

Abstract
INTRODUCTION: High-flow nasal cannula (HFNC) can deliver heated and humidified gas (up to 100% oxygen) at a maximum flow of 60 L/min via nasal prongs or cannula. The aim of this study was to assess the short-term physiologic effects of HFNC. Inspiratory muscle effort, gas exchange, dyspnea score, and comfort were evaluated.
METHODS: Twelve subjects admitted to the ICU for acute hypoxemic respiratory failure were prospectively included. Four study sessions were performed. The first session consisted of oxygen therapy given through a high-FIO2, non-rebreathing face mask. Recordings were then obtained during periods of HFNC and CPAP at 5 cm H2O in random order, and final measurements were performed during oxygen therapy delivered via a face mask. Each of these 4 periods lasted ∼20 min.
RESULTS: Esophageal pressure signals, breathing pattern, gas exchange, comfort, and dyspnea were measured. Compared with the first session, HFNC reduced inspiratory effort (pressure-time product of 156.0 [119.2–194.4] cm H2O × s/min vs 204.2 [149.6–324.7] cm H2O × s/min, P < .01) and breathing frequency (P < .01). No significant differences were observed between HFNC and CPAP for inspiratory effort and breathing frequency. Compared with the first session, PaO2/FIO2 increased significantly with HFNC (167 [157–184] mm Hg vs 156 [110–171] mm Hg, P < .01). CPAP produced significantly greater PaO2/FIO2 improvement than did HFNC. Dyspnea improved with HFNC and CPAP, but this improvement was not significant. Subject comfort was not different across the 4 sessions.
CONCLUSIONS: Compared with conventional oxygen therapy, HFNC improved inspiratory effort and oxygenation. In subjects with acute hypoxemic respiratory failure, HFNC is an alternative to conventional oxygen therapy. (ClinicalTrials.gov registration NCT01056952.)
- high-flow nasal cannula
- continuous positive airway pressure
- oxygen therapy
- acute hypoxemic respiratory failure
- inspiratory effort
Introduction
Supplemental oxygen administration is the first-line treatment for acute hypoxemic respiratory failure. Oxygen is usually delivered through a high-FIO2, non-rebreathing face mask.1–3 One limitation with conventional oxygen administration is the substantial mismatch between oxygen flow and the patient's inspiratory flow. The patient's peak inspiratory flow may vary between 30 and 120 L/min during respiratory failure.2,3 An alternative to conventional oxygen therapy has been developed. High-flow nasal cannula (HFNC) is a technique that can deliver heated and humidified gas (up to 100% oxygen) at a maximum flow of 60 L/min via nasal prongs or cannula.4–6 Studies have shown that HFNC can generate flow-dependent, low-level positive airway pressure (PAP),6–9 reduce airway resistance10,11 and flush nasopharyngeal dead space.12–14 Positive expiratory pressure may have a number of benefits in respiratory failure, including improved ventilation/perfusion matching with improved oxygenation, reduced airway resistance, and reduced work of breathing. Moreover, HFNC may improve oxygen administration by decreasing oxygen dilution, decreasing dead space, and providing high levels of humidification. Data on ICU subjects with respiratory failure are scarce.15–18 In these studies, HFNC had a beneficial effect on clinical signs and oxygenation in subjects with acute respiratory failure. However, to our knowledge, a rigorous assessment of inspiratory effort and oxygenation has not been performed.
The aim of this study was to assess the short-term physiologic effects of HFNC compared with those of conventional oxygen therapy delivered via a face mask in subjects admitted to an ICU for acute hypoxemic respiratory failure. We also compared HFNC with CPAP at 5 cm H2O. Our hypothesis was that HFNC and CPAP would reduce the inspiratory effort and subsequently the breathing frequency and improve oxygenation and comfort better than standard oxygen.
QUICK LOOK
Current knowledge
Heated and humidified high-flow oxygen has been shown to improve oxygenation and reduce minute ventilation requirements in patients with respiratory disease. The mechanisms of action include the washout of anatomical dead space of the upper airway, development of a low level of PEEP, and meeting inspiratory demands with sufficient flow.
