

Abstract
Weaning comprises 40 percent of the duration of mechanical ventilation. Protocols to reduce weaning time and to identify candidates at the earliest possible moment have been introduced to reduce complications and costs. Increased demand for mechanical ventilation, an increase in the number of patients requiring prolonged ventilation, and resource/staffing issues have created an environment where automated weaning may play a role. A number of closed loop techniques have been introduced since the early 1990s, with increasing sophistication. Preliminary research has demonstrated mixed results. Current systems continue to be evaluated in different patient populations and environments. Automated weaning is part of the ICU armamentarium, and identification of the patient populations most likely to benefit needs to be further defined.
Introduction
Weaning from mechanical ventilation has undergone whole scale renovation over the last decade. While perhaps appropriately dubbed “weaning” during the early years of positive-pressure ventilation, the gradual withdrawal of mechanical ventilation was in fact necessitated by early clinical practice and technology. Patients were frequently ventilated by overriding the respiratory drive and abolishing patient efforts. Heavy sedation and or paralysis were used, and patients were awakened after 10–14 days, in hopes of initiating weaning. Respiratory muscle atrophy and asynchrony were unrecognized or perhaps considered the cost of life-saving mechanical ventilation. After days of respiratory muscle inactivity, the slow resumption of spontaneous breathing and weaning ventilatory support must have appeared a necessity.1,2
In recent years, the term “weaning” has been replaced by “liberation” from or “discontinuation” of ventilatory support to reflect the fact that a gradual withdrawal was not only unnecessary but potentially harmful.3–6 Daily spontaneous breathing trials (SBTs) have been identified as the most expeditious way to determine safe discontinuation of ventilatory support, and bedside protocols facilitate this practice.7–18
The success of protocols cannot be overemphasized and is one of the potential advantages that lend support to the implementation of closed loop weaning. Protocols can be operationalized as both decision support systems or closed loop control of ventilator variables. This paper will describe the argument for expanded use of closed loop ventilation and describe the evidence using current closed loop techniques for weaning.
State of the Art Ventilator Discontinuation
While weaning remains the most common term for describing the process of gradual withdrawal of ventilatory support, it may also include an abrupt withdrawal without traditional weaning. In either case, weaning involves the transition of the work of breathing and control of ventilation from the ventilator to the patient, a little at a time or all at once. Of note is that the weaning process accounts for nearly 40% of the duration of invasive ventilation.8 Since costs and complications of invasive mechanical ventilation are substantial, discontinuation at the earliest possible moment is imperative.9,10
Liberating the patient from mechanical ventilation emphasizes early identification of patients for ventilator discontinuation using screening assessments.10–13 Patients who successfully pass screening assessments undergo SBTs, typically lasting 30–120 min, during which time specific physiologic measures determine success or failure.16–18 The literature supports the use of protocols conducted by the bedside caregivers (respiratory therapists and nurses in the United States) to reduce practice variability and to avoid delays created by physician availability.10–18 However, there remain difficulties in implementing protocols in a multidisciplinary ICU, and at least one group has demonstrated that protocols operated by respiratory therapists were not superior to physician directed weaning.19 The physician staffing and expertise in this study, however, may not be available in all ICUs. It is also of note that, while there were no differences in the patient outcomes, common sense suggests that physician directed weaning was more costly.
While there have been descriptions of modes of ventilation for weaning, including intermittent mandatory ventilation (IMV) and pressure support ventilation (PSV), to date no one method has been shown to have a clear advantage.17,18,20–22
The Argument for Automated Weaning Modes
While the earliest report of a method for automated weaning most likely lies in the initial description of mandatory minute volume (MMV) by Hewlett et al in 1977, there appears to have been little enthusiasm for this technology.23 More recently, a host of factors have transpired that appear not only to support the development of automated weaning but to mandate these techniques to standardize care and prevent errors. Clearly, technological advances in the sophistication of mechanical ventilators have been critical in allowing closed loop control. Similarly, advances in artificial intelligence and micro computing make closed loop control a bedside reality. But advances in technology alone do not justify closed loop control: technology simply makes automation possible. This creates the classic conundrum in medicine, just because we can do it, should we?
Table 1 lists the current limitations in ICU care and mechanical ventilation related to current healthcare realities in staffing, resources, and demand. Staffing shortages, increased demand for care, and failure to use evidenced-based practices translate into increased morbidity, mortality, and costs.24–42 Closed loop control of the weaning process and identification of patients for ventilator liberation have the possibility of serving as solutions to a number of these problems.
The Argument for Closed Loop Control and Automating the Weaning Process
Current State of the Art Closed Loop Systems
Closed loop control of mechanical ventilation has been covered in detail in a number of previous publications.43–46 This paper will strictly review closed loop control of the weaning process.
Mandatory Minute Volume
MMV, also called mandatory minute ventilation, was introduced by Hewlett et al in 1977.23 The original device was completely mechanical, using a metered flow of fresh gas (equal to desired minute volume [V̇E]) delivered to a reservoir bag for spontaneous breathing. The patient could breathe at any combination of spontaneous rate and tidal volume (VT) that satisfied the V̇E setting. If the patient did not meet the V̇E set value, the reservoir bag would begin to fill. If the bag became full, a mechanism would trigger mandatory breaths at a set VT. The mandatory breath rate would continue until the patient breathed enough volume from the bag to release the trigger mechanism.
