

Abstract
BACKGROUND: Oxidative stress has been known for having a key role in pathogenesis of many diseases. The aim of this study was to investigate the oxidative stress and also the relationship between antioxidant system statuses and lung function in patients with COPD and smokers and non-smokers subjects.
METHODS: Thirty subjects with COPD, 30 smokers, and 30 healthy non-smokers participated in this study. The investigation included determination of the lung function and the measurements of plasma ceruloplasmin, ferritin, and total antioxidant capacity, and also erythrocyte glutathione peroxidase, glutathione reductase, superoxide dismutase, and catalase.
RESULTS: Plasma ceruloplasmin, ferritin, erythrocyte glutathione peroxidase, and glutathione reductase were not significantly different between the studied groups. Subjects with COPD and smokers had lower catalase and superoxide dismutase activity (P < .001) than the non-smoker group. Levels of antioxidant capacity were significantly lower in subjects with COPD and smokers than in the non-smoker group (P < .001). Regression analysis revealed no correlations between antioxidant status and spirometric data.
CONCLUSIONS: Decreased total antioxidant capacity in plasma of subjects with COPD and smokers suggests an increased oxidative stress in this group. However, no relationship was found between lung function and antioxidant systems status in COPD subjects.
Introduction
Antioxidant systems include antioxidant enzymes such as glutathione peroxidase, superoxide dismutase, and catalase; non-enzymatic antioxidants include ceruloplasmin, ferritin, ascorbic acid, uric acid, thionine, and carotene.1 Under physiological conditions a balance exists between the amount of reactive oxygen species produced in normal cellular metabolism and the endogenous antioxidant defense. An imbalance between the antioxidant capacity and the production of reactive oxygen species leads to oxidative stress, which is associated with the pathogenesis of several human diseases.2
COPD is one of the most common lung diseases and has an increasing incidence worldwide.3 COPD is characterized by a slowly progressive and irreversible decrease in FEV1, and FEV1 reductions are caused by narrowing of airway lumen diameters.4
An oxidant/antioxidant imbalance has been proposed as having a key role in the pathogenesis of COPD.1 The lung is directly exposed to high levels of oxygen, and therefore has to have efficient antioxidant mechanisms.5 Smoking is one of the important factors for development of COPD, and the majority of patients with COPD are smokers.6 Cigarette smoke is a complex mixture of chemical compounds, containing many free radicals and oxidants. Free radicals include superoxide anion, nitric oxide, and hydroxyl radicals.7 There is evidence that increased levels of markers of oxidative stress may be associated with reduced lung function.1
In this study we aimed to confirm the hypothesis that oxidative stress has a key role in patients with COPD and smokers. We therefore measured plasma antioxidant status, including enzyme and non-enzyme antioxidants, and correlated these factors with lung function in healthy non-smokers, healthy smokers, and subjects with COPD.
QUICK LOOK
Current knowledge
Oxidative stress plays a key role in the pathogenesis of many respiratory diseases. Under normal physiological conditions a balance exists between the amount of reactive oxygen species and the antioxidant defense. An imbalance leads to oxidative stress.
What this paper contributes to our knowledge
Decreased total antioxidant capacity in patients with COPD and smokers suggests increased oxidative stress. No relationship was found between lung function and antioxidant systems status in COPD patients.
Methods
Subjects
Thirty subjects with COPD participated in this study. Their disease was diagnosed by a respiratory physician in Ekbatan Hospital, Hamadan, Iran. The participants were requested to fill in a questionnaire for identifying their demographic characteristics. In order to confirm the COPD diagnosis, a trained observer assessed spirometry and airway reversibility in all subjects. At least 3 acceptable maneuvers meeting American College of Chest Physicians standards were required, with at least 2 reproducible FEV1 and FVC maneuvers within 5% of best required for each test.8 The airway responsiveness was performed in a standardized fashion.9 The subjects had COPD as indicated by the criteria of the American Thoracic Society.10 The clinical condition of the subjects was stable in the month prior to entry into the study. Exclusion criteria included chronic respiratory failure, asthma, coronary disease, and chronic metabolic diseases.
Thirty healthy smokers recruited from the general population, with no specific pulmonary disease, and none of them receiving any medication, and specifically any inhaled bronchodilators or corticosteroids, participated in the study. The World Health Organization definition for smoker applied to the smokers who participated in the study.11
Thirty healthy non-smokers participated in this study as the control group, and had no history of lung disease. All the participants in this study were selected using convenience sampling. All participants gave written informed consent, and this project was approved by the ethical committee of Hamadan University of Medical Science.