What this paper contributes to our knowledge
In a small group of 12 subjects, the delivery of heated and humidified oxygen with high-flow nasal cannula (HFNC) was superior to high-flow oxygen via a non-rebreathing mask. Breathing frequency and inspiratory effort were reduced with HFNC compared with the non-rebreathing mask. However, CPAP at 5 cm H2O, was superior to HFNC in improving oxygenation.
Methods
Subjects
Consecutives subjects admitted to the ICU between January 2011 and January 2012 for acute hypoxemic respiratory failure were considered eligible for the study. Inclusion criteria were: acute hypoxemic respiratory failure defined by PaO2/FIO2 ≤ 300 mm Hg on oxygen and lung infiltrates by chest radiograph.3,19 Subjects with tracheostomies were not eligible for the study. Exclusion criteria were: < 18 y of age, chronic retention of CO2, respiratory acidosis (pH < 7.35 and PaCO2 > 45 mm Hg), factors related to insertion of an esophageal catheter (recent gastric or esophageal surgery, active upper gastrointestinal bleeding, poor cooperation), excessive amounts of respiratory secretions, systolic blood pressure of < 90 mm Hg, ventricular arrhythmia, encephalopathy or coma, life-threatening hypoxemia (PaO2/FIO2 < 100 mm Hg), and decision to limit life-support treatments in the ICU.3 An independent review board (Comité de Protection des Personnes Sud-Ouest et Outre Mer) approved the study. Written informed consent was obtained from each subject or next of kin before inclusion.
Study Design
Protocol.
Subjects meeting eligibility criteria were enrolled in the study. Four study sessions with subjects in a semirecumbent position were performed. The first session consisted of conventional oxygen therapy via a high-FIO2, non-rebreathing face mask. Recordings were then obtained during sessions of HFNC and CPAP, in random order, and the final measurements were taken during oxygen therapy delivered via the high-FIO2, non-rebreathing face mask. Each of these 4 periods lasted ∼20 min, so the measurements were completed in < 2 h.
Non-Rebreathing Mask.
Conventional oxygen was given via a high-FIO2, non-rebreathing face mask (Hudson RCI/Teleflex Medical, High Wycombe, United Kingdom). The goal was to achieve an SpO2 of > 90%. At the end of the first non-rebreathing mask session, the FIO2 was measured using a portable oxygen analyzer (MiniOX I, Mine Safety Appliances, Pittsburgh, Pennsylvania). The tip of the oxygen analyzer was introduced via a small hole in the face mask.17
HFNC Device.
We used the Optiflow HFNC device (Fisher & Paykel Healthcare, Auckland, New Zealand). This device consists of an air-oxygen blender with adjustable FIO2 that delivers a modifiable gas flow to a heated chamber (MR850 pass-over humidifier, Fisher & Paykel Healthcare), where the gas is heated and humidified. The gas mixture is then delivered at 37°C via short, wide-bore, bi-nasal prongs. For all subject, gas flow was set at 60 L/min. We used the largest cannula tolerable for each individual subject.
CPAP Device.
The CPAP device used was the BiPAP Vision (Philips Respironics, Murrysville, Pennsylvania) fitted to a face mask (Mirage, ResMed, Sydney, Australia) and connected to an active humidification system (Fisher & Paykel Healthcare). The size of the face mask was chosen to optimize subject comfort while minimizing air leaks. For all subjects, CPAP was set at 5 cm H2O.
The FIO2 measured at the end of the first non-rebreathing mask session served as a reference. We set the same level for HFNC and CPAP sessions, and we checked it at the end of every session using the portable oxygen analyzer.
Measurements
Esophageal Pressure.
Esophageal pressure (Pes) was measured using a single-balloon catheter (Marquat, Boissy-Saint-Léger, France) inserted through the nose (after topical anesthesia) and advanced until the distal balloon was in the middle portion of the esophagus. The balloon was filled with 1 mL of air and connected to a pressure transducer at ± 100 cm H2O (Biopac Systems, Goleta, California). An occlusion test was performed to assess appropriate placement of the esophageal balloon. Gentle manual pressure on the abdomen was applied to verify the absence of pressure fluctuations.20,21 Pressure was digitized on a personal computer at 200 Hz and sampled using an analog-to-digital converter system (MP100, Biopac Systems).
