal mask.
Discussion
Pulse-dose technology, also referred to as demand oxygen delivery,4 is an important development in portable oxygen systems. Portable oxygen concentrators are designed to be small enough to be carried by the patient, and can be powered by standard household alternating current, direct current (available in most motor vehicles), or rechargeable battery. A portable concentrator can also use pulse-dose technology and produce a variable oxygen percentage.5 Some, including the Inogen One, offer only a pulse-dose mode. The available portable concentrators have markedly different performance, so it is necessary to adjust the concentrator to meet the specific patient's needs, at rest and during activity.6 There are concerns regarding these concentrator's triggering sensitivity and response to varying nocturnal breathing patterns,5,7 and NIV can hinder the concentrator's triggering.
An increasing number of patients, especially COPD patients, use home oxygen during nocturnal NIV. The Eurovent study8 found that 34% of home mechanical ventilator users had lung diseases. Despite conflicting evidence about a long-term benefit from ventilation in COPD patients, the study showed that it is widely used, so oxygen plus NIV will be used by a growing number of patients. This is an important fact in the context of “non-delivery” or “deliveryless” technology.9,10
The Inogen One did not detect our patient's inspiratory efforts because of “pressure contamination” in the circuit from the ventilator. Pulse-dose oxygen technology generally works by detecting the patient's inspiratory effort and triggering the delivery of a bolus of oxygen in the first 100 ms of the inspiration. The oxygen flow then turns off until the next inspiration is detected. Like other portable oxygen concentrators, the Inogen One uses pressure sensing to identify the onset of inspiration. The Inogen One also monitors the respiratory rate and adjusts the bolus volume to maintain a consistent minute volume of oxygen. The NIV inspiratory and expiratory pressures in the ventilator circuit prevented the Inogen One from identifying the onset of inspiration, so the concentrator simply did not work as it is supposed to. We think these results can be extrapolated to other portable concentrators, which we are now testing.
Portable oxygen concentrators are considered as deliveryless technology, but our results show a clear limitation of portable oxygen concentrators in clinical practice. If patients and doctors do not know that a portable concentrator might not work during NIV, the patient can be undertreated at night, receiving no supplemental oxygen during sleep, which is an important problem that can lead to clinical deterioration.
We speculate that NIV may hinder triggering of portable oxygen concentrators. We need to study these devices from a clinical point of view to determine their efficacy in various settings. Further research is needed to determine the general performance of portable oxygen concentrators in patients who use nocturnal NIV and oxygen therapy. Deliveryless technology is a challenge in patients receiving NIV.
Footnotes
- Correspondence: Salvador Díaz Lobato PhD, Pneumological Department, Hospital Ramón y Cajal de Madrid, Carretera de Colmenar Viejo, KM 9,100, Madrid 28034 Spain. E-mail: sdiazlobato{at}gmail.com.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1975
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}