Conceptually, MMV has been touted as a weaning mode. MMV has also been considered a safety net during weaning, in case of patient fatigue. Early in the history of MMV, shortcomings were identified and solutions were proposed.47 A major issue was the inability of the device to recognize hypoventilation (low VT and rapid respiratory rate—the hallmark of weaning failure) if the target V̇E was met.
With the introduction of microprocessor technology, MMV became easier to implement with additional monitoring and alarms. The most common approach was to follow the predicted V̇E, based on an average of a series of breaths over a designated time period.48–49 Some manufacturers achieved the V̇E goal through the addition of mandatory breaths at the set VT. This results in a variation of IMV with a variable mandatory breath rate based on the patient's spontaneous V̇E. Other ventilators use an adaptive pressure control strategy, increasing or decreasing pressure during spontaneous breathing to meet the V̇E target. These systems typically compare a rolling average of V̇E calculated over 8–10 breaths or over a predefined time frame and predict the V̇E based on this period of observation. When patient V̇E meets the set V̇E, there are no mandatory breaths.
Mandatory Minute Volume for Automated Weaning.
In 1989, Davis et al compared MMV to IMV in a group of 22 subjects with respiratory failure due to “pulmonary parenchymal and airway pathology.” They found that weaning with MMV was “rapid and less demanding on the ICU staff,” compared to IMV.50 IMV was weaned by 2 breaths every 3–4 hours during waking hours (06:00–18:00) and MMV was set at 75% of the patient's current V̇E. MMV patients weaned in a mean time of 4.75 hours, while IMV weaning required a mean time of 33 hours. Much of this difference could be attributed to the IMV protocol requiring the gradual withdrawal of mandatory breaths.
More recently, 2 trials of MMV have been accomplished in neonates.51,52 Claure et al compared IMV to computer controlled minute ventilation. The study used a modified Sechrist infant ventilator. The description of this mode implies MMV with adjustments in mandatory rate to maintain a desired V̇E. Interestingly, the Sechrist IV-100B did not have a commercially available version of MMV. Claure et al studied 15 infants with a mean gestational age of 26 weeks. They demonstrated that computer controlled minute ventilation resulted in fewer mandatory breaths (15 vs 9 breaths/min), lower peak mean airway pressures, and a reduced mandatory V̇E (116 vs 65 mL/min/kg). There were no differences in oxygen saturation or transcutaneous carbon dioxide. The authors concluded that computer controlled minute ventilation could provide similar gas exchange at lower levels of mechanical support, perhaps reducing the incidence of chronic lung disease and barotrauma. No weaning advantage was inferred.
Guthrie et al performed a short, crossover trial comparing MMV to SIMV in 20 infants > 33 weeks of gestational age.52 Confirming the work by Claure and colleagues, this study demonstrated a significant decrease in the number of mandatory breaths during MMV (4 vs 24 breaths/min), while gas exchange remained the same. Of note is that the spontaneous rate was significantly greater with MMV (42 vs 25 breaths/min), and there was concern that this change in breath type might lead to reductions in mean airway pressure leading to hypoxemia. The authors increased PEEP in the MMV subjects to prevent this mean airway pressure loss. In agreement with the other study in neonates, the authors speculated that reducing mandatory breaths might reduce barotrauma, but no reduction in weaning time was appreciated. Despite being developed solely as a process to facilitate or speed weaning, there is no evidence in the literature documenting any advantage of MMV.
Adaptive Pressure Ventilation
Adaptive pressure ventilation, or dual control, includes a number of breath delivery techniques, including volume support ventilation (VSV), pressure regulated volume control (PRVC), AutoFlow, Volume Control+, and others.53–55 Each technique is closed loop control of either pressure support or pressure control breaths, targeting a desired delivered VT. Adaptive pressure ventilation uses a negative feedback control mechanism, adjusting the pressure of a breath based on the difference in desired and actual VT from the previous breath.
Decreases in pulmonary compliance, increases in resistance, or reduced patient effort result in an increase in peak airway pressure. Increases in compliance, decreases in resistance, or an increased patient effort result in a decrease in peak pressure. Conceptually, as the patients' respiratory mechanics improve, the ventilator pressure is reduced until the patient is receiving a peak pressure of PEEP + 5 cm H2O, signaling time for ventilator discontinuation.
Adaptive Pressure Ventilation for Weaning.
Guldager et al compared PRVC to volume control ventilation in 44 adult patients with acute respiratory failure.56 In a crossover trial they demonstrated that PRVC provided ventilation with a lower peak inspiratory pressure, which was not much of a surprise, as the flow pattern in volume control was constant. Piotrowski et al,57 Kocis et al,58 and D'Angio et al59 all evaluated PRVC compared to SIMV in a neonatal population.57–59 Only D'Angio and colleagues evaluated the impact on time to ventilator discontinuation.59 They randomized 212 neonates with respiratory distress to either pressure targeted SIMV or PRVC in the assist control mode. This may confound the study, as one technique provides support to every triggered breath, while the other allows spontaneous breathing. In this carefully controlled trial there was no difference in the number of infants alive and extubated or those alive without bronchopulmonary dysplasia. More infants reached final extubation at 14 days of age in the pressure targeted SIMV group (44 of 108 vs 38 of 104), but there was no difference in the median time to final extubation. The authors concluded that in this group of neonates, who had received surfactant therapy, PRVC offered no advantage over SIMV.
