

Abstract
BACKGROUND: Patients who require prolonged weaning from mechanical ventilation represent a major challenge in intensive care, and the timed inspiratory effort (TIE) index has been shown to be a clinically valuable tool to predict weaning success.
OBJECTIVE: To evaluate whether weekly serial measurements of the TIE index can predict the success in prolonged weaning.
METHODS: A prospective observational study in which the subjects who started the weaning process off mechanical ventilation underwent weekly measurements of the TIE index. The area under the receiver operating characteristic curve was used to evaluate the accuracy of the TIE index as a predictor of weaning success. A multivariate Cox regression model was developed to test the association of TIE index values of ≥1.0 cm H2O/s with a failure of weaning.
RESULTS: Seventy subjects were selected. Their median (IQR) age was 72 (62–78) y, the median (IQR) duration of mechanical ventilation was 17.5 (14–28) d, and the median (IQR) APACHE II (Acute Physiology and Chronic Health Evaluation) II score was 28 (24–31). Thirty-five of the 70 subjects (50%) died, 22 of them after successful weaning. A total of 224 tests were performed over 56 d. The area under the receiver operating characteristic curve of the TIE index was 0.93. In the analysis of the probability of success during the follow-up (Kaplan-Meier method), a significant difference was obtained in favor of those with a TIE index of ≥ 1.0 cm H2O/s (53% vs 32%, P = .030). In the multivariate Cox regression analysis, values of the TIE index ≥ 1.0 cm H2O/s revealed an inverse, strong, and independent association with failure (hazard ratio 0.36, 95% CI 0.15–0.91; P = .030). The following variables were also found to have an independent but direct association with failure: age and length of time before weaning.
CONCLUSIONS: When measured weekly, a TIE index of ≥1.0 cm H2O/s was a good predictor of success in subjects who required prolonged weaning in our hospital.
Introduction
Weaning is a critical step in the process of transition from mechanical ventilation to spontaneous breathing.1,2 Mechanical ventilation is associated with ventilator-induced diaphragmatic dysfunction, which may start within 18 h of controlled ventilation,3 which leads to respiratory muscle weakness and the inability to sustain spontaneous breathing.4–7 The most recent weaning classification is based on the duration of ventilation after the first weaning attempt.8,9 Therefore, prolonged weaning is defined as the dependence on mechanical ventilation for >7 d after the onset of spontaneous breathing trials. It is estimated that ∼15% of patients with a difficult weaning progress to prolonged ventilation,5,6,8 which results in an increased hospital length of stay, high mortality rate (47%), and elevated costs.4,10–12 Interventions to restore muscle strength and ventilatory independence would be of great value in this setting. In addition, diagnostic tools to evaluate respiratory muscle function could be helpful to guide starting the weaning process.13
Indexes to predict weaning outcomes have been used worldwide for decades, especially in difficult cases.6 Two indexes are among the most used and recommended by the sixth American Thoracic Society and European Respiratory Society consensus8: the relationship between breathing frequency and tidal volume (rapid shallow breathing index), and maximum inspiratory pressure (PImax). In this regard, a recently proposed weaning index, the timed inspiratory effort (TIE) index exhibited a better performance than previously reported indexes.6,13–15 The timed inspiratory effort (TIE) index is calculated as the ratio of the PImax registered after the first 30 s of observation to the corresponding time required to reach this value with airway occlusion for up to 60 s.15 Based on the aforementioned information, we think it is timely to search for tools capable of early identification of the optimum time to initiate the weaning process with a high probability of success. The objective of the present study was to evaluate whether weekly serial measures of the TIE index can predict the success of prolonged weaning off mechanical ventilation in subjects with a tracheostomy.
QUICK LOOK
Current knowledge
Patients requiring prolonged weaning have a high mortality rate. A recently reported weaning predictor, the timed inspiratory effort (TIE) index, combines the ability to generate an inspiratory pressure with the time needed to achieve the maximum inspiratory pressure.
