

Abstract
BACKGROUND: Failure of noninvasive ventilation (NIV) is common in patients with COPD admitted to the ICU for acute hypercapnic respiratory failure (AHRF). We aimed to assess the rate of NIV failure and to identify early predictors of intubation under NIV in patients admitted for AHRF of all origins in an experienced unit.
METHODS: This was an observational cohort study using data prospectively collected over a 3-year period after the implementation of a nurse-driven NIV protocol in a 24-bed medical ICU of a French university hospital.
RESULTS: Among 242 subjects receiving NIV for AHRF (PaCO2 > 45 mm Hg), 67 had cardiogenic pulmonary edema (CPE), 146 had acute-on-chronic respiratory failure (AOCRF) (including 99 subjects with COPD and 47 with other chronic respiratory diseases), and 29 had non-AOCRF (mostly pneumonia). Overall, the rates of intubation and ICU mortality were respectively 15% and 5%. The intubation rates were 4% in CPE, 15% in AOCRF, and 38% in non-AOCRF (P < .001). After adjustment, non-AOCRF was independently associated with NIV failure, as well as acidosis (pH < 7.30) and severe hypoxemia (PaO2/FIO2 ≤ 200 mm Hg) after 1 hour of NIV initiation, whereas altered consciousness on admission and ventilatory settings had no influence on outcome.
CONCLUSIONS: With a nurse-driven NIV protocol, the intubation rate was reduced to 15% in patients receiving NIV for AHRF, with a mortality rate of only 5%. Whereas the risk of NIV failure is associated with hypoxemia and acidosis after initiation of NIV, it is also markedly influenced by the presence or absence of an underlying chronic respiratory disease.
- noninvasive ventilation
- acute respiratory failure
- acute-on-chronic respiratory failure
- cardiogenic pulmonary edema
- COPD
- hypercapnic coma
- endotracheal intubation
Introduction
Noninvasive ventilation (NIV) reduces the rates of intubation and mortality in patients with severe exacerbation of COPD1,2 or cardiogenic pulmonary edema (CPE).3 In our ICU, NIV has been used since the late 1980s, and was shown by Brochard et al4 to be beneficial in patients admitted with exacerbation of COPD. A subsequent prospective randomized study demonstrated that NIV was associated with reduced rates of endotracheal intubation and mortality in these patients.5
Several large surveys show that the use of NIV has become widespread in treatment of severe exacerbation of COPD in Europe and in the United States.6–8 Despite the increasing experience with this technique, the rate of NIV failure remains high, between 20% and 30% in COPD patients admitted to ICUs.2,5,9,10 NIV may also be used as first-line management of non-COPD patients having acute hypercapnic respiratory failure (AHRF), but the rate of NIV failure and intubation can exceed 30–40% in this group.8,11,12 In COPD patients the severity of hypercapnia and/or acidosis after initiation of NIV is a major predictor of NIV failure.11,13–15 However, no study has evaluated the impact of the NIV ventilatory settings and respiratory parameters under NIV on outcome, and little information is available on hypercapnic non-COPD patients treated with NIV.
The aims of this study were to assess the rate of NIV failure in patients admitted for AHRF, whatever the cause, in an experienced unit, and to identify early predictors of intubation under NIV. Some of the results of this study have been previously reported in the form of an abstract at the 2012 meeting of the European Society of Intensive Care Medicine in Lisbon, Portugal.16
QUICK LOOK
Current knowledge
Failure of noninvasive ventilation (NIV) is common in patients with COPD admitted to the ICU for acute hypercapnic respiratory failure. In selected patients the commonly reported failure rate is approximately 30%.
What this paper contributes to our knowledge
With a nurse-driven NIV protocol, the intubation rate was reduced to 15% in patients receiving NIV for acute hypercapnic respiratory failure, with an accompanying mortality rate of only 5%. The risk of NIV failure is associated with hypoxemia and acidosis after initiation of NIV, and is also markedly influenced by the presence or absence of an underlying chronic respiratory disease. Altered consciousness at admission and ventilator settings had no influence on outcome.