In a recent study of 36 patients following cardiac surgery, Samantaray and Hemanth found that PRVC was associated with an improved oxygenation index compared to pressure control ventilation.60 No assessments of duration of mechanical ventilation were attempted.
Both PRVC and VSV were introduced without any clinical research to support the indication of reduced weaning time. Given our current knowledge regarding daily SBTs, it seems unlikely that breath to breath alterations in peak airway pressure will facilitate weaning. No literature supports the contention that adaptive pressure ventilation speeds discontinuation of mechanical ventilation.
AutoMode
AutoMode switches between pressure control and pressure support, based on the presence or absence of patient effort. AutoMode combines VSV and PRVC into a single mode. The mode provides PRVC if the patient is paralyzed. All breaths are mandatory breaths that are time triggered, pressure limited, and time cycled. The pressure limit increases or decreases to maintain the desired VT set by the clinician. If the patient triggers 2 consecutive breaths, the ventilator switches to VSV. If the patient becomes apneic for 12 seconds (8 s in the pediatric setting, or 5 s in the neonatal setting), the ventilator switches to PRVC. The change from PRVC to VSV is accomplished at equivalent peak pressures. AutoMode also switches from pressure control to pressure support, or from volume control to VSV. In the volume control to VSV switch, the VSV pressure limit will be equivalent to the pause pressure during volume control. If an inspiratory plateau is not available, the initial pressure level is calculated as:
AutoMode for Weaning.
A single clinical study of AutoMode, in patients with normal lungs and neurologic injury, demonstrated that during AutoMode fewer caregiver adjustments were necessary, compared to SIMV.61 This study also showed tighter control of PaCO2, but these differences were very small (39.5 ± 3.1 mm Hg vs 38.3 ± 7.3 mm Hg). No evidence supports the use of Automode to speed ventilator discontinuation.
Adaptive Support Ventilation
Adaptive Support Ventilation (ASV) was first described in the literature in 1994 and is perhaps the most studied of the closed loop techniques.62–64 ASV uses adaptive pressure ventilation in the delivery of both mandatory and spontaneous breaths to target a V̇E, VT, and respiratory rate based on the patient's ideal body weight and a percentage V̇E setting. The VT and respiratory frequency combination are selected based on the ideal body weight and the equation of Otis et al, which predicts that for a given V̇E there is an “optimal” breathing pattern associated with a minimum work of breathing.65 The clinician is responsible for setting PEEP, FIO2, body weight, and the percentage V̇E.
Under adult conditions, a setting of 100% V̇E results in a V̇E of 0.1 mL/kg/min (eg, a 60 kg patient would receive a V̇E of 6.0 L). As an example for this 6.0 L V̇E, the respiratory rate and VT combinations would range from 260 mL × 23 breaths/min to 600 mL × 10 breaths/min. The low-VT limit is governed by knowledge of the normal dead space (2.2 mL/kg) and the upper limit is constrained by setting the maximum pressure. Other combinations are possible, but this is the relevant clinical range. Otis's formula and predicted body weight as well as the clinician set maximum pressure are all involved in selecting the VT and respiratory frequency target. Once the target is identified, ASV adjusts both inspiratory pressure of mandatory and/or spontaneous breaths and the mandatory breath rate to maintain the desired breathing pattern (Fig. 1).

Adaptive Support Ventilation adjusts both the inspiratory pressure of mandatory and/or spontaneous breaths and the mandatory breath rate to maintain the desired breathing pattern. VT = tidal volume. f = respiratory frequency. Pinsp = inspiratory pressure.
The calculation of the expiratory time constant also allows ASV to determine inspiratory time and inspiratory/expiratory ratio in the absence of spontaneous breathing. This allows the system to adapt to varying lung pathology and to adjust the inspiratory/expiratory ratio appropriately. The ability of ASV to select appropriate breathing patterns based on obstructive versus restrictive pathology has been confirmed in a large study of patients in a mixed-ICU setting.66 During spontaneous breathing with the patients respiratory rate above the respiratory rate target, only PSV is delivered, and ASV is unable to alter the inspiratory/expiratory ratio. A key issue in using ASV for weaning is appropriate selection of the percentage V̇E setting to encourage spontaneous breathing. This has not been well defined and requires clinician judgment for optimum selection.67,68 ASV has been shown to provide adequate ventilation from initiation of support until ventilator discontinuation.66–67
Adaptive Support Ventilation for Weaning After Cardiac Surgery.
A number of studies have evaluated ASV for weaning patients following cardiac surgery.69–74 These are detailed in Table 2. Postoperative cardiac surgery patients are an attractive group for studying ventilator manipulations, as the volume is quite high and the normal time course is well known. However, the very short time of intubation for patients undergoing fast track weaning (3–4 h) and relatively brief duration for more complicated patients (10–12 h) do not allow detection of meaningful differences related to ventilator discontinuation.