Gas Exchange and Hemodynamic Parameters.
An indwelling catheter was inserted into a radial artery to allow blood gas analysis and systemic blood pressure monitoring at the end of each test period except the final non-rebreathing mask session. Blood gases were measured using an ABL520 analyzer (Radiometer, Brønshøj, Denmark). Systolic and diastolic arterial blood pressures were continuously monitored. SpO2 was monitored continuously. Heart rate and breathing frequency were monitored using an ICU monitor.
Comfort and Dyspnea.
Subject comfort and dyspnea were assessed at the end of each test period. A member of the team (MS-L) asked the subjects to grade the comfort of the different devices using the following scale: 1, severe discomfort; 2, discomfort; 3, acceptable level of comfort; 4, good level of comfort; and 5, very good level of comfort.22 Dyspnea was assessed using a visual analog scale.
Data Collection and Recordings.
Age, sex, primary diagnosis of acute hypoxemic respiratory failure, PaO2/FIO2, and severity of illness assessed using Simplified Acute Physiology Score II were recorded upon enrollment. Data were taken during the last 5 min of stable breathing pattern. After elimination of artifacts produced by coughing and esophageal spasms, mean values were computed over 10–30 consecutive breaths and used for the analysis. To estimate the inspiratory effort, we determined the Pes and the esophageal pressure-time product (PTPes). PTPes/breath was obtained by measuring the area under the Pes