Blood Sampling
With each subject we drew 7 mL of venous blood into a heparin tube, centrifuged it at 1,000 g for 15 min, and the plasma was removed. Then erythrocytes were washed with 0.9% NaCl solution 3 times and kept at −80°C until biochemical determination.
Glutathione peroxidase (GSH-Px) activity was measured with the RANSEL,SC692 kit (Randox Laboratories, Crumlin, United Kingdom)). GSH-Px catalyzes the oxidation of glutathione by cumene hydroperoxide. In the presence of glutathione reductase and NADPH (nicotinamide adenine dinucleotide phosphate hydrogen) the oxidized glutathione (GSSG) is immediately converted to the reduced form with a concomitant oxidation of NADPH to NADP+. The decrease in absorbance at 340 nm is measured and expressed as U/g Hb.
Superoxide dismutase (SOD) activity was detected with the RANSOD, SD125 kit (Randox Laboratories, Crumlin, United Kingdom). This method employs xanthine and xanthine oxidase to generate superoxide radicals, which react with 2-(4-iodophenyl)-3-(4-nitrophenol)-5-phenyltetrazolium chloride to form a red formazan dye. The superoxide dismutase activity is then measured by the degree of inhibition of this reaction. One unit of SOD activity causes a 50% inhibition of the rate of reduction of 2-(4-iodophenyl)-3-(4-nitrophenol)-5-phenyltetrazolium chloride under the conditions of the assay. Activity is expressed as U/g Hb.
Catalase activity was determined using the Luck method, as described by Karincaoglu et al.12 Briefly, the decomposition of H2O2 was measured spectrophotometrically at 240 nm.
Total antioxidant status was measured with kit NX2615 (Randox Laboratories, Crumlin, United Kingdom). ABTS (2, 2′-Azino-di-[3-ethylbenzthiazoline sulfonate]) is incubated with a peroxidase (metmyoglobin) and H2O2 to produce the radical cation ABTS*+. This has a relatively stable blue-green color, which is measured at 600 nm. Antioxidants in the added sample cause suppression of this color production to a degree that is proportional to their concentration.
Plasma ferritin was determined by enzyme-linked immunosorbent assay (ELISA) kit (2825–300A, Monobind, Lake Forest, California), according to manufacturer's instruction.
Ceruloplasmin in plasma was measured according to its oxidase activity, as reported by Schosinsky et al.13 The enzymatic activity of ceruloplasmin is expressed in international units, in terms of consumed substrate.
The data are expressed as mean ± SD, and statistical analysis was carried out using statistics software (SPSS 13, SPSS, Chicago, Illinois). Statistical and correlation analysis were performed using analysis of variance test and Spearman correlation coefficient test. A P value < .05 was accepted as statistically significant.
Results
Age and spirometric parameters of the studied groups are summarized in Table 1. Spirometric values FEV1 (% predicted) and FEV1/FVC (% predicted) in subjects with COPD were significantly lower, compared to those of the smoker and non-smoker healthy groups (P < .001). No significant difference in plasma ceruloplasmin and ferritin levels was found between COPD subjects and smoker and non-smoker subjects (Table 2).
Characteristics of Subjects
Antioxidant Values
Significant decreased levels of superoxide dismutase and catalase activities in subjects with COPD and smokers were found, as compared with those of non-smoker healthy subjects (P < .001, see Table 2). Levels of antioxidant capacity were significantly lower in subjects with COPD and smokers than in the non-smoker group (P < .001, see Table 2).
