

Abstract
BACKGROUND: Elevated dead space fraction (the ratio of dead space to tidal volume [VD/VT]) is a feature of ARDS. PEEP can partially reverse atelectasis, prevent alveoli recollapse, and improve lung compliance and gas exchange in patients with ARDS. However, whether VD/VT variables have a close relationship with PEEP and collapse alveolar recruitment remains under recognized. Meanwhile, few clinicians titrate PEEP in consideration of changes in VD/VT. Therefore, we performed the study to evaluate VD/VT, arterial oxygenation, and compliance changes during PEEP titration following lung recruitment in ARDS patients.
METHODS: Twenty-three ARDS patients ventilated in volume-controlled mode were enrolled in the study. Sustained inflation (40 cm H2O, 30 s) was used as a recruitment maneuver, followed by decremental PEEP changes from 20 to 6 cm H2O, in steps of 2 cm H2O, and then to 0 cm H2O. VD/VT, pulmonary mechanics parameters, gas exchange parameters, and hemodynamic parameters were recorded after 20 min at each PEEP step.
RESULTS: Compared with VD/VT at the PEEP levels of 20 cm H2O and 0 cm H2O, VD/VT was significantly lower at 12 cm H2O (P = .02), and compliance of the static respiratory system (CRS) was significantly higher at pressure step 12/10 cm H2O (P < .001). Compared with PaCO2 at the PEEP level of 20 cm H2O, PaCO2 was significantly lower at 12 cm H2O (P < .001). Arterial oxygenation values and functional residual capacity were reduced gradually during PEEP, decreasing from 20 cm H2O to 0 cm H2O.
CONCLUSIONS: A significant change of VD/VT, compliance and arterial oxygenation could be induced by PEEP titration in subjects with ARDS. Optimal PEEP in these subjects was 12 cm H2O, because at this pressure level the highest compliance in conjunction with the lowest VD/VT indicated a maximum amount of effectively expanded alveoli. Monitoring of VD/VT was useful for detecting lung collapse and for establishing open-lung PEEP after a recruitment maneuver.
Introduction
ARDS is a major cause of acute respiratory failure, with high morbidity and mortality.1,2 There is convincing evidence from radiologic and pathologic studies showing that alveolar collapse and diffuse endothelial and epithelial injury are prominent features of ARDS.3,4 Alveolar collapse leads to an elevated pulmonary shunt and intractable hypoxemia, and, as a consequence, mechanical ventilation is often implemented to restore adequate oxygenation.5,6
It has been evident over the past 2 decades that recruitment maneuvers (RM) and an adequate PEEP could reverse atelectasis, prevent alveoli recollapse, and improve lung mechanics and gas exchange.7 However, the adequate level of PEEP that avoids alveoli recollapse and at the same time does not overdistend the lung is difficult to determine at bedside.
Dead space fraction (the ratio of dead space volume to tidal volume [VD/VT]) is useful to research the efficiency of ventilation; its variables can reflect alveolar collapse and recruitment. Elevated VD/VT may be explained by lung vascular injury and obstruction, as well as by an increase in ventilation of poorly perfused alveoli secondary to ventilation-perfusion mismatch or overinflation of normal compliant lung units. Studies in patients with ARDS revealed that elevated VD/VT was a feature of ARDS,8–11 and is independently associated with an increased risk of death. Some publications supported the value of monitoring the relationship between PEEP and VD/VT during positive-pressure ventilation. Early in 1975,12 Suter et al showed that the “best” PEEP closely correlated with the lowest VD/VT as well as with the highest compliance and oxygen transport in patients with acute lung injury. Tusman et al showed that in an experimental model of patients with respiratory failure who responded to PEEP with an increase in oxygenation also showed a decrease in VD/VT.13,14 However, some studies15,16 failed to find similar effect on VD/VT during PEEP titration in this kind of patient. Whether VD/VT variables have a close relationship with PEEP and collapse or alveolar recruitment remains controversial.