signal from the onset of its negative deflection to its return to baseline. The average PTPes/breath (cm H2O × s) was multiplied by the subject's own breathing frequency to obtain PTPes/min (cm H2O × s/min). We recorded the frequency by the variations in Pes.
Statistical Analysis.
Data are reported as the median and interquartile range. We compared the values obtained during the HFNC, CPAP, and first non-rebreathing mask test periods. The small sample size required the use of nonparametric tests. The Friedman test was used for repeated-measures analysis of variance by ranks, and pairwise comparisons were conducted using the Wilcoxon test. The different pairwise comparisons were: HFNC versus first non-rebreathing mask session and HFNC versus CPAP. Because of multiple comparisons, statistical significance was adjusted using the Bonferroni correction. P < .01 was considered statistically significant.
Results
The main baseline characteristics of subjects are reported in Table 1.
Subject Characteristics at Enrollment
Inspiratory Effort
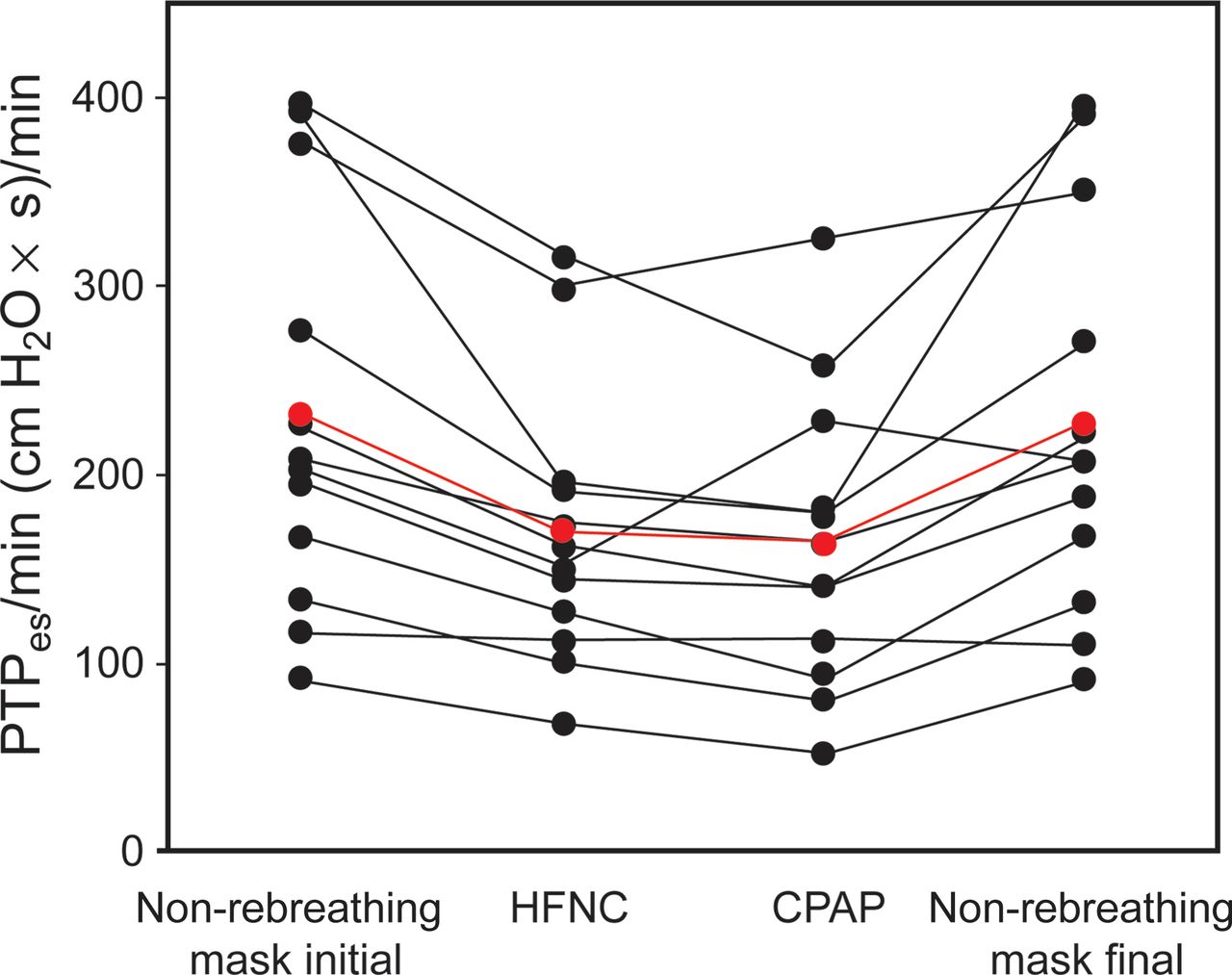
Table 2 lists the main inspiratory effort data, and Figure 1 shows the individual PTPes/min values. Compared with the first non-rebreathing mask session, HFNC reduced the inspiratory effort, as indicated by the reduction in Pes, PTPes/breath, and PTPes/min (P < .01). With CPAP, the inspiratory effort was reduced to a similar extent as with HFNC.
Inspiratory Effort, Arterial Blood Gas Parameters, Comfort, and Dyspnea Score During Study Periods