What this paper contributes to our knowledge
In a specific group of subjects with a low level of consciousness and difficult weaning, the TIE index demonstrated good ability to predict weaning outcome. Age and length of time before weaning were found to have a direct association with weaning failure.
Methods
This was a prospective observational cohort study conducted at the ICU of the Hospital Naval Marcílio Dias, Rio de Janeiro, Brazil, from December 2015 to July 2017. Subjects who met eligibility criteria had the TIE index recorded weekly to evaluate its predictive power related to weaning outcome. Subjects were enrolled in the study if they were ages >18 y, had a tracheostomy and a weaning time of >7 d after the first weaning attempt, resolution of the acute phase of the disease that led to mechanical ventilation, adequate cough reflex, and no excessive tracheobronchial secretion. Also, subjects who had any infection under control, stable cardiovascular status (heart rate ≤ 120 beats/min and systolic blood pressure between 90 and 160 mm Hg, no or minimum use of vasopressors), stable metabolic status, hemoglobin > 10 g/dL, adequate oxygenation (arterial oxygen saturation of >90% with FIO2 ≤ 0.4 or the ratio of oxygen blood pressure by inspiratory fraction of oxygen (P/F ratio) ≥150, with a final positive expiratory pressure of ≤ 8 cm H2O, adequate breathing frequency (≤35 breaths/min), supportive pressure of ≤ 20 cm H2O, no significant respiratory acidosis (pH > 7.30), and a Richmond Agitation-Sedation Scale (RASS) score of ≤ 0.16
We excluded patients older than 86 y, with tracheal stenosis, intracranial pressure > 20 mm Hg, on sedation, with severe cardiac insufficiency or hemodynamic instability, with signs of systemic infection and/or reinfection during the weaning process, and discontinuation due to intercurrences. When adopting the RASS, whose score ranges from −5 to 4, patients who scored > 1 were excluded. The consciousness levels of the included cases were categorized as alert and non-alert in which alertness was defined by objective actions such as opening eyes in response to a voice, following simple commands, and/or having a RASS score of −1 to +1. Weaning was considered successful if spontaneous breathing was sustained for ≥ 48 h after withdrawal from mechanical ventilation.6–9,14,17 This study was approved by the research ethics committee of the Hospital Naval Marcílio Dias - Marinha does Brasil (CAAE 50264415.2.000.5256). Informed consent was obtained from every subject whenever possible or from his or her next of kin.
Procedures
All study subjects were on mechanical ventilation with the ventilator model PB840 (Covidien-Nellcor and Puritan Bennett, Boulder, Colorado) and continuously monitored by using the multi-parameter DX 2010 monitor (Dixtal, São Paulo, Brazil). After categorization as prolonged weaning and tracheostomized, subjects on pressure-support ventilation who were able to start the weaning process were followed up weekly by using the timed inspiratory effort index, as measured by the physiotherapist (BLSG). Regardless of the value obtained, all the subjects were placed on our mechanical ventilation discontinuation protocol by using respiratory training with the T-piece attached to low oxygen flow (3–5 L/min). The subjects had daily T-piece trials, with progressing spontaneous breathing time according to the protocol, then were returned to mechanical ventilation.
Criteria to interrupt periods of spontaneous breathing in T-piece trial were the following: agitation and/or anxiety, reduced level of consciousness, diaphoresis, dyspnea and/or cyanosis, SaO2 < 90% or PaO2 < 60 mm Hg, with FIO2 > 0.4, PaCO2 > 50 mm Hg or increased > 8 mm Hg; arterial pH of <7.33 or decreased by ≥0.07, frequency of >35 breaths/min or increased by 50% for 5 min or longer, heart rate of >140 beats/min or a sustained increase or decrease of >20%, mean blood pressure of >130 or <70 mm Hg, and tachyarrhythmias.6–9,14,17 The subjects who demonstrated one or more of these signs during the spontaneous breathing test or within 48 h after discontinuation of mechanical ventilation were labeled as weaning failure and were returned to ventilatory support.6–9,14,18 The decision to return the subject to mechanical ventilation was made by a respiratory physiotherapist (BLSG) and the physician in charge based on the signs of poor tolerance, as described above.