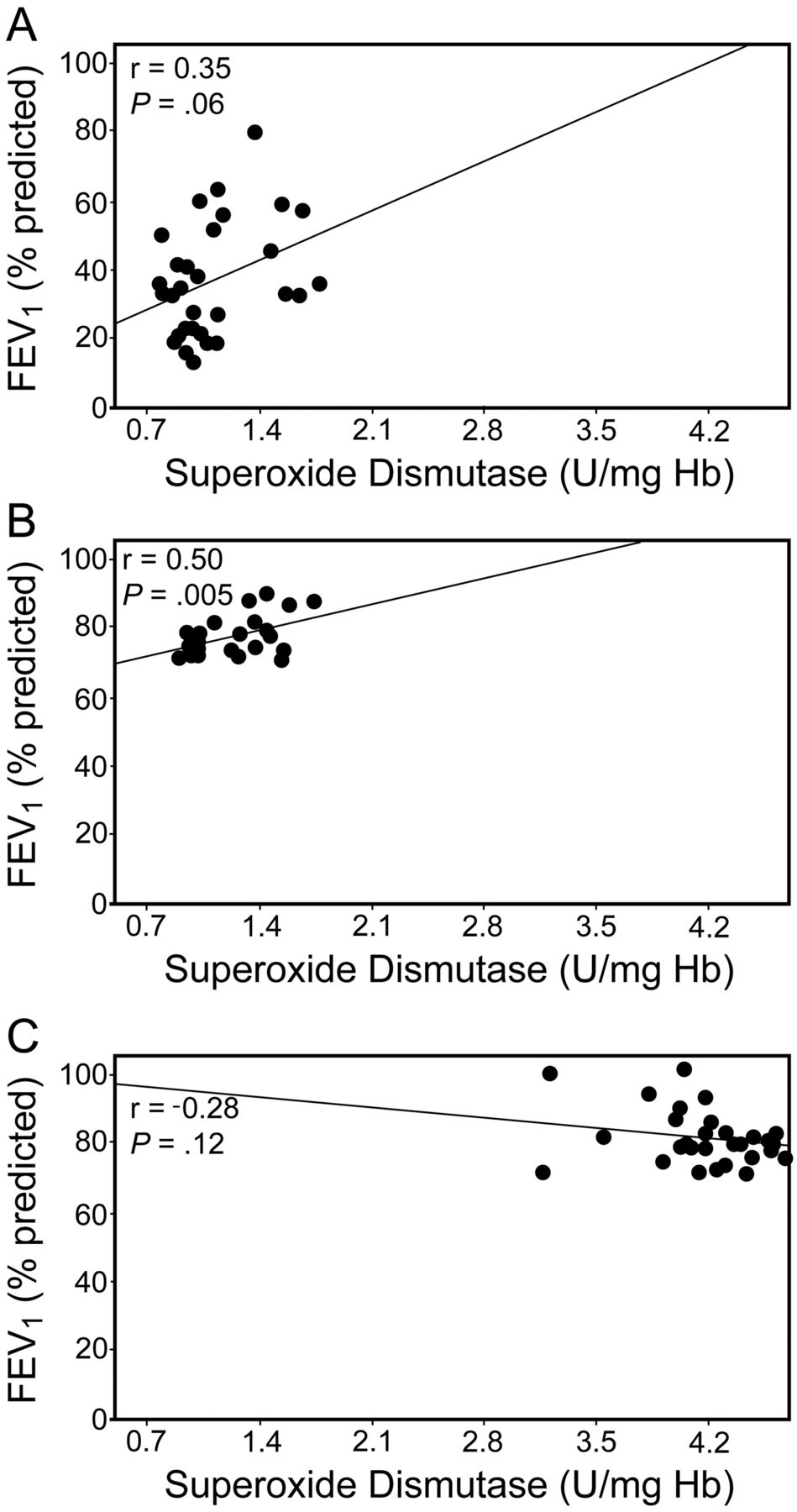
Plasma glutathione peroxidase and glutathione reductase activities in non-smokers, smokers, and in subjects with COPD did not show any significant difference (see Table 2). There was no correlation between the spirometric value (FEV1) and antioxidant status in subjects with COPD or healthy non-smokers (Figs. 1 and 2).

Relationship between lung function, measured as FEV1, and superoxide dismutase (SOD) in (A) subjects with COPD, (B) smokers, and (C) non-smokers.

Relationship between lung function, measured as FEV1, and plasma antioxidant capacity in (A) subjects with COPD, (B) smokers, and (C) non-smokers.
FEV1 values positively correlated with erythrocyte superoxide dismutase activities in smokers (r = 0.50, P = .005, see Fig. 2), and FEV1/FVC negatively correlated with plasma ferritin levels in the smokers group (r = −0.52, P = .003).
Discussion
One of the most important lung diseases caused by cigarette smoking is COPD, which is an indicator of the amount of smoking in a country.14 Some studies have shown that there is oxidative stress in the lung and systemic circulation in COPD.15,16 The role of antioxidant defense mechanisms in COPD and alteration of these systems have been less revealed.