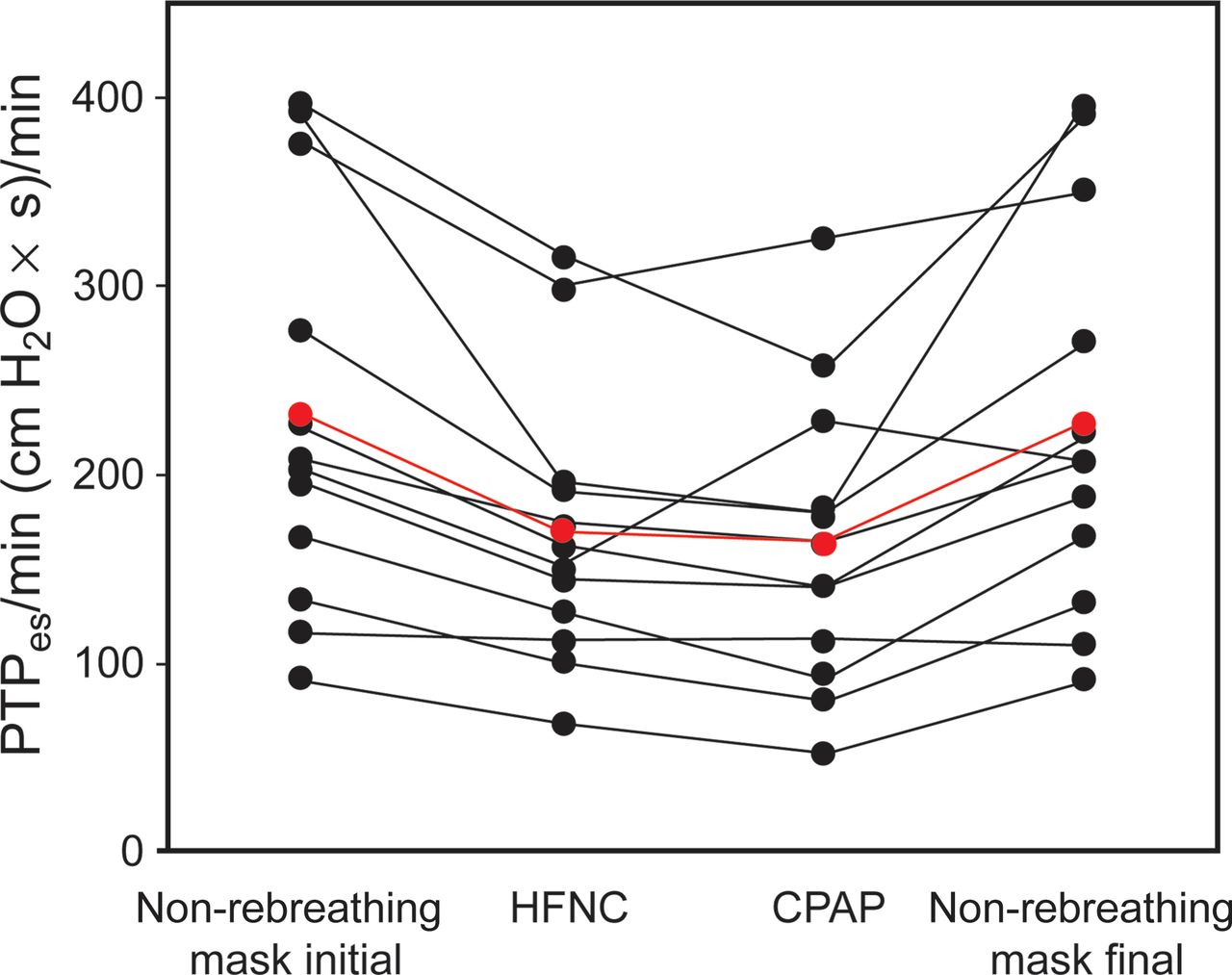
Individual changes in the esophageal pressure-time product (PTPes)/min during the 4 periods. The red line represents the mean values. PTPes/min decreased in all subjects except one with high-flow nasal cannula (HFNC) compared with conventional O2 therapy delivered via a face mask (first non-rebreathing mask session). CPAP produced unloading similar to HFNC.
Effects on Oxygenation and Ventilation
HFNC caused a significant reduction in median breathing frequency compared with the first non-rebreathing mask session (25 [21–33] breaths/min versus 23 [18–25] breaths/min, P < .01). The difference between HFNC and CPAP was not significant (23 [18–25] breaths/min versus 21 [21–32] breaths/min, P = .9) (Fig. 2). Arterial blood gas values were obtained for all subjects. However, gas exchange measurements were not performed in the final non-rebreathing mask session. Table 2 reports arterial blood gas parameters during the study periods. Figure 3 depicts a schematic representation of individual changes in PaO2/FIO2. Compared with the first non-rebreathing mask session, PaO2/FIO2 increased significantly with HFNC (∼10%). However, CPAP produced a significantly greater improvement in PaO2/FIO2 than did HFNC (P < .01).

Box plots summarizing breathing frequency variation during different respiratory sessions. Box plots show median, interquartile range, and outliers (5th to 95th percentiles) of frequency in different periods. HFNC = high-flow nasal cannula.