The timed inspiratory effort index and PImax were recorded by using the digital vacuometer MVD 300 (Globalmed, Porto Alegre, Brazil), with a scale of 300 cm H2O, sensitivity of 1 cm H2O, and a sample frequency of 100 ms.14 Before testing, all the subjects were on ventilation by using the pressure-support mode. The subjects were positioned in dorsal decubitus, with the head elevated at 45°, and the tracheostomy cuff was inflated to avoid leakage during the measurement. After tracheal aspiration, the subjects remained connected to the mechanical ventilator with a 1.0 FIO2 for 2 min, aimed at preventing hypoxemia during the measurements.14 The mechanical ventilator was disconnected, and a 10-s spontaneous breathing period ensued (to allow adaptation to the breathing mode without positive pressure).
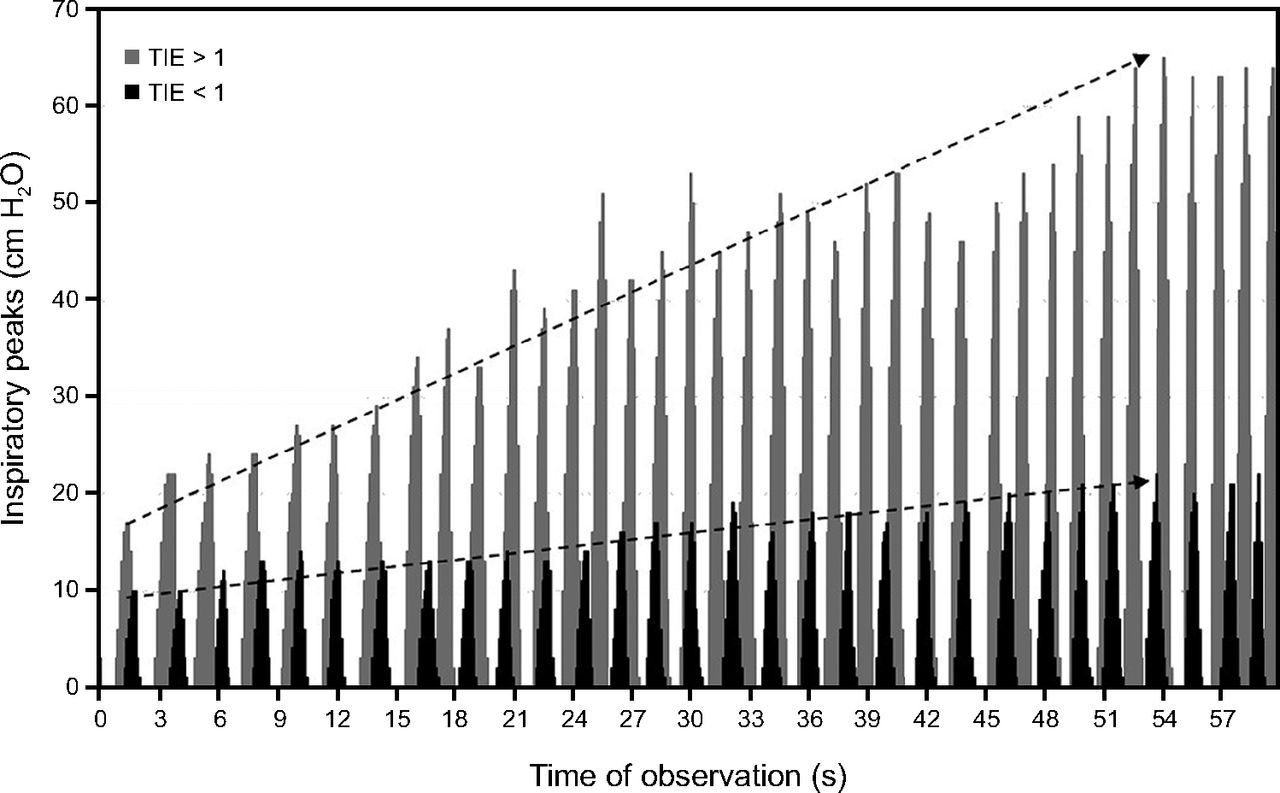
The vacuometer was coupled to the tracheostomy cannula at the end of a normal expiration (at the level of functional residual capacity). The inspiratory pressures, in cm H2O, and their corresponding registration time points, in seconds, were stored and analyzed. Typical plots of the inspiratory pressures versus time with the timed inspiratory effort index of >1 (successful weaning) and of <1 (failed weaning) is depicted in Figure 1). The timed inspiratory effort index was calculated as the ratio of the PImax registered after the first 30 s of observation by the corresponding time to reach during inspiration, whereas keeping the airway occluded during inspiration with a unidirectional valve for up to 60 s.15 The subjects were not coached for the maneuver, which allowed