Synopsis of Trials Evaluating ASV for Weaning After Cardiac Surgery
Collectively, these studies find few advantages of automated weaning compared to traditional withdrawal of support. There is no consistent reduction in the duration of ventilatory support, and no difference in the requirement for sedation or ventilator manipulations. It is important to note that no negative effects are seen with ASV, and weaning is not impeded. Postoperative cardiac patients are most likely not the best population to evaluate weaning methods. While a convenient population, these patients suffer from the effects of anesthesia, not lung disease.
Adaptive Support Ventilation for Weaning After Respiratory Failure.
There are several trials75–83 evaluating the use of ASV for weaning in patients with acute respiratory failure. One of the earliest trials evaluated adaptive lung ventilation, an early version of ASV that included measurement of end-tidal carbon dioxide (PETCO2).75 This study evaluated the use of adaptive lung ventilation in 27 patients requiring mechanical ventilation. One third of patients had normal lungs, one third had obstructive lung disease, and one third had restrictive lung disease. All patients were evaluated over a 2 hour period after meeting standard weaning criteria. Twenty-two patients were deemed eligible for discontinuation of ventilation after 2 hours and were successfully extubated. Four patients required continued support with PSV near 15 cm H2O and could not be discontinued from ventilatory support. This study is observational in nature, and, while it provided support for further refinements in ASV, it did not confer any advantage to ASV, as there was no comparative group.
Chen et al recently reported their experience of introducing ASV into a 16 bed Chinese ICU where one respiratory therapist was responsible for all the ventilators during the day and there was no coverage at night.77 The authors compared management of patients with ASV over a 10 month period to a matched historical control. The study evaluated 79 patients managed with ASV to 70 patients managed with SIMV and or pressure support. Under these rather unique circumstances the authors demonstrated that patients in the ASV group achieved extubation readiness within one day of enrollment more often (20% vs 4%); achieved weaning readiness more quickly (1 d vs 3 d); and were more likely to be liberated from the ventilator within 3 weeks of enrollment. However, there were no differences in ICU or hospital stay. These findings must take into account the unusual environment and staffing. However, one potential advantage of closed loop ventilation is the ability to continue care in the absence or unavailability of caregivers. This study seems to support this thesis.