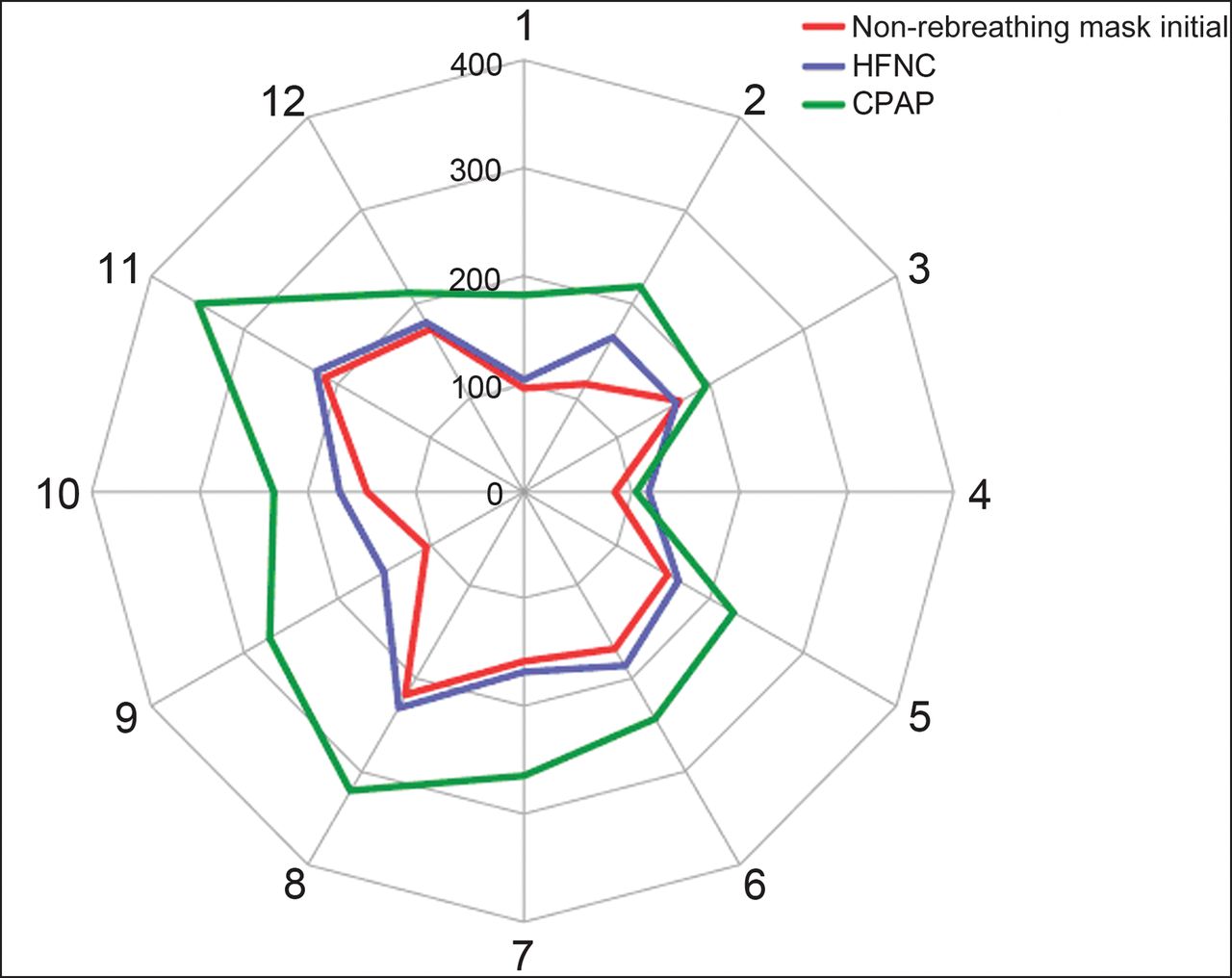
Schematic representation of individual changes in PaO2/FIO2. High-flow nasal cannula (HFNC) induced a significant change in PaO2/FIO2 compared with O2 therapy delivered via a face mask (first non-rebreathing mask session). However, CPAP provided the greatest improvement in PaO2/FIO2. Lines numbered 1–12 represent the 12 subjects studied. The concentric values (100–400) denote PaO2/FIO2 obtained with each device.