simultaneous determination of the timed inspiratory effort index and PImax. For each subject, the first timed inspiratory effort index was measured at the beginning of the prolonged weaning process and the last was measured the week before successful weaning or death.
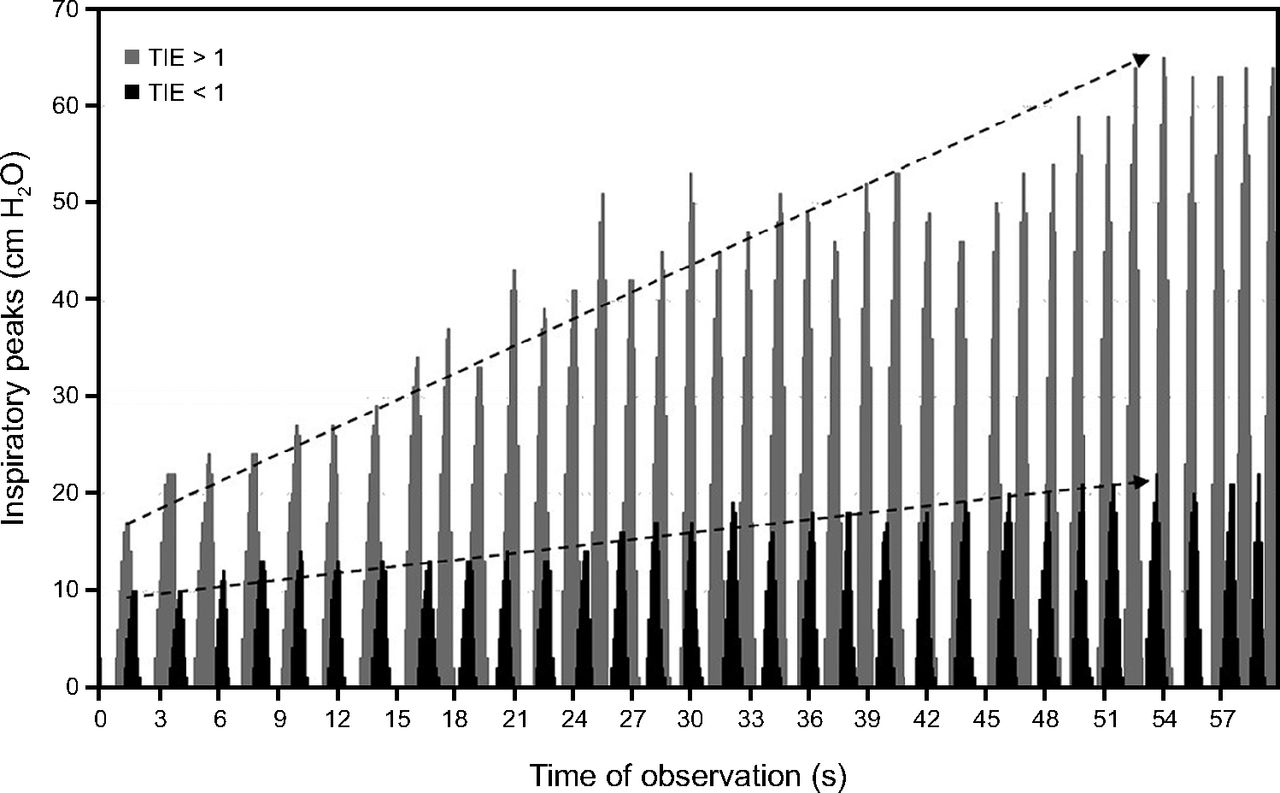
Typical plots of the inspiratory pressure vs time of observation, variables used to calculade the timed inspiratory effort (TIE) index. In gray: TIE = 65 cm H2O/54 s = 1.20 cm H2O/s. In black: TIE = 22 cm H2O/54 s = 0.41 cm H2O/s.
Statistical Analysis
For descriptive statistics, median (IQR), and frequency were used. The following indicators were used to record the performance of the timed inspiratory effort index in predicting the weaning outcome: sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio. The accuracy of the timed inspiratory effort index was also assessed by calculating the area under the receiver operating characteristic curve. The cutoff points were calculated by using the Youden index. The outcomes along the follow-up were shown as Kaplan Meier curves factored by the timed inspiratory effort index and compared by using the log-rank test.
A multivariate Cox proportional hazards regression model was used to test the association with failure at prolonged weaning in which the primary interest variable was the timed inspiratory effort index as a dichotomic variable (values ≥ 1.0). Other variables included for their potential to influence the outcome were age, sex, APACHE II (Acute Physiology and Chronic Health Evaluation II) score, length to start weaning, weaning duration, number of interruptions of weaning trials, and alertness. The level of significance was set at 5%. All statistical analyses were performed by using MedCalc 11.4.2.0 (MedCalc Software, Mariakerke, Belgium) and SPSS 18.0 for Windows (SPSS, Chicago, Illinois).