Kirakli and colleagues compared ASV to PSV for weaning of patients with COPD. They evaluated 97 patients: 49 in the ASV group and 48 in the PSV group. All patients had a confirmed diagnosis of COPD, were currently on ventilatory support, and were deemed ready for weaning. SBTs using a PSV of 7 cm H2O and lasting 2 hours were performed prior to extubation in both groups. The primary outcome variable was discontinuation from mechanical ventilation, which was defined as independence from ventilatory support > 48 hours following extubation.76
These authors found that patients ventilated with ASV had shorter weaning times (24 h vs 73 h) and equivalent weaning success (71% vs 68%). Similar to the Chinese study, while weaning time was shorter, the stay in the ICU was not statistically different between groups. Additionally, the total duration of ventilatory support was not different (120 h vs 156 h, P = .56).
One criticism of ASV has been the finding that VT may approach 9–10 mL/kg in some patients.66,79–81 This can be overcome by appropriate setting of the maximum pressure value and VT limits. ASV is approaching 20 years of clinical investigation. While this technique can facilitate weaning, it appears to have no clear advantage over manual techniques. However, ASV answers a number of limitations reviewed in Table 1. Closed loop techniques reduce practice variation and provide state-of-the-art care (lung protection in this case), regardless of the environment or the skill and availability of caregivers. I have previously argued that techniques like ASV may provide the most benefit in resource limited environments, compared to academic medical centers where physicians, fellows, residents, and respiratory therapist are plentiful.43 The work by Chen et al appears to support this opinion.77
Intellivent
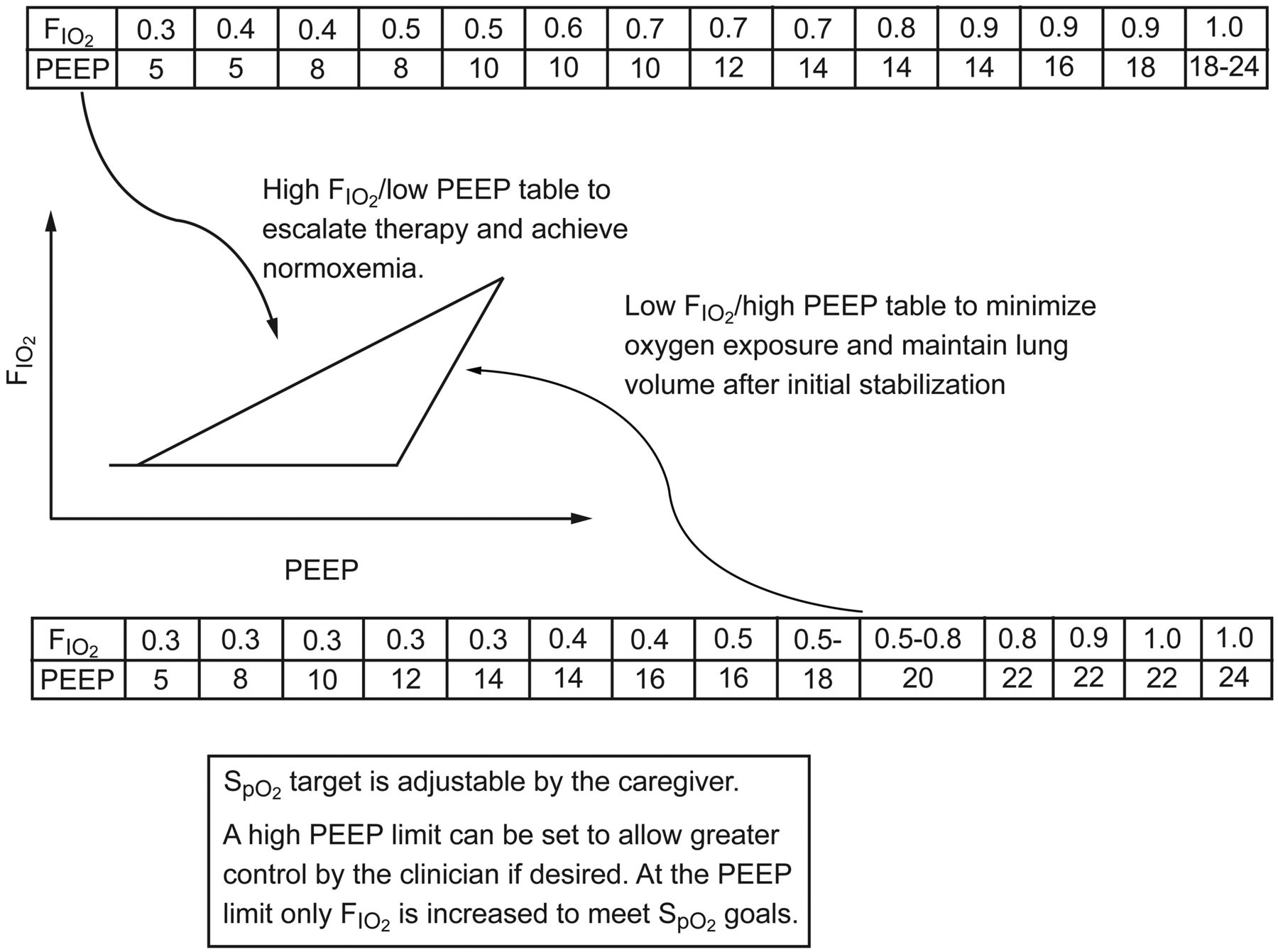
The successor to ASV is Intellivent. This mode combines ASV with closed loop control of PEEP and FIO2. The PEEP/FIO2 controller uses the PEEP tables from the ARDS Network's prospective randomized multi-center trial of 6 mL/kg vs 12 mL/kg VT for treatment of acute lung injury and ARDS (ARMA) and the ARDS Network's prospective randomized multi-center trial of higher end-expiratory lung volume/lower FIO2 versus lower end-expiratory lung volume/higher FIO2 ventilation in acute lung injury and ARDS (ALVEOLI).82,83 The former used an aggressive FIO2 strategy, while the latter is PEEP intensive. A pulse oximeter integral to the ventilator provides feedback to the ventilator, where the clinician can set the desired SpO2. Feedback from the oximeter can also provide information regarding hemodynamic status of the patient, perhaps leading to less aggressive use of PEEP. Intellivent is not commercially available in the United States at present.