Methods
This observational cohort study was conducted in our 24-bed medical ICU at Hôpitaux Universitaires Henri Mondor in Créteil, France. The institutional review board of the French Society for Respiratory Medicine approved this noninterventional study and waived the need for informed consent.
Subjects
We prospectively included all consecutive patients admitted during a 3-year period (June 2008 to June 2011) and who received NIV as initial ventilatory support for AHRF. AHRF was defined as recent dyspnea with sternocleidomastoid muscle activation and a breathing frequency > 25 breaths/min and/or an arterial pH < 7.35, with a PaCO2 above 45 mm Hg. We excluded patients who were intubated before ICU admission or intubated upon ICU admission without prior NIV, and patients for whom NIV was used with a do-not-intubate order.
NIV Protocol and Definitions
The study was conducted after the implementation, in June 2008, of a nurse-driven NIV protocol that included prospective daily collection of clinical data and ventilatory parameters on a specific NIV monitoring form. When the NIV form was unavailable or incomplete, data were retrieved from the subject's records.
All stages of the protocol had been developed within a multidisciplinary working group including ICU physicians, nurses, and respiratory therapists. A daily NIV prescription by the physician indicated the duration of NIV sessions and targeted expiratory tidal volume (around 6–8 mL/kg) and SpO2 (88–92% in subjects with acute-on-chronic respiratory failure [AOCRF], and ≥ 94% in other subjects). Given that respiratory therapists are not present every day and all day long in our unit, the protocol aimed at empowering nurses to adjust the ventilatory settings and to improve the subject's tolerance to NIV. Nurses are not as highly skilled in mechanical ventilation as respiratory therapists in the United States can be, and were not involved in the decision to intubate. The first objective was to reach the targeted expiratory tidal volume and SpO2, and to improve the subject's tolerance to NIV following a simple decision algorithm (see the protocol and algorithm used in the supplementary material at http://www.rcjournal.com).
Pressure-support ventilation was started, using a pressure-support level of 8 cm H2O, a PEEP level of 0 cm H2O, an inspiratory trigger of 3 L/min, and a maximal inspiratory time of 1 second. The nurses then adjusted the ventilatory parameters, including pressure-support level and FIO2, according to the protocol. Pressure-support level was gradually increased by 2 cm H2O steps to reach the target expiratory tidal volume, and PEEP level was then adjusted as prescribed. FIO2 was gradually adjusted by 5% steps to reach the targeted SpO2. NIV was applied intermittently for periods of at least 2 hours, with a minimal duration of 6 hours per day, or continuously in case of hypercapnic coma, and was maintained until signs of respiratory distress improved. An algorithm was used by nurses in case of leaks, which involved repositioning of the mask, then reducing the PEEP by 2 cm H2O, then reducing the pressure-support level by steps of 2 cm H2O until the minimal expiratory volume was reached, and then changing the mask interface. Continuous mandatory ventilation could be used transiently in subjects with hypercapnic coma and triggering insufficient tidal volume despite high pressure support levels.
A mobile cart containing all types and sizes of interfaces was available at the bedside during initiation of NIV. NIV was performed via a non-vented oronasal mask (FreeMotion RT041, Fisher & Paykel, Auckland, New Zealand, or Ultra Mirage, ResMed, San Diego, California), with an ICU ventilator using a dedicated NIV mode (Evita XL, Dräger, Lübeck, Germany, or Engström CareStation, GE Healthcare, Little Chalfont, Buckinghamshire, United Kingdom), equipped with a heated humidifier (MR850, Fisher & Paykel, Auckland, New Zealand).
The following criteria were used for endotracheal intubation: hypercapnic coma with inability to deliver tidal volume, loss of consciousness or persistent hypercapnic coma under NIV, psychomotor agitation making nursing care impossible and requiring sedation, pronounced worsening in signs of respiratory distress with a breathing frequency above 40 breaths/min under NIV, SpO2 remaining below 90% despite FIO2 1.0, and persistent hypotension despite fluid resuscitation requiring vasopressors. Worsening respiratory acidosis or absolute values of pH/PCO2 were not used as criteria for intubation in the absence of other signs cited above.