Results
From a total of 247 patients on mechanical ventilation in the ICU during the study period, 70 subjects were selected for the final analysis. Details about the selection process are depicted in Figure 2. The characteristics of the 70 subjects included in the study are presented in Table 1. A total of 224 tests were performed over 56 d. In 4 subjects (6%), all with a diagnosis of sepsis, the tests were interrupted before the standardized 60 s of airway occlusion. All of these subjects were promptly reconnected to the ventilator and recovered without any consequence.

Flow chart.
General Characteristics of the Subjects
The timed inspiratory effort index was measured weekly, from the beginning of the protocol until the end of the weaning process. Forty-nine subjects were successfully weaned. In the subjects for whom weaning failed, the baseline and final median (IQR) TIE index values were similar, 0.67 (0.44–0.81) cm H2O/s versus 0.65 (0.42–0.77) cm H2O/s, P = .20. In those who were successfully weaned, a statistically significant increase was found in the median (IQR) TIE index, 0.82 (0.65–0.97) cm H2O/s to 1.55 (1.29–2.15) cm H2O/s, (P < .001). A median (IQR) of 3.2 (2–6) timed inspiratory effort index measurements were taken before a value of ≥1.0 was achieved in the subjects who were successfully weaned. The mean time to achieve the PImax was 45.02 ± 11.88 s.