The approach to PEEP titration and the variables that reliably determine an adequate level of PEEP remain unanswered.17 We consider that downward titration of PEEP following an RM could recruit alveoli, but that higher PEEP levels may increase VD/VT by regional overdistention of well ventilated alveoli. Therefore, the aim of this study was to evaluate the effects of PEEP on VD/VT, compliance, functional residual capacity (FRC), and arterial oxygenation before and after an RM in patients with ARDS.
QUICK LOOK
Current knowledge
Elevated ratio of dead space to tidal volume (VD/VT) is common in ARDS and is associated with greater mortality. PEEP and/or lung-recruitment maneuvers can improve VD/VT. It is unknown whether VD/VT can help guide the setting of PEEP and the use of recruitment maneuvers.
What this paper contributes to our knowledge
In the context of recruitment and PEEP titration, lowered VD/VT was associated with increased functional residual capacity, compliance, and PaO2/FIO2. Measurement of VD/VT might help to assess alveolar recruitment and implement a lung-protective ventilation strategy.
Methods
Patient Selection
Patients with ARDS admitted to the Department of Critical Care Medicine, Zhong-Da Hospital, Southeast University, Nanjing, Jiangsu, China, from June 2009 to January 2010 were enrolled in the study. The study protocol was approved by the local ethics committee, and informed consent was obtained from each subject or surrogate. The inclusion criteria were: ≥ 18 years old, mechanical ventilation via an orotracheal tube or tracheostomy, and meeting the American-European Consensus Conference criteria for ARDS18 (PaO2/FIO2 ≤ 200 mm Hg, bilateral opacities on chest radiograph, and either a pulmonary-artery wedge pressure of ≤ 18 mm Hg or absence of clinical evidence of left atrial hypertension). Patients were excluded if they met diagnostic criteria for ARDS for ≥ 72 hours, had obstructive or interstitial lung disease, had a history of congestive heart failure with left ventricular ejection fraction ≤ 40%, had pneumothorax, or were pregnant.
Anesthesia, Ventilation, and Monitoring
All subjects were supine and ventilated (Engström Carestation, GE Healthcare, Madison, Wisconsin) in a volume-controlled ventilation mode. There was no method of humidification during the study. Ventilation started with VT of 6 mL/kg predicted body weight and PEEP of 6 cm H2O. The respiratory rate was regulated according to PaCO2, which was kept between 36 and 42 mm Hg. The ratio of inspiratory time and expiratory time was 1:2. The FIO2 was regulated according to peripheral oxygen saturation (SpO2), which was kept above 90%.
Heart rate, invasive systolic, diastolic, and mean arterial blood pressure, central venous pressure, and SpO2 were measured by a monitor (S5, Datex Ohmeda, Madison, Wisconsin) during the entire study period. From the readings of the ventilator, the variables of PEEP, inspiratory pressure, VT, and minute ventilation were recorded.
Study Design
For an initial period of 30 min, lungs were ventilated in a volume-controlled ventilation mode, with VT of 6 mL/kg predicted body weight, respiratory rate of 24 breaths/min, and PEEP of 0 cm H2O. Before starting an RM, arterial blood gases, pulmonary mechanics, FRC and hemodynamics were measured. Collapsed alveolar recruitment was applied by RM, performed in sustained inflation (40 cm H2O, 30 s). Conditions for appropriate alveolar recruitment were considered as follows: PaO2/FIO2 ≥ 400 mm Hg; otherwise, we performed sustained inflation again until change in PaO2/FIO2 was < 10% between 2 sustained inflations.19 After RM, PEEP titration was applied as follows: PEEP was decreased from 20 to 6 cm H2O in steps of 2 cm H2O and then to 0 cm H2O. The ventilation mode was volume-controlled, and other settings were the same as above. Each pressure level was maintained for approximately 20 min, except if any of the hemodynamic variables deviated from baseline by > 15% or new arrhythmia emerged. Hemodynamics, pulmonary mechanics, arterial blood gases, and VD/VT were observed at the end of 20 min. During the study, anesthesia was maintained with fentanyl 50 μg/h and midazolam 2–4 mg/h. Vecuronium bromide induced relaxation by neuromuscular block. The monitoring of neuromuscular block was done with nerve stimulator (train-of-4 monitoring).