Data Collection
From the NIV monitoring forms we analyzed the number and duration of NIV sessions, ventilator settings (pressure support level, PEEP, FIO2), ventilatory parameters (SpO2, breathing frequency, expiratory tidal volume), level of consciousness (assessed using the Richmond Agitation-Sedation Scale),17 NIV tolerance (scored from 0 for “poor” to 3 for “excellent”), amount of leaks (scored from 0 for “no leaks” to 3 for “major”), and hemodynamic parameters (heart rate, blood pressure). Poor tolerance was considered as a score of 0 or 1, and major leaks as a score of 2 or 3. Altered consciousness was defined as a Richmond Agitation-Sedation Scale < 0, and coma as a Glasgow coma score ≤ 8. Blood gases were routinely measured 1 hour after initiation of NIV. Clinical data (breathing frequency, SpO2, blood pressure, heart rate, Glasgow coma score) and blood gases at admission before NIV initiation were retrospectively collected from the medical chart. An independent pulmonologist classified subjects according to the underlying cause of AHRF into one of 3 subgroups: CPE, AOCRF (including subjects having chronic respiratory failure associated with COPD or with other, non-COPD causes), and non-AOCRF, which included subjects without underlying chronic respiratory disease.
Statistical Analysis
Data are expressed as mean ± SD, median and IQR, or number and percent (for dichotomous variables). Qualitative data were compared using the chi-square test, and quantitative data using the unpaired Student t test or Kruskal Wallis test.