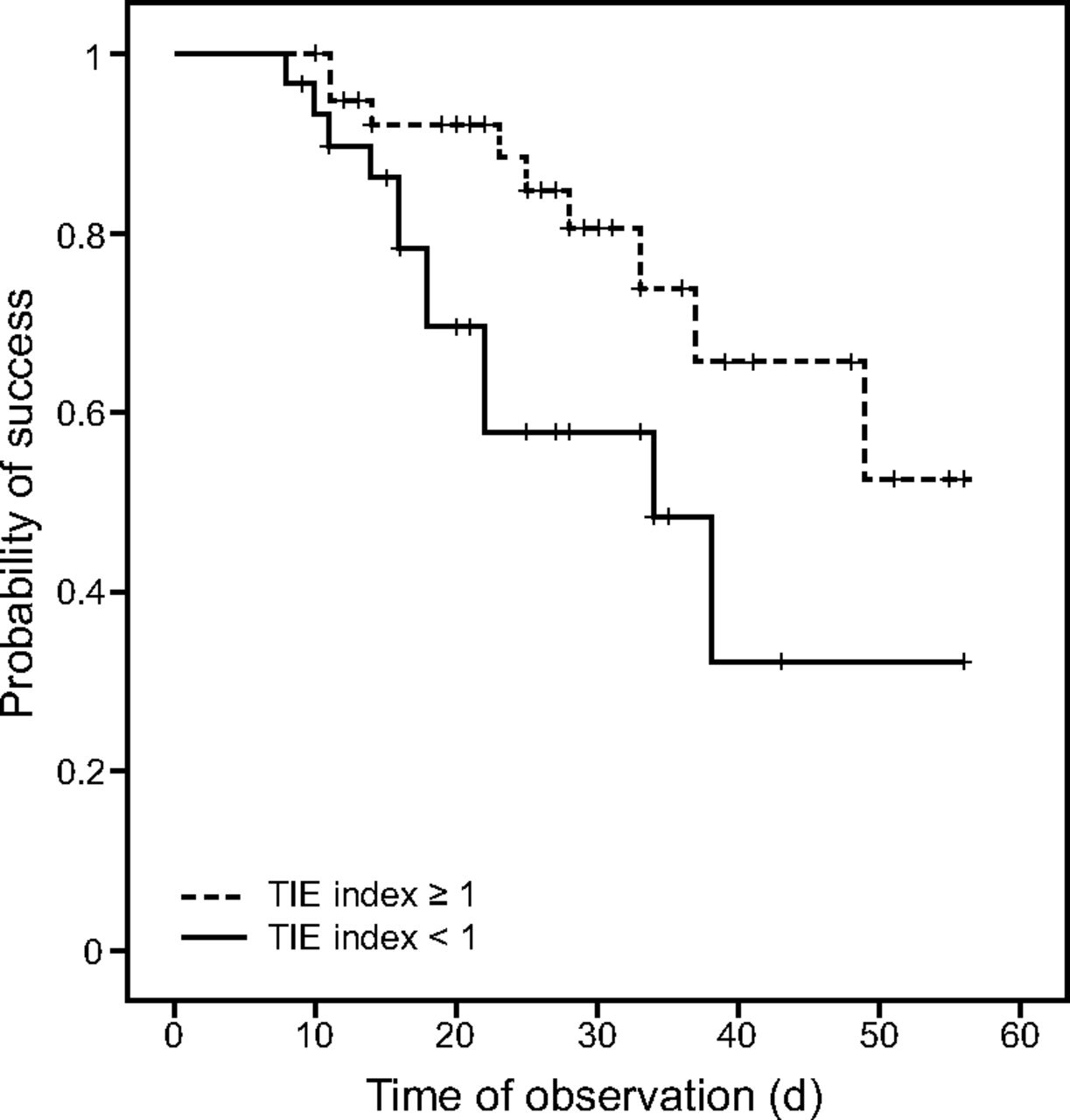
The cutoff points and the results of the TIE index performance (sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio) are presented in Table 2. The area under the receiver operating characteristic curve was 0.93, P = .001 (Fig. 3). In the analysis of the probability of success during the follow-up time (Kaplan-Meier curve), a significant difference was obtained in favor of those with a timed inspiratory effort index of ≥1.0 cm H2O/s (53% vs 32%, P = .030) (Fig. 4).