The minimum PEEP is 5 cm H2O, and at initiation the controller uses the ARMA PEEP/FIO2 table to reach the desired SpO2. After stabilization the FIO2 and PEEP are weaned using the ALVEOLI table (Fig. 2).
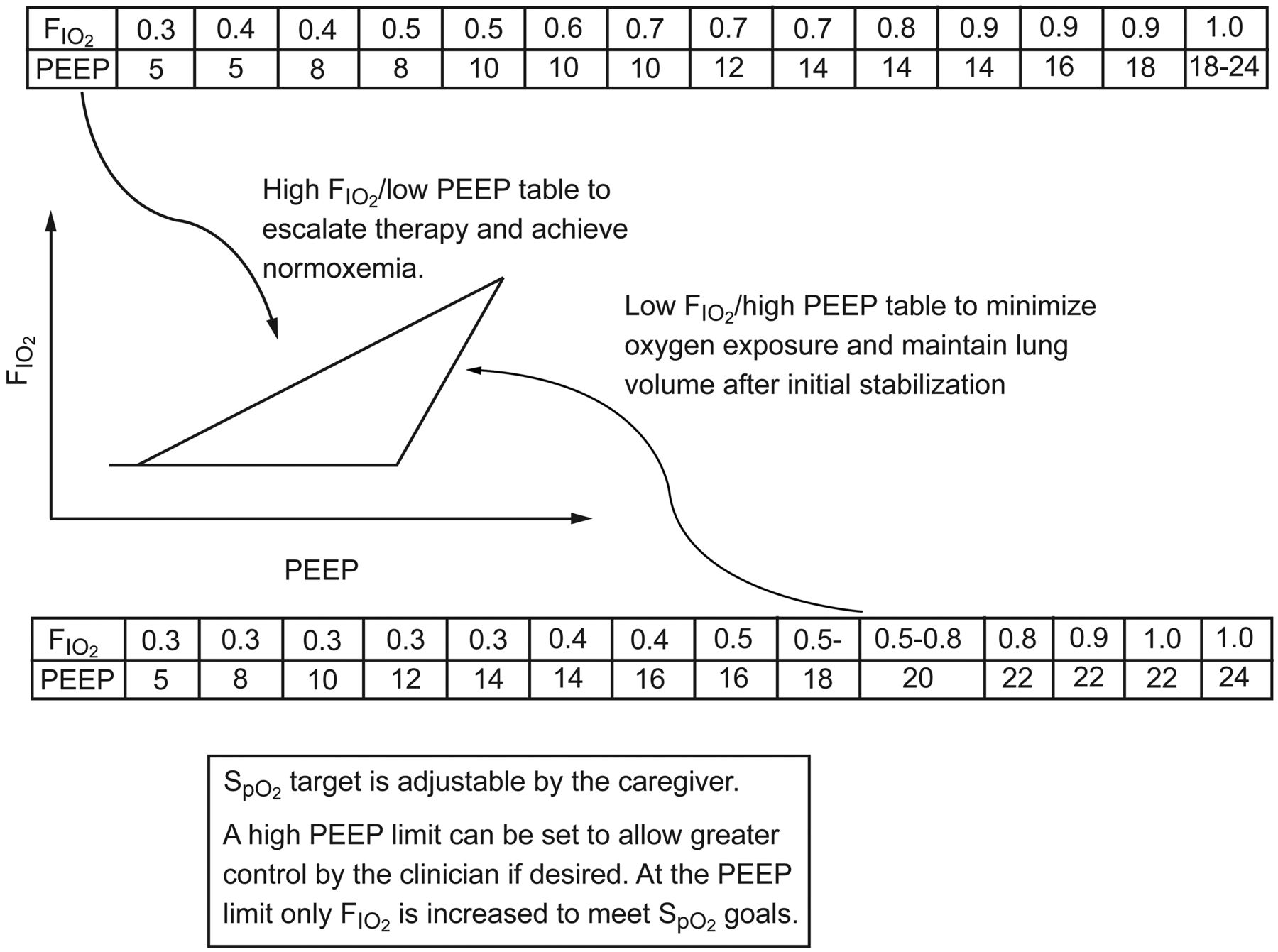
Intellivent mode combines Adaptive Support Ventilation (ASV) with closed loop control of PEEP and FIO2.
Intellivent for Weaning.
Only recently introduced in Canada and Europe, Intellivent has a short list of evidence regarding efficacy and safety. The principles are based in the ARDS Network trials and represent the ability of successful protocols to be introduced via technology. Arnal et al have studied Intellivent versus ASV alone in a 2 hour crossover trial of patients with respiratory failure.84 This study did not address weaning, but demonstrated that in passive patients the system was effective. Compared to ASV alone, Intellivent provided a lower VT and higher PEEP. There was no difference in oxygenation indices, but PaCO2 was slightly higher with Intellivent.
Lellouche et al have presented data in abstract form, comparing Intellivent to protocolized ventilation in patients following cardiac surgery.85 There was no difference in the duration of ventilation, but Intellivent resulted in a lower VT and FIO2 and a greater duration of normoxemia, compared to ASV and manual control of FIO2 and PEEP.
Jouvet et al86 compared Intellivent to ASV during the weaning phase of 15 pediatric patients. Intellivent maintained patients in the normal ventilation range for 94% of the 60 min trial. This feasibility trial demonstrates that Intellivent is capable of maintaining ventilation and oxygenation support during the weaning phase. No weaning advantages were inferred.
Intellivent is the first technique that manages both ventilation and oxygenation autonomously. Further study is warranted to define the utility of Intellivent in the weaning process.
SmartCare/PS
SmartCare/PS describes PSV wherein control of the pressure support level is based on the patient's VT, respiratory rate, PETCO2, and a series of pre-sets based on the patient's condition. (Table 3). SmartCare/PS adjusts the pressure support level in an effort to maintain the patient in a “normal” range of ventilation. A normal range of ventilation is defined as a VT > 300 mL, a respiratory rate > 12 breaths/min and < 30 breaths/min, and PETCO2 < 55 mm Hg (this assumes a patient weighing > 55 kg without COPD or neurologic injury). Outside of the range SmartCare defines other conditions and manipulates the pressure support setting based on the current value, the clinician input parameters, and the patient's historical breathing pattern (Table 4).