To evaluate independent factors associated with NIV failure at admission, univariate risk factors with a P value < .10 were examined using backward stepwise logistic regression analysis. Among related significant univariate factors, only the most clinically relevant were entered into the regression model in order to minimize the effect of collinearity. We therefore included the cause of AHRF, tachypnea, and altered consciousness at admission, and hypoxemia and respiratory acidosis after NIV initiation, whereas Simplified Acute Physiology Score II was not entered into the model. We considered 2-tailed P values < .05 as significant. The statistical analysis was performed using statistics software (Stata 10.1, StataCorp, College Station, Texas).
Results
Subjects
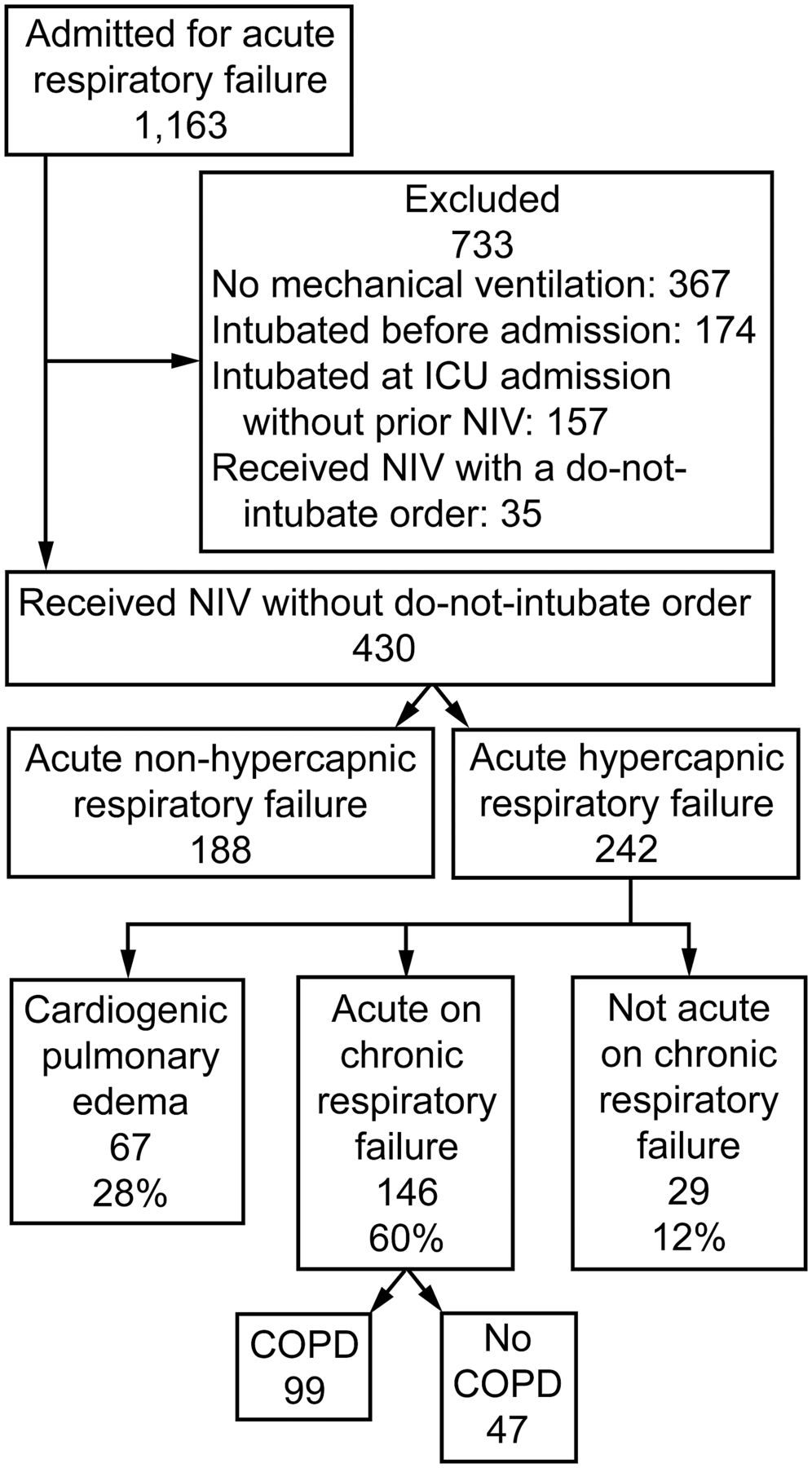
Over the 3-year period, 242 subjects received NIV for AHRF, including 67 with cardiogenic pulmonary edema (CPE), 146 with AOCRF, and 29 with non-AOCRF (Fig. 1). Prospective data on NIV ventilatory parameters was available for 83% (201/242). Among the 47 subjects with non-COPD AOCRF, 30 had obesity and/or obstructive sleep apnea syndrome (median body mass index 38 kg/m2), while others had bronchiectasis (n = 4), permanent ventilatory impairment due to asthma (n = 4), pulmonary cancer (n = 2), chest-wall disease (n = 3), myopathy (n = 2), and myasthenia gravis (n = 2). Among the 29 subjects having non-AOCRF and hypercapnia, 24 had pneumonia (including 8 subjects with clinical criteria for ARDS), and 5 had drug intoxication. The subjects' characteristics at admission and their outcomes in ICU are reported in Table 1. Overall, 31 subjects were comatose either at admission (n = 15) or during the first 24 hours (n = 16).