In this study we investigated enzymatic and non-enzymatic antioxidant defense systems, and our results showed significantly lower catalase activities in erythrocytes of smoker and COPD groups, in comparison with healthy non-smoker group. Catalase is the major enzyme associated with hydrogen peroxide destruction, and is expressed in the intracellular alveolar macrophages and neutrophils.17 Mak et al have shown that erythrocyte catalase activity increased in patients with COPD, which is different from our finding.18 However, some studies demonstrated that antioxidant enzyme may be down-regulated during severe or chronic oxidant exposure in an animal model.19
Our results showed that SOD activity is significantly lower in smokers and COPD subjects than in non-smoker subjects. This enzyme is the only enzyme family with activity against superoxide radicals, and is mainly a cytosolic enzyme that expresses in the bronchial epithelium of human lung.20 This decrease can possibly be due to the response to increased reactive oxygen species production, which with severe or chronic oxidant exposure conditions may be inadequate to detoxify high levels of reactive oxygen species. Additional studies are required to show the exact mechanisms that decrease catalase and SOD activities.
Based on our findings, there was no significant difference in plasma glutathione peroxidase and glutathione reductase activities in non-smokers, smokers, and subjects with COPD, and this finding is compatible with the work of Montaño et al.21 Glutathione peroxidase is synthesized in bronchial epithelial cells, alveolar macrophages, and other lung cell lines, and is induced by hypoxia and decreased by exposure to ozone.22
We did not find a significant difference in plasma ceruloplasmin and ferritin levels in healthy non-smokers, smokers, and subjects with COPD. Ferritin level in COPD was lower but not significantly, when compared to non-smokers, and this may lead to a high level of free iron. Iron concentration in alveolar macrophages and lining fluids of smokers is greater than in non-smokers.23 Ferrous iron (Fe++) can produce hydroxyl radicals, which are a potent oxidant.24 Because of high reactivity, iron is bound to compounds such as ceruloplasmin and ferritin. There are some studies that confirm that oxidants can release iron from ferritin.25
As observed in the present study, total antioxidant capacity in plasma of subjects with COPD and smokers was significantly lower than in the non-smoker group. Plasma has important antioxidant systems, including enzymatic and non-enzymatic antioxidant, which can provide a protective environment against oxidative stress. A decreased total antioxidant capacity in plasma suggests an increased oxidative stress. Other studies have shown that smoking can produce oxidative stress and that smokers have low plasma antioxidant defenses.26 Although smoking plays a key role in lung diseases such as COPD, and cigarette smoke contains millions of oxygen free radicals,14 further studies are necessary to disclose the exact mechanisms primarily responsible.
Our correlation studies have shown that there is no significant correlation between spirometric data and antioxidant system status in healthy non-smokers or subjects with COPD, and this finding at least is partly compatible with the work of Rahman et al.1 Reasons for the lack of a significant correlation may relate to variability in the consumption of dietary antioxidants, which may result in different oxidative stresses, depending on conditions.
A significantly positive correlation was observed between FEV1 and erythrocyte SOD activities in the smokers group. Based on our data, FEV1/FVC negatively correlated with plasma ferritin levels in the smokers group. This alteration may relate to either effects of cigarette smoke on gene expression, such as induction of SOD,19 or exogenous dietary antioxidant.
Based on our knowledge, a limited number of factors that are involved in the oxidative stress and COPD have been measured in previous studies, while this study took into account more factors simultaneously (enzymatic and non-enzymatic, and also lung function), which can be counted as a strength of the study. Also, few studies have involved 3 groups (COPD, smokers, and non-smokers), and no similar study was found in this geographical region.
The present study had some limitations. First, our sample size did not allow the detection of some differences. Second, differences in the intake of dietary antioxidants might affect the results. Third, the method of sampling was not randomized. The other factor that can be mentioned as a limitation of the study is our not having considered the physical activity of subjects.
Conclusions
In conclusion, our observations suggest the presence of an oxidative presence in smokers and in subjects with COPD and that the imbalance may be important in the pathogenesis of this disease. The antioxidant status did not correlate with spirometric data in subjects with COPD. Further research is required to reveal the exact mechanism of oxidative stress in subjects with COPD and the effects of smoking. Measurement of these factors in lung tissue may also result in a more accurate assessment.
Footnotes
- Correspondence: Mohammad Taghi Goodarzi PhD, Research Center for Molecular Medicine, Hamadan University of Medical Sciences, Hamadan 65178 Iran. E-mail: mt.goodarzi{at}umsha.ac.ir.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}