Measurements
FRC was calculated by an automated procedure available in the ventilator, based on the nitrogen washout method, with an FIO2 step change of 0.1, as previously described by Olegård et al.20 Using sidestream gas analyzing technology, calculation of FRC values was obtained by applying the following equations.
The fractions of inspired and end-tidal nitrogen were calculated from:
where FIN2 is the fraction of inspired nitrogen, PETO2 is the partial pressure of end-tidal oxygen, and PETN2 is the partial pressure end-tidal nitrogen.
Expired and inspired alveolar VT were calculated by energy expenditure measurements for V̇O2 and V̇CO2, where
where RQ is respiratory quotient.
Nitrogen volumes associated with expiration and inspiration for a single breath were:
The changes during one breath equaled:
Before making the step change in FIO2, we measured V̇O2, V̇CO2, and PETN2. Oxygen uptake (V̇O2) and carbon dioxide production (V̇CO2) were assumed to be constant throughout the measurement. After a step response the FRC was calculated as:
where the PETN2 was the last recorded value after the step change:
Airway pressure values were measured by the ventilator at the level of the Y piece. At each PEEP level, end-inspiratory holds (inspiration holds) and end-expiratory holds (expiration holds) were performed (each lasting for at least 5 s). Intrinsic PEEP was determined automatically by the ventilator. Static compliance of the respiratory system (CRS) was calculated by dividing the expiratory VT by the pressure difference between end-inspiratory plateau pressure (Pinsp) and total end-expiratory pressure (Pexp):
Arterial blood samples were drawn at the end of each protocol step and analyzed for PaO2, PaCO2, SaO2, and pH. These values were measured by the blood-gas analyzer (ABL 700, Radiometer, Copenhagen, Denmark). Samples were processed within 5 min.
VD/VT was measured by volumetric capnography (NICO Cardiopulmonary Management System, Novametrix, Wallingford, Connecticut), which calculated the partial pressure of mixed-expired CO2, then acquired by the Enghoff modification of the Bohr equation as follows:
where PeCO2 is mean expired CO2.21 An arterial blood gas sample was obtained when the PeCO2 variability on the NICO monitor was ≤ 1 mm Hg within 5 min; these values were then used to calculate VD/VT. The NICO monitor had been validated as an accurate measurement of VD/VT in patients with ARDS. The NICO sensor fits between the Y-piece and the endotracheal tube, and VD/VT measurement is not affected by circuit compression.
Clinical Data Collection
The following data were recorded: age, sex, weight, height, and severity of illness, evaluated with the Acute Physiology and Chronic Health Evaluation II (APACHE II) during admission to the ICU, and lung injury score on the day of VD/VT measurement. We also recorded the etiology of the ARDS and respiratory parameters, including CRS, plateau pressure, FRC, and VD/VT.
Statistical Analysis
All data were analyzed using statistics software (SPSS 16.0, SPSS, Chicago, Illinois). Measurements and other recorded values were expressed as mean ± standard deviation. Variables were analyzed by one-way analysis of variance. Baseline (0 cm H2O of PEEP prior to RM) or 20 cm H2O of PEEP after RM were taken as reference values. Receiver operating characteristic (ROC) curves were generated for VD/VT, FRC, lung injury score, and APACHE II with prognosis. The areas under the ROC curves were calculated for each parameter. P value of < .05 was considered statistically significant.
Results
Baseline Characteristics
A total of 23 subjects with ARDS were enrolled in the study (7 women and 16 men; mean age 57 ± 16 y). The demographics, etiology of ARDS, and baseline physiologic variables are summarized in Table 1. The mortality at 28 days was 52.2%. The mean VD/VT was higher among subjects who died than among those who survived (0.64 ± 0.08 versus 0.53 ± 0.04). The area under the ROC curve for VD/VT was 0.867 (see Table 1).