Hemodynamic Parameters
Neither mean arterial pressure nor heart rate changed significantly (Table 3).
Mean Arterial Blood Pressure and Heart Rate
Comfort and Dyspnea Score
As shown in Table 2, subject comfort was not different in the 4 sessions. However, dyspnea decreased with HFNC and CPAP, but this improvement was not significant. Seven subjects preferred HFNC, 2 subjects preferred oxygen therapy delivered via a face mask, and one subject found CPAP more comfortable. Two subjects perceived no difference.
Discussion
Main Study Results
Compared with conventional oxygen therapy via a face mask, HFNC resulted in less inspiratory effort and a slight but significant increment in PaO2/FIO2. CPAP produced a significantly greater improvement in PaO2/FIO2 than did HFNC. Tolerance was similar with the 2 methods. Dyspnea improved with HFNC, but this improvement was not significant.
Inspiratory Effort
To our knowledge, this is the first study evaluating the effects of HFNC on inspiratory effort. Nevertheless, we found in the literature indirect evidence of inspiratory effort improvement. Sztrymf et al15 reported their experience with HFNC in 20 subjects with acute hypoxemic respiratory failure. After subjects were placed on HFNC, respiratory distress was rapidly alleviated, with a significant decrease in breathing frequency and a significant reduction in supraclavicular retraction and thoracoabdominal asynchrony.15 In a larger cohort of subjects, the same team confirmed the rapid alleviation of respiratory distress in more severe subjects.16 Several mechanisms may explain the effect of HFNC. The most obvious technique for minimizing the work of breathing during spontaneous ventilation is to decrease airway resistance and recruit collapsed alveolar units. It has been demonstrated that HFNC generates a certain amount of PAP.6–9 In subjects recovering from cardiac surgery, a mean PAP of 2.7 cm H2O was measured at 35 L/min with the mouth closed.7 Chanques et al9 confirmed that HFNC was able to provide a low PAP (< 4 cm H2O).
An increase in airway resistance has been described with cold- and dry-air inhalation.23,24 This may cause a modest increase in ventilatory loading. A heated humidifier noticeably provides much higher levels of humidity.25 One may hypothesize that, during acute hypoxemic respiratory failure, humidified HFNC could decrease airway resistance compared with a poorly humidified conventional oxygen therapy device.26 Shepard and Burger10 demonstrated that, during inspiration, the nose behaves like a variable resistor with a collapsible segment, limiting inspiratory air flow. It is possible that by delivering inspiratory flows higher than those generated by a patient, HFNC opposes this increase in inspiratory resistance, thus reducing the work of breathing.
PaO2/FIO2
We found that HFNC slightly but significantly increased PaO2/FIO2 compared with conventional oxygen therapy. Frat et al27 showed that HFNC significantly improved oxygenation and tachypnea compared with standard oxygen therapy in subjects with acute hypoxemic respiratory failure. HFNC improves oxygenation by various mechanisms, such as decreasing oxygen dilution, reducing dead space, and increasing end-expiratory lung volume and tidal volume.8–11 Corley et al8 used electrical lung impedance tomography to assess changes in lung volume.28,29 They showed that HFNC was associated with an increase in end-expiratory lung volume and confirmed the generation of positive oropharyngeal pressure reported in earlier studies. Moreover, they reported a significant correlation between end-expiratory lung impedance and airway pressure and demonstrated that at least part of the improvement in oxygenation in subjects with acute hypoxemic respiratory failure was due to alveolar recruitment.8
It is important to discuss the greater improvement in PaO2/FIO2 with CPAP (5 cm H2O) compared with HFNC. In patients with acute hypoxemic respiratory failure, CPAP increases functional residual capacity and displaces ventilation up from the lower flat portion of the respiratory system pressure-volume curve into a more linear portion. Through this well-known mechanism, CPAP improves oxygenation.30–32 Although studies have demonstrated that HFNC is associated with generation of significant positive expiratory pressure,6–8 PAP is widely influenced by numerous factors. The benefits of PAP are likely to be greatest in those patients using high flows and breathing with the mouth closed. However, in our study, we used the highest possible flow, and all our subjects breathed with the mouth closed. In addition, the generated expiratory pharyngeal pressure is significantly different between sexes, with males tending to have lower PAPs than females. Two possible explanations for this discrepancy exist: PAP is influenced first by nasopharyngeal size and second by leaks from the nose.6 In our physiologic study, the majority of our subjects (10/12) were men. So, HFNC probably generates a low PAP, but it is highly dependent upon numerous factors: flow, gender, leaks from the nose, and whether the mouth is open or closed.9
Breathing Frequency
In our study, HFNC was associated with a decrease in frequency. A previous review found variations in frequency response to HFNC33: in most studies, mean frequency decreased. There are probably several competing explanations: a decrease in work of breathing and improvement in oxygenation.