Flow chart. NIV = noninvasive ventilation.
Characteristics and Outcomes of 242 Subjects Receiving Noninvasive Ventilation for Acute Hypercapnic Respiratory Failure of All Origins
Rates of NIV Failure and ICU Mortality
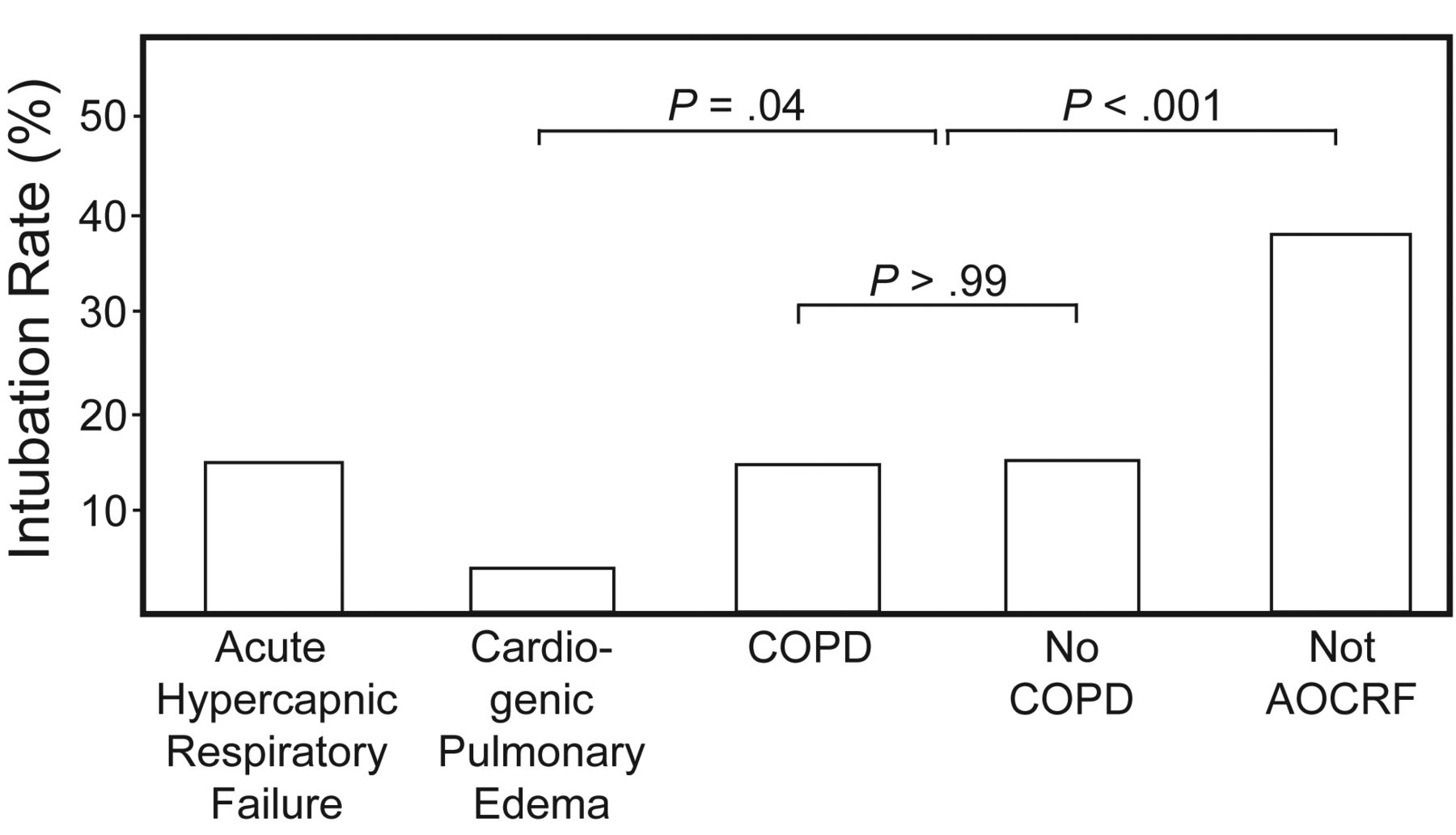
The overall rates of intubation and mortality were respectively 15% (36/242) and 5% (13/242). The intubation rates were 4% (3/67) in CPE, 15% (22/146) in AOCRF—with an identical rate in COPD and non-COPD subjects—and 38% (11/29) in non-AOCRF (P < .001) (Fig. 2). The corresponding ICU mortality rates were 3% (2/67), 5% (7/146), and 14% (4/29) (P = .08) (Fig. 3). The intubation rates were 11% (13/115) in subjects having a pH on admission ≥ 7.30 and 18% (23/128) in those having a pH < 7.30 (P = .15). The in-ICU mortality rate of intubated subjects was 36% (13/36).

Intubation rate in subjects receiving noninvasive ventilation for acute hypercapnic respiratory failure, overall and according to the reason for admission. AOCRF = acute-on-chronic respiratory failure.

ICU mortality in subjects receiving noninvasive ventilation for acute hypercapnic respiratory failure, overall and according to the reason for admission. AOCRF = acute-on-chronic respiratory failure.
Factors Associated With NIV Failure
Among variables recorded on ICU admission, the etiology of AHRF and tachypnea (> 30 breaths/min) was independently associated with NIV failure (Table 2). Non-AOCRF was an independent predictor of NIV failure, as compared to subjects with AOCRF and CPE.