Baseline Demographics, Clinical Characteristics, and Physiologic Variables of the 23 Study Subjects
VD/VT Change Induced by Different PEEP Levels
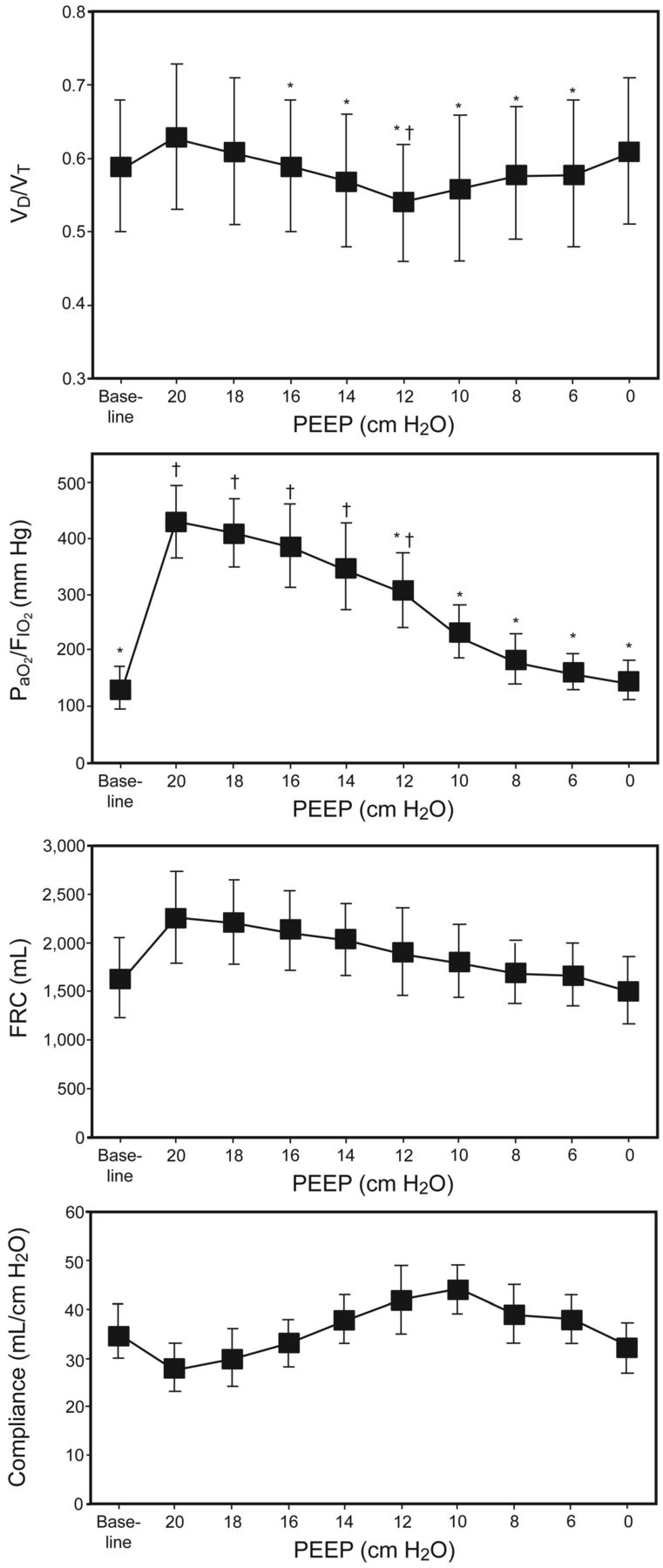
At the pressure level of PEEP 20 cm H2O after recruitment, VD/VT increased from 0.59 ± 0.09 to 0.63 ± 0.11. However, when PEEP decreased from 20 cm H2O to 12 cm H2O, VD/VT decreased gradually to 0.54 ± 0.08. While from 12 cm H2O to 0 cm H2O, VD/VT increased to 0.61 ± 0.10. Comparing the pressure level of baseline and PEEP 20 cm H2O, VD/VT value was significantly lower at the pressure level of PEEP 12 cm H2O (P = .02) (Fig. 1 and Table 2).