Clinician Inputs to SmartCare/PS That Alter Control of the Pressure Support Setting Based on Patient Condition and Care Plan
Defined Conditions Based on Tidal Volume, Respiratory Rate, and PETCO2, and the Ventilator Response During SmartCare/PS (Assumes Weight > 55 kg)
SmartCare/PS was originally called NeoGanesh after the elephant-headed Hindu god of intellect and wisdom, also known as the “gatekeeper.”87 Interestingly, the first use of NeoGanesh was accomplished on a Hamilton Veolar ventilator.88 SmartCare/PS was designed specifically to be an automated weaning system and has several components that make it unique and may lead to its success. The first is that, unlike other closed loop techniques, SmartCare/PS only makes changes to ventilator settings every 2–5 min. While closed loop allows breath to breath changes, it has never been determined what is the optimum time or number of breaths that should be evaluated before a change. This allows the ventilator to withstand perturbations in patient condition that are transient and not associated with a sustained physiologic change. It is also the first system to take into account more than a single variable to guide the single ventilator output (pressure support level). Finally, SmartCare/PS can alert the ICU staff that the patient has reached a period of stability on a minimal level of PSV and can allow them to perform an SBT and suggest ventilator discontinuation. This final feature specifically addresses one of the shortcomings identified in Table 1. Discontinuation of ventilatory support at the earliest possible time is desirable, and recognizing that the patient is ready in a busy ICU with a number of sick patients is not always accomplished.
SmartCare/PS for Weaning.
The initial study of NeoGanesh demonstrated that closed loop control was able to maintain patients in a respiratory zone of comfort twice as often as traditional pressure support.87 In a follow-up study, Dojat and others demonstrated that NeoGanesh predicted the timing of extubation more reliably than traditional weaning parameters.88 This included comparisons to SBTs and calculation of the rapid shallow breathing index. In 1996, the same group compared 24 hour periods of ventilation with conventional pressure support and the “knowledge based” pressure support system.89 The main outcome was not weaning but, rather, maintenance of the patient in the predefined comfort zone, as defined by respiratory rate, VT, and PETCO2. Similarly to the initial study, the knowledge based system resulted in a 50% increase in the amount of time spent in the comfort zone (93% vs 66%). The time spent with a P0.1 (airway-occlusion pressure 0.1 s after the start of inspiratory flow) > 4 cm H2O (consistent with excessive respiratory work load) occurred 11 ± 17% of the time with the knowledge based system and 34 ± 35% of the time in physician directed PSV.
Bouadma and colleagues used the computer driven system to support 33 patients requiring prolonged ventilatory support.90 They compared the time at which clinicians detected weaning readiness to the time determined by the ventilator. Weaning was successful in 25 patients, with 7 failures and one unplanned extubation. Patients were managed with the closed loop system for a mean of 3 ± 3 days (maximum 12 d). The computer directed system detected weaning readiness earlier than the intensivists in 17 patients, intensivists earlier than the ventilator in 4 patients, and the times coincided in 11 patients. This was not a comparative trial, but it demonstrated that the system could manage patients for a prolonged period of time and that the system identified patients ready for ventilator discontinuation earlier than the ICU staff. This addresses one of the limitations of current technology.
The largest trial comparing SmartCare/PS to conventional weaning, in 5 ICUs, was published in 2006.91 Lellouche et al found that SmartCare/PS reduced weaning duration from a median of 5 days to 3 days (P = .01) and total duration of mechanical ventilation from 12 days to 7.5 days (P = .003). The reintubation rate did not differ between groups (23% vs 16%, P = .40). Patients on automated weaning also had a shorter median ICU stay (15.5 d to 12 d, P = .02). No adverse events attributable to the ventilation mode were reported. Sedation requirements were not different between groups. Adherence to recommended modes and daily SBT was estimated at 96% and 51%. This study supports the use of automated weaning, with one caveat. The conventional care group did not have the same adherence to protocols in all 5 centers. This is a valid scientific criticism. However, we know that in routine ICU care around the world, even protocols with a strong evidence base are not followed. The control group in this study may in fact accurately represent the current state of the art.
Rose et al compared SmartCare/PS to conventional weaning in 102 patients in an Australian ICU.92 The median time to successful extubation was 43 hours with SmartCare/PS and 40 hours in the control group. Identification of weaning readiness occurred in 20 hours with SmartCare and 8 hours in the control group. The authors estimated that the probability of reaching “separation potential” was 21% less likely with SmartCare/PS. This ICU had a 1:1 experienced nurse-to-patient ratio and a dedicated weaning protocol. This study is the antithesis to the Chen et al trial evaluating ASV, where the caregiver to patient ratio was 1:16. The authors concluded that closed loop systems may not benefit patients in ICUs with appropriate staffing and aggressive protocols.
Jouvet and others evaluated closed loop weaning in 20 pediatric patients. All patients were ventilated using the computer directed system and compared to a historical control of 20 patients using a clinician decision protocol. The closed loop system successfully ventilated 16 patients and recommended separation from the ventilator in 14. There were no serious adverse events identified. Duration of ventilation was 5.1 ± 4.2 days in the automatic weaning group and 6.7 ± 11.5 days in the control group. There was no difference in the need for reintubation or noninvasive ventilation.93
Kataoka and colleagues evaluated SmartCare/PS in patients following off pump cardiac surgery.94 Ten patients were ventilated using SmartCare/PS and 35 patients were ventilated using PSV and conventional physician directed weaning. The duration of intubation in the SmartCare/PS group was 172 ± 51 min, and 342 ± 239 min in the control group. No adverse effects associated with automatic weaning were noted, and there was no difference in rates of reintubation.