Quality Indicators of the Timed Inspiratory Effort Index as a Predictor of Successful Weaning

The area under the receiver operating characteristic curve, evaluating the timed inspiratory effort index as a predictor of weaning success. Area under the curve of 0.93, P = .001.

Kaplan-Meier curves, showing the probability of weaning success in subjects with timed inspiratory effort (TIE) of ≥1 cm H2O/s and TIE of <1 cm H2O/s over a 56-d period. P = .030 between groups.
In the multivariate Cox regression model to test the association with failure at prolonged weaning (Table 3), the TIE index of ≥1.0 cm H2O/s revealed an inverse and independent association with the outcome (hazard ratio 0.36, 95% CI 0.15–0.91; P = .030). Age (hazard ratio 1.04, 95% CI 1.01–1.07; P = .03) and the length of time to start the weaning process (hazard ratio 1.03, 95% CI 1.01–1.05; P = .037) also showed an independent association with failure. A trend was also observed toward an association between the number of weaning trial interruptions and outcome, but this was not statistically significant (hazard ratio 3.01, 95% CI 0.91–9.91; P = .07).
Cox Regression Analysis to Test for Association of the Timed Inspiratory Effort With Failure of Weaning Adjusted for Selected Variables
Discussion
We enrolled 70 subjects who were admitted in the ICU and who required mechanical ventilation. The tracheostomy rate was on the high side of those reported in the literature,19 probably due to the severity of disease at ICU admission as assessed by the APACHE II score.20 Weaning outcomes depend on the balance between the ventilator demands and patient capacity. In this sense, respiratory muscle function is an essential factor for the ability to sustain spontaneous breathing without any assistance.21 The present study included a sample of subjects on prolonged weaning, with an average time of 17 d to the start of weaning, which implied that their respiratory muscles were already compromised to some extent.4,5,11
To test if the timed inspiratory effort index would be useful to predict successful weaning in the study group, serial measurements of this parameter were performed from the beginning of the protocol until the end of the weaning process. The most common method to assess respiratory muscle function at the bedside is the PImax. However, some studies have shown that it has low accuracy to predict weaning outcomes, even when using a unidirectional valve.6,13,14,22 Although a recent study found an accuracy of 0.8014,15 when using the unidirectional valve method, the use of the TIE index, which takes into account the time required to reach the PImax within a maximum observation period of 60 s, provided an accuracy of 0.90 in a general sample of subjects in the ICU.14 Accordingly, we found an accuracy of 0.96, which confirmed the TIE index as a useful tool when assessing subjects with respiratory muscle dysfunction during the weaning process.6
In the present study, weaning failure was present in 37% of the subjects, and the ICU mortality was 50%, 22 (31%) of which occurred in subjects who had successful weaning. Our findings can be compared with 2 other studies. In the first study, the weaning failure rate was 47% and in-hospital mortality was 26%.5 In the second study, the weaning failure rate was 53% and ICU mortality was 36.8%, with a hospital death rate of 58.6%.23 The differences observed in our study may be explained, in part, by the advanced age of the subjects (median, 72 y), prolonged duration of mechanical ventilation (median, 17.5 d), high prevalence of infection (58%), and higher APACHE II scores.
The spontaneous breathing trial is the accepted standard to evaluate the success of weaning and extubation of patients on mechanical ventilation in the ICU.8,24,25 However, the failure rate of an spontaneous breathing trial to predict weaning success is ∼15%, whereas the accuracy of the timed inspiratory effort index is ∼90%.14 It is likely that the good performance shown by the timed inspiratory effort index stems is because its measurement considers the muscular response (time) in combination with the performance of the respiratory muscles.8,15 Essentially, a good screening test should include a low number of false-negative results, along with a high number of true-positive results.15,18 In our study, the sensitivity of the timed inspiratory effort index was 86.4% and the specificity was 96.2%. These numbers translated the high reliability of the parameter to predict weaning failure or success.