Changes of dead space fraction (the ratio of dead space to tidal volume [VD/VT]), PaO2/FIO2, functional residual capacity (FRC), and static respiratory system compliance (mean ± SD) during decremental PEEP after recruitment maneuver (n = 23). * P < .05 was considered significant, comparing the PEEP level of 20 cm H2O, † P < .05 was considered significant, comparing the baseline.
Dead Space Fraction, PaCO2, PaO2/FIO2, Functional Residual Capacity, Respiratory System Compliance, and Airway Resistance Change During Decremental PEEP After Recruitment Maneuver
Change of PaO2/FIO2 and FRC During PEEP Decrement
After RM, PaO2/FIO2 and FRC values significantly increased, then decreased gradually while PEEP reduced from 20 cm H2O to 0 cm H2O. Compared to the baseline, PaO2/FIO2 and FRC values were notably higher on all pressure steps, except for the pressure levels of PEEP 8/6/0 cm H2O (see Fig. 1 and Table 2).
CRS Change During PEEP Decrement
Compared to the baseline and PEEP 20 cm H2O after RM, CRS values were significantly higher on the pressure levels of PEEP 12/10 cm H2O. Intrinsic PEEP remained below 2 cm H2O in all subjects (see Fig. 1 and Table 2).
Hemodynamic Change Induced by Different PEEP Levels
Arterial blood pressure, heart rate, and central venous pressure did not change significantly during the test periods (Table 3).
Hemodynamic Change During Decremental PEEP After Recruitment Maneuver
Relationship Between VD/VT and Prognosis
The areas under the ROC curves were as follows: 0.87 ± 0.05 for VD/VT, 0.83 ± 0.03 for FRC, 0.75 ± 0.06 for lung injury score, and 0.78 ± 0.05 for APACHE II. The area for VD/VT was significantly greater than the area for lung injury score (P = .005) and APACHE II (P = .006). The threshold VD/VT value of 0.57 allowed discrimination between deceased and surviving subjects with a sensitivity of 83% and a specificity of 82%. The threshold FRC value of 1,605 mL allowed discrimination between deceased and surviving subjects with a sensitivity of 91% and a specificity of 75%. The threshold APACHE II value of 17.5 allowed discrimination between deceased and surviving subjects with a sensitivity of 83% and a specificity of 73% (Fig. 2).

The area under the receiver operating characteristic curve for dead space fraction, functional residual capacity (FRC), lung injury score, and Acute Physiology and Chronic Health Evaluation (APACHE II) score.
Discussion
In this clinical study, a decremental PEEP procedure was performed after an RM. We observed that PEEP caused a significant change of VD/VT as well as FRC, CRS, and PaO2/FIO2. VD/VT also showed a high sensitivity and specificity for predicting prognosis. Our results suggest that VD/VT, in the context of recruitment and a PEEP titration procedure, might become a clinically useful bedside tool for assessing collapsed alveolar opening and implementing an open-lung protective ventilation strategy in patients with ARDS.
Various studies in patients with ARDS reported that increased VD/VT is one of the hallmarks of early ARDS, and an elevated VD/VT is independently associated with an increased risk of death. Our study showed an increased physiologic VD/VT in the early phases of ARDS, which is consistent with results from previous studies.7–9 Elevated VD/VT in the early phase of ARDS probably reflects alterations in the distribution of pulmonary blood flow and may be explained by several mechanisms. Pulmonary vascular injury leads to vasoconstriction and vascular obstruction. Intrapulmonary shunt perturbs carbon dioxide exchange by increasing alveolar dead space,22–24 particularly in the presence of low cardiac output, reduced hemoglobin levels and metabolic acidosis. An increase in ventilation of poorly perfused alveoli secondary to ventilation-perfusion mismatch or overinflation of normal compliant lung units, resulting in maldistribution of pulmonary blood flow, are plausible explanations for an elevated VD/VT.