Recently, Schädler et al evaluated SmartCare/PS to a standardized weaning protocol using PSV in 300 surgical ICU patients: 150 patients in each group. Patients requiring > 9 hours of ventilatory support were enrolled in 3 different ICUs.95 There was no difference in the median duration of ventilation between groups (31 h vs 39 h). Comparisons of time in the comfort zone, number of ventilator manipulations per hour, alarms per hour, ICU stay, and 28 and 90 day mortality demonstrated no differences. A subgroup analysis separated patients into 4 categories based on diagnosis. These groups included cardiac surgery (n = 132), COPD (n = 41), and sepsis (n = 44). There were no differences in the COPD and sepsis groups. However, patients in the cardiac surgery category in the SmartCare/PS group had a shorter duration of ventilation (24 h) versus 35 hours during conventional weaning. There were no differences in complications of mechanical ventilation, incidence of reintubation, or requirement for NIV. Sedation requirements were similar between groups. Interestingly, the most common reason in either group for being outside the comfort zone was a respiratory rate < 15 breaths/min.
Implementation
There are no head to head comparisons of closed loop techniques, save a bench study by Morato et al.96 They compared SmartCare/PS to ASV and mandatory rate ventilation. They created models to simulate 6 clinical scenarios: weaning success, weaning failure, weaning success with extreme anxiety, weaning success with Cheyne-Stokes, weaning success with irregular breathing, and weaning failure with ineffective efforts. They found that, in the presence of anxiety or irregular breathing, the closed loop systems worked according to design, but that Cheyne-Stokes breathing resulted in erratic changes in pressure support. They noted the largest oscillations in ASV, which is easily explained by algorithm designs. The breath to breath changes of ASV are more likely to result in changes in PSV than in SmartCare/PS, where changes are made in 2–5 min increments.
When to use a closed loop weaning method remains to be defined. ASV allows management of the patient during both the acute and weaning phases of ventilation. SmartCare/PS is not meant to support the patient during the acute phase of either hypoxic or hypercapnic respiratory failure. In both cases, when to implement these techniques remains a manual decision made by the clinician. It could be argued that ASV allows the widest range of implementation, but during weaning a clinician still has to reduce the percentage V̇E setting to facilitate withdrawal of ventilator support. The bottom line remains that a clinician has to make the decision when the patient is ready to be assessed for weaning readiness.
While the arguments for using closed loop ventilation advanced in Table 1 have some support, many well staffed ICUs will find this method potentially intrusive and unnecessary. My opinion is that closed loop algorithms, like protocols, are best served caring for the routine patients (which represent the majority of patients we care for), where standardizing care has advantages. Additionally, closed loop control can play a clear role in resource limited environments where patient to caregiver ratio is excessive or the expertise of the staff 24 hours a day is variable.
Passing an SBT is of course just one aspect of discontinuing ventilatory support. Following the SBT, a clinician still has to make the decision to remove the endotracheal tube or perform a tracheostomy, based on the patient's mental status and ability to mobilize secretions and protect the airway. No ventilator mode can make these observations. Another concern is the issue of failure. With a manual SBT the therapist places the patient in some aspect of spontaneous breathing and monitors the success or failure. The etiology of failure can then be identified and addressed. Closed loop systems do not yet provide this valuable feedback. In fact, there might be concern that closed loop control may escalate therapy as appropriate, but without clinician monitoring these changes are not immediately obvious. Status observations and information from the ventilator to the clinician should include both “success” and “failure.” A simple status of green, yellow, and red may be helpful in conveying the information that the patient is progressing as desired, is stalled, or is regressing. These issues need to be resolved.
A difficult issue is cost. The addition of ASV or SmartCare/PS to your current ventilators or the additional cost of a new ventilator fleet is not inconsequential. If the additional cost is $7,000 per ventilator, you could argue that this is cost prohibitive. If weaning is expedited and complications and costs reduced, quicker weaning of less than 2 dozen patients would easily justify the cost. However, these could not be patients following cardiac surgery. Real impact would have to be seen in patients with > 72 hours of support and demonstrate reduction in days, not hours.
Conclusions
Closed loop control of ventilator weaning is feasible and has been shown to facilitate weaning in certain populations. Staffing ratios, protocol use, and patient condition are all factors in the success or lack of success in the application of automated weaning. It is likely that changes in the demand for mechanical ventilation, severity of patient illness, and staffing issues will make automated weaning more attractive. Clinicians must continue to evaluate these new techniques and provide feedback such that systems can continue to evolve and represent current best practices.
Footnotes
- Correspondence: Richard Branson MSc RRT FAARC, Division of Trauma and Critical Care, Department of Surgery, University of Cincinnati, 231 Albert Sabin Way, Cincinnati OH 45267-0558. E-mail: richard.branson{at}uc.edu.
Mr Branson presented a version of this paper at the New Horizons Symposium, “The Ventilator Liberation Process: A Fresh Look at the Evidence,” at the AARC Congress 2011, held November 5–8, 2011, in Tampa, Florida.
Mr Branson has disclosed relationships with Ikaria, General Electric, Covidien, Hamilton Medical, and Breathe Technologies.
- Copyright © 2012 by Daedalus Enterprises Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.
- 13.↵
- 14.
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.
- 22.↵
- 23.↵
- 24.↵
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.↵
- 43.↵
- 44.
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.
- 71.
- 72.
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.↵
- 80.
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵





{kind=link}
{kind=link}