Predictors of Endotracheal Intubation in Subjects Admitted for Acute Hypercapnic Respiratory Failure Receiving Noninvasive Ventilation
Pressure-support level adjusted by nurses was significantly greater 1 hour after NIV initiation than at NIV initiation (9.5 ± 3.0 cm H2O vs 9.2 ± 2.6, P = .036), while tidal volume remained similar (468 ± 144 mL vs 465 ± 135, P = .64). Although not significantly different, expiratory tidal volume 1 hour after NIV initiation tended to be lower in subjects who failed NIV, compared to those who succeeded in NIV.
Among variables recorded at one hour after NIV initiation, ventilatory settings and subject tolerance to NIV or amount of leaks had no influence on outcome, whereas severe hypoxemia (PaO2/FIO2 ≤ 200 mm Hg) and severe acidosis (pH < 7.30) were independently associated with NIV failure.
After adjustment, altered consciousness at admission was not associated with NIV failure and only 23% (14/60) of subjects who had encephalopathy were intubated. Among the 31 comatose subjects, 15 (48%) succeeded in NIV without need for endotracheal intubation.
Discussion
In hypercapnic patients receiving NIV as first-line ventilatory support for acute respiratory failure of various origins, we found that the overall rate of intubation was only 15%. However, this rate differed markedly according to the underlying cause of acute respiratory failure, and reached 38% in patients without chronic respiratory disease (non-AOCRF). Among patients with AOCRF, no difference was found between COPD and non-COPD patients.
Rate of NIV Failure According to the Cause for Acute Hypercapnic Respiratory Failure
The intubation rate of only 4% in subjects receiving NIV for CPE compares favorably with the 14% rate reported in a meta-analysis3 and the 18% rate reported in a survey from the United States.12 Some studies have even reported intubation rates exceeding 20% in the subset of hypercapnic patients.18 Our results are, however, consistent with those of Nava et al,19 who reported an intubation rate of only 6% in hypercapnic patients with CPE treated in an ICU having extensive experience with NIV.
The 15% intubation rate we recorded in subjects with AOCRF is also lower than the 20–30% rates usually reported in studies evaluating NIV in COPD patients.5,8–10,12 Plant et al reported an overall intubation rate of only 15% in patients receiving NIV in respiratory wards, but this rate reached 36% in patients with a pH < 7.30,20 whereas only 18% of our subjects with a pH < 7.30 needed intubation. A recent study reported a rate of NIV failure of only 11% in severe COPD patients admitted to a specialized respiratory ICU,21 with an ICU mortality rate of 8%, which is close to the 5% recorded in our study. In this large observational study, rates of NIV failure and mortality were significantly lower in patients with obesity-hypoventilation syndrome than in those with COPD.21 We found a similarly low risk of NIV failure (15%) in subjects having COPD or another underlying chronic respiratory disease. Indeed, NIV has been successfully used in obese patients with severe obstructive sleep apnea syndrome21–23 or bronchiectasis,24 and may also be effective, despite mixed results, in patients with restrictive pulmonary disease,25 myasthenia gravis,26 or neuromuscular disease.27 Identification of an underlying chronic respiratory disease other than COPD could be of major interest to better assess the risk of NIV failure in hypercapnic patients.
By contrast, we found a markedly higher rate (38%) of NIV failure in hypercapnic subjects with non-AOCRF, mostly associated with pneumonia. High intubation rates of 38%12 or 47%11 have already been reported in non-COPD patients receiving NIV for AHRF when including patients with and without underlying chronic respiratory disease.11,12 In patients having de novo acute hypoxemic (non-hypercapnic) respiratory failure and no chronic respiratory disease, even higher intubation rates of up to 60% have been reported.8,12 It is noteworthy that the intubation rate in our subgroup of patients having de novo acute hypercapnic respiratory failure was only 38%, and that, although significantly less hypercapnic, they were not more hypoxemic than the others 2 subgroups.