Comfort
Comfort scores were not significantly different under the 3 oxygen therapy conditions. The short duration of sessions in our study may explain the lack of differences in comfort, as longer durations are needed for the emergence of adverse experiences such as upper airway dryness caused by the high-FIO2 face mask,26 intolerance to CPAP,19 or noise with HFNC.34 However, contrary to this result, 75% of our subjects found that HFNC was more pleasant than the other oxygen delivery techniques (CPAP and high-FIO2, non-rebreathing face mask). In clinical practice, Sztrymf et al15,16 reported a remarkable tolerance of HFNC over longer use. This excellent tolerance, systematically reported with HFNC during acute hypoxemic failure,4,15,16 is attributable, at least in part, to the heat and humidity supplied by the device.35 We reported a case of prolonged HFNC use for over 30 d.36
Dyspnea Score
All studies performed in subjects with acute hypoxemic respiratory failure showed significant improvement in clinical parameters with HFNC compared with standard face mask oxygen therapy.4,15,16 However, in our study, even though HFNC distinctly improved dyspnea, the improvement was not statistically significant. Two hypotheses exist: first, although none of our subjects had delirium, the visual analog scale used in our study was subjective, and second, the study may have been underpowered.
Limitations of This Study
This study was designed to determine the physiologic short-term effects of HFNC and did not seek to assess their impact on outcome. However, the findings provide a convincing physiologic explanation to the results of some clinical trials. Neither the subjects nor the investigators were blinded to the oxygen delivery devices. This may have biased the results, although this was minimized by the fact that study periods were performed in a random order. Only one type of HFNC device was used in this study. Nonetheless, the results regarding subject effort or PaO2/FIO2 would probably be similar with other HFNC devices. We used the largest cannula tolerable for each individual; however, we were not able to quantify leaks around the nose. The PAP generated by HFNC appears to be flow-dependent, so we used the highest possible flow (60 L/min). However, we cannot assert that the results (in terms of inspiratory effort or oxygenation) would be similar with a different setting. We did not record the flow signal or gastric pressure. This is another limitation of our study in the assessment of inspiratory effort.
Conclusions
In summary, the results of this provide new physiologic guidance for selecting oxygen therapy devices in patients with acute hypoxemic respiratory failure. The findings are of clinical relevance because they show that, in such subjects, HFNC provided a better physiologic response in terms of muscle unloading and oxygenation than conventional oxygen given through a high-FIO2, non-rebreathing face mask. However, in our study, oxygenation improvement was better, with a CPAP of 5 cm H2O. HFNC could be an alternative to conventional oxygen therapy in patients with acute respiratory failure, but further studies are needed to specify the place of HFNC in the strategy of treatment for these patients.
Acknowledgments
We are grateful to the junior doctors, nursing staff, and our clinical research associate Marie-Pierre Baudier. We thank Patrick McSweeny for stylistic editing of the manuscript.
Footnotes
- Correspondence: Frederic Vargas MD PhD, Service de Réanimation Médicale, Centre Hospitalo-Universitaire Pellegrin-Tripode, Place Amélie Raba Léon, 33076 Bordeaux Cedex, France. E-mail: frederic.vargas{at}chu-bordeaux.fr.
This study was supported by a research grant from Fisher & Paykel Healthcare. The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1522
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}