Many predictive indexes were not incorporated into clinical practice because they presented low accuracy (area under the curve values receiver operating characteristic of <0.80).14,15,18,26 In the present study, the accuracy of the TIE index, measured as the area under the receiver operating characteristic curve, was 0.93, similar to previous studies which showed area under the curve values between 0.90 and 0.96.6,14 It is worth noting that the cutoff point found in the present study, which dealt with subjects with tracheostomy and in prolonged weaning (≥1.0 cm H2O/s), matched the one reported for subjects with difficult weaning and with neuromuscular diseases.6
When the probability of success over a 56-d period was analyzed on a Kaplan-Meier curve factored by the cutoff value of the timed inspiratory effort index, a statistically significant difference was obtained in favor of values ≥ 1.0 cm H2O/s. The finding confirmed our working hypothesis that the weekly serial measurement of the TIE index can help the decision to start the weaning process. In clinical practice, a TIE index of ≥1.0 cm H2O/s could be used as an indication that patients are ready to start the weaning process. Comparisons with previous studies could not be done because the use of the TIE index for this specific purpose is not reported in the literature.
In addition, we used a Cox regression multivariate model to test for the association of timed inspiratory effort index of ≥1.0 cm H2O/s with weaning failure. Even after adjustment for age, sex, APACHE II score, length of time to weaning initiation, weaning duration, weaning trial interruptions, and alertness, the risk of weaning failure was reduced by 64% when the TIE index value was ≥1.0 cm H2O/s. Conversely, the risk rate increased with age, length of time to weaning initiation, and the number of weaning trial interruptions, but statistical significance was not found for the last variable.
Although alertness had no statistical significance in this model, it is considered a determining factor when using tools to measure lung function as well as to achieve ventilatory independence.15,27,28 In this context, patients with a low level of consciousness may present with a low PImax.27–29 However, the technique used for the assessment of the TIE index allows the progressive stimulation of the respiratory center with airway occlusion until no more increases in peak pressures are observed.13,14,27,28 Thus, the TIE index measurement does not require verbal stimulation by the examiner and can be performed in patients who are cooperative as well as in patients who are uncooperative.13,14 In this way, the absence of an association of the alertness with weaning failure in the present study cannot be seen as a surprise. Ventilatory independency mainly depends on an intact respiratory center combined with adequate respiratory muscle strength, variables well assessed during the measurement of the timed inspiratory effort index.13
Our study presented some limitations. The sample size of the present study was relatively small and derived from a sole center, which perhaps limited the generalizability of the findings. Although we had no objective information on the factors that led to a skeletal muscle injury in our sample, the timed inspiratory effort index was helpful to evaluate respiratory muscles function and to predict weaning outcome in subjects who were difficult to wean. Additional studies that confirm our results are needed before recommending such a strategy in clinical practice, and a randomized controlled trial would be needed to see if the timed inspiratory effort index leads to faster liberation from the ventilator.
Conclusions
The weekly serial measurements of the timed inspiratory effort index proved to be efficient in predicting the success of weaning off mechanical ventilation in subjects with tracheostomy and classified as prolonged weaning.
Acknowledgments
The authors thank the respiratory physiotherapists and physicians of the ICU of the Hospital Naval Marcílio Dias (Marinha do Brazil).
Footnotes
- Correspondence: Leonardo Cordeiro de Souza PhD PT, Physical Therapy Service of Hospital Icaraí and Hospital e Clínica São Gonçalo, Rua Marquês de Paraná, 233 – 5o. andar., CEP 24030-215 - Centro, Niterói, Brazil. E-mail: leonardo.uti{at}gmail.com.
This study was partially supported by Universidade Estácio de Sá by a research productivity program.
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}