Predictive Factors for NIV Failure After NIV Initiation
A higher severity score is usually associated with NIV failure in hypercapnic patients.11,15,28 However, using the Simplified Acute Physiology Score II is clinically impractical since this score is computed only at 24 hours after admission, therefore taking into account any potential complications of intubation in patients who failed NIV within the first 24 hours.
The severity of hypercapnia and/or respiratory acidosis after initiation of NIV is a well known predictor of NIV failure.11,13–15,29 Probably because we included AHRF of all origins, we also found that severe hypoxemia (PaO2/FIO2 ≤ 200 mm Hg) was an independent predictor of intubation in hypercapnic subjects.
By contrast, tolerance to NIV and amount of leaks had no impact on NIV failure. In a survey from 70 ICUs, poor NIV tolerance was a strong predictor of NIV failure.8 However, this study reported good NIV tolerance in only 27% of patients, and 57% had high levels of leaks. In our series, 86% of subjects had good NIV tolerance, and only 10% had high levels of leaks, probably due to our NIV protocol. Pressure-support level was significantly increased during the first hour of NIV, suggesting that the protocol was correctly applied by nurses. With such good NIV tolerance during the first hour of NIV, the ventilatory parameters or ventilator settings had no influence on outcome. However, the trend toward a lower tidal volume in patients who failed NIV, as compared to patients who avoided intubation, might suggest the need to increase the targeted tidal volume in patients at high risk of failure.
Clinical Implications
In a general ICU using protocolized care and monitoring of NIV by nurses, the overall rate of intubation in hypercapnic patients receiving NIV for acute respiratory failure could be maintained below 15%. This rate can be used as an upper limit, both for COPD patients and for other patients having a chronic underlying respiratory disease. These results are probably due, first, to our NIV protocol optimizing the patient's tolerance to NIV, and, second, to our conservative intubation criteria, enabling continuation of NIV under close monitoring in some patients with altered consciousness. As expected, the rate of intubation was particularly high in patients with persistently or newly occurring severe altered consciousness. Nevertheless, 48% of our comatose patients achieved NIV without the need for intubation. Several studies have already shown that NIV could be successful in patients with hypercapnic coma.30,31 Moreover, it has been shown that NIV failure was not associated with an increased mortality rate in hypercapnic patients28; thus, delayed intubation in some patients likely did not worsen their outcome. In our study the ICU mortality rate for intubated patients was 36%, which is in line with the 30–40% rate reported in large surveys.12,28 Our results also suggest that, similar to protocols for weaning from mechanical ventilation32 or sedation,33 which enabled reduction of the time to extubation, NIV protocols involving nurses and/or respiratory therapists might reduce the intubation rate.
Limitations
Our study was conducted in a single unit with longstanding experience in the practice of NIV, and therefore our results may not be applicable to other centers with less extensive experience. Experience and nurse-driven protocols may improve tolerance to NIV, and we report a poor tolerance rate of only 14% after 1 hour of NIV. Another limitation is the retrospective nature of the study. However, prospective data collection of ventilatory parameters under NIV was available for a vast majority of our subjects, and, because of the availability of computerized medical charts for all subjects, all those receiving NIV for AHRF could be analyzed.
Conclusions
While the rate of NIV failure is usually around 20 to 30% for acute hypercapnic respiratory failure, we found that the intubation rate could be maintained below 15% in a highly experienced unit, with an overall ICU mortality of only 5%. Our study suggests that an NIV trial should be considered in all hypercapnic patients presenting with acute respiratory failure, even when the risk of failure is high because of coma, whether in patients with AOCRF or in patients without underlying respiratory disease. Interestingly, severe hypoxemia was an independent predictor of NIV failure in hypercapnic patients of all origins, whereas altered consciousness at admission and ventilatory settings had no influence on outcome.
Footnotes
- Correspondence: Damien Contou MD, Réanimation Médicale, Hôpitaux Universitaires Henri Mondor, 51 Avenue du Maréchal de Lattre de Tassigny, 94010 Créteil, France. E-mail: contou{at}club-internet.fr.
Dr Contou presented a version of this paper at the 2012 meeting of the European Society of Intensive Care Medicine, held October 13–17, 2012, in Lisbon, Portugal.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}