RM combines with PEEP and low VT to recruit collapsed alveoli, prevent recollapse of alveoli, and avoid regional and global stress and strain on the lung parenchyma. A study by Maisch et al25 analyzed the effects of PEEP and recruitment on VD/VT, FRC, CRS, and PaO2 in anesthetized patients with healthy lungs. The effects of PEEP in conjunction with RM were evaluated in ARDS patients. The results showed that different PEEP levels after RM caused significant changes in VD/VT as well as in PaO2/FIO2, FRC, and CRS in ARDS patients. Our data are in agreement with those of Gattinoni et al,26 which indicated the same recruitment effect: after the recruitment, the lung's capacity for CO2 elimination is increased. This, in turn, corresponds with a decrement in PaCO2. However, higher PEEP could increase VD/VT by regional overdistention of well ventilated alveoli (and therefore increase in zone I conditions in the lung)27 or by reduction in cardiac output.28,29
As a result of lung collapse, refractory hypoxemia is a predominant clinical feature, caused mainly by the intrapulmonary shunt and a reduced lung volume. Accordingly, determination of the alveolar recruitment is performed by analyzing PaO2/FIO2. However, arterial oxygenation depends on the hemodynamic and metabolic state, which is nonspecific for judging recruitment effect, and insensitive to the overdistention of alveoli. This fact was confirmed in our study. As shown in Figure 1, the highest PaO2/FIO2 was reached at PEEP 20 cm H2O after recruitment; however, CRS reduced and VD/VT increased, which indicated overdistended lungs. Another disadvantage of using PaO2/FIO2 to determine the recruitment effects is the trouble and expense of drawing and analyzing a series of arterial blood samples in a timely manner.
FRC results revealed a similar effect to PaO2/FIO2. FRC was higher after the recruitment. However, FRC seems to be insensitive for detecting lung overdistention. A gain in absolute lung volume after the recruitment could not result from a pure distention of aerated alveoli or airways, but should be the result of an increase in functional alveolar units. Thus, this is proof for the intended “opening effect” of an alveolar recruitment.
As a result of alveolar collapse, decreased CRS is one of the physiopathological hallmarks of ARDS. Data from various studies supported CRS as a marker of alveolar recruitment. However, as an easier measurement, CRS has some limitations. Rothen et al showed that the changes over time of static CRS and the amount of atelectasis estimated by computed tomography were not in parallel.30 On the other hand, the point of maximum CRS indicated the PEEP level at which lung collapse started to occur, as confirmed by the appearance of atelectasis on computed tomography scan.31 In our study, PEEP corresponding to the maximum after RM was found to be 10 cm H2O, which was lower than the PEEP corresponding to the minimal VD/VT.
In our study, the alveolar recruitment strategy was performed by a sustained inflation, in order to minimize the side effects of RM and shorten the study period in the clinical setting. Blood gas values were determined at the end of sustained inflation, in order to reach a complete recruitment in all subjects. Conditions for complete recruitment were as follows: PaO2/FIO2 ≥ 400 mm Hg or change in PaO2/FIO2 < 10% after sustained inflation.
There are limitations to our study. In the context of recruitment and PEEP, collapsed alveolar opening could be assessed only by indirect computed tomography methods, not direct measurements.32 Study periods were long because both FRC and blood gas values were determined at the end of each protocol step. Further limitations of this study were lack of data of oxygen transport, and a small number of subjects.
Conclusions
In conclusion, in the context of recruitment and a PEEP titration procedure, a reduction of the VD/VT and increase in FRC, CRS, and PaO2/FIO2 could be induced in patients with ARDS; optimal PEEP in these subjects was 12 cm H2O, because at this pressure level the highest CRS in conjunction with the lowest VD/VT indicated a maximum amount of effectively expanded alveoli. The measurement of VD/VT might become a clinically useful bedside tool for assessing alveolar recruitment and implementing an open-lung protective ventilation strategy.
Footnotes
- Correspondence: YANG Yi MD, Department of Critical Care Medicine, Zhong-Da Hospital, Southeast University, 210009 Nanjing, Jiangsu, China. E-mail: yiyiyang2004{at}yahoo.com.cn.
This work was supported by grant BK2008298 from the Nature Science Foundation of Jiangsu Province.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}