

Abstract
INTRODUCTION: Recent advances in technology and protocols have made the use of extracorporeal membrane oxygenation (ECMO) a viable rescue therapy for patients with ARDS who present with refractory hypoxemia. Despite the lack of strong evidence supporting the use of ECMO in ARDS, its use seems to be increasing. We sought to determine recent trends in the use of ECMO for ARDS. We also assessed trends in mortality among patients with ARDS in whom ECMO was used.
METHODS: We performed a retrospective analysis using the largest all-payer in-patient healthcare database in the United States, the Healthcare Cost and Utilization project, the National In-patient Sample database from 2008 to 2012. Subjects with ARDS were identified using carefully chosen International Classification of Diseases, Ninth Revision codes.
RESULTS: We found that in 2008, about 1 in 1,000 subjects with ARDS underwent ECMO. Over the subsequent 4-y time period, there was a 0.19% absolute increase and 70% relative increase in the use of ECMO for ARDS. The mortality rate among subjects with ARDS in whom ECMO was used declined from 78% in 2008 to 64% in 2012. We also found a trend toward a reduction in hospital stay among survivors.
CONCLUSION: In the United States, between 2008 and 2012, there was an increasing trend toward the use of ECMO in patients with ARDS that coincided with a slight increase in survival among these patients.
Introduction
ARDS affects up to 200,000 patients in the United States each year and is a major cause for morbidity and mortality. When Ashbaugh and colleagues first described the syndrome in 1967, the mortality was about 65%.1,2 Subsequent observational studies have shown a continued trend toward decreasing mortality from ARDS with current estimates at about 30−40% with severe forms of ARDS having higher mortality rates compared with mild or moderate forms of ARDS.3,4 Factors associated with the observed decline in ARDS-related mortality include early recognition, advances in treatment of sepsis and other associated critical illnesses, lung-protective ventilatory strategies, use of neuromuscular blockade, and prone positioning.5,6,7 A mortality rate of 30−40% for ARDS is still unacceptably high. Therefore, researchers and clinicians continue to seek additional therapies that could potentially improve outcomes of ARDS. A subset of patients with severe ARDS present with refractory hypoxemia that is not resolved with strategies like lung recruitment maneuvers, prone positioning, neuromuscular blockade or rescue therapies like inhaled nitric oxide or high-frequency oscillatory ventilation.2,8–11 In these patients, extracorporeal membrane oxygenation (ECMO) is an attractive option. The conventional ventilatory support versus ECMO for severe adult respiratory failure (CESAR) trial showed increased 6-month disability-free survival in subjects who received ECMO.12,13 Interest in the use of ECMO for ARDS goes back to the 1970s, and earlier studies showed no survival benefit.14,15,16 However, in the past decade, substantial improvements have been made in the technology and protocols for ECMO, and thus interest has renewed in this therapeutic option for patients with severe ARDS and refractory hypoxemia. In 2009, the CESAR trial 15 showed that subjects transferred to a center with an ECMO-based management protocol had a survival benefit compared with those who received conventional management without referral. We used a large national database of in-patients in the United States to examine the recent trends in the use of ECMO for ARDS during the period from 2008 to 2012. We also examined demographics and mortality trends among subjects with ARDS who underwent ECMO during that period.
QUICK LOOK
Current knowledge
ARDS continues to have high morbidity and mortality. Survival in patients with ARDS may be improving, however, Extracorporeal membrane oxygenation (ECMO) can be utilized in patients with severe forms of ARDS. There is a paucity of data regarding extracorporeal support measures in ARDS.
What this paper contributes to our knowledge
The rates of diagnosis of ARDS are increasing as reported by national in-patient sampling data. The survival rates of subjects with ARDS improved during the study period of 2008 to 2012. There was an increase in the utilization of ECMO from 2008 to 2012 with an improvement in the survival of subjects requiring it. The length of stay in subjects requiring ECMO decreased. As the number of subjects receiving ECMO increased, there seemed to be no difference in the sex or ethnic distribution.
Methods
Patient Population
Institutional review board exemption was obtained for this study. We performed a retrospective analysis using the largest all-payer in-patient healthcare database in the United States, the Healthcare Cost and Utilization project - National In-patient Sample database (HCUP-NIS).17 Unweighted, it includes data from approximately 8 million hospital stays per year, representing a sample of 20% of the hospitals in the United States. Weighted (when expanded to estimate nationwide discharges), it estimates data corresponding to about 40 million annual hospitalizations. To identify patients with ARDS, we examined all patients in the database from 2008 to 2012 with the following International Classification of Diseases, Ninth Revision (ICD-9) codes 518.82, 518.51, 518.52, 518.53, 518.81, 518.84, 518.7, 518.4, 861.20, 785.52, 995.92 and ICD-9 Procedure Codes 96.70, 96.71, and 96.72.17,18 Patients who underwent ECMO therapy were identified by the ICD-9 procedure code 39.65. (Table 1).
ICD–9 and CPT Codes Used for Identifying Subjects
Subject Characteristics
Age, sex, race, income quartile for the subjects' zip code, hospital discharge status, and hospital stay for survivors were extracted from the NIS database. The NIS provides 6 categories for race/ethnicity, as follows: “White,” “Black,” “Hispanic,” “Asian/Pacific Islander,” “Native American,” and “other.” The median income quartile for the subjects' zip code was used as a surrogate for socioeconomic status (SES). The HCUP-NIS database defines SES based on the following quartiles of median income for the subjects' zip code: quartile 1, $1−$38,999; quartile 2, $39,000−$47,999; quartile 3, $48,000−$62,999; and quartile, 4 ≥$63,000.
Statistical Analyses
Continuous variables were reported as means and standard deviations and categorical variables as percentages. Using χ2 tests for trend testing, we examined the trends in ARDS diagnosis, mortality from ARDS, the use of ECMO for ARDS, and in-hospital mortality among subjects with ARDS who underwent ECMO. Among subjects with ARDS in whom ECMO was used, we examined the trends in hospital stay. Next, we assessed the differences in use of ECMO for ARDS by sex, age, race, and SES. Univariate analyses were performed using Mann-Whitney U tests and χ2 tests. Analyses were conducted using STATA/IC 13.1 (StataCorp; Texas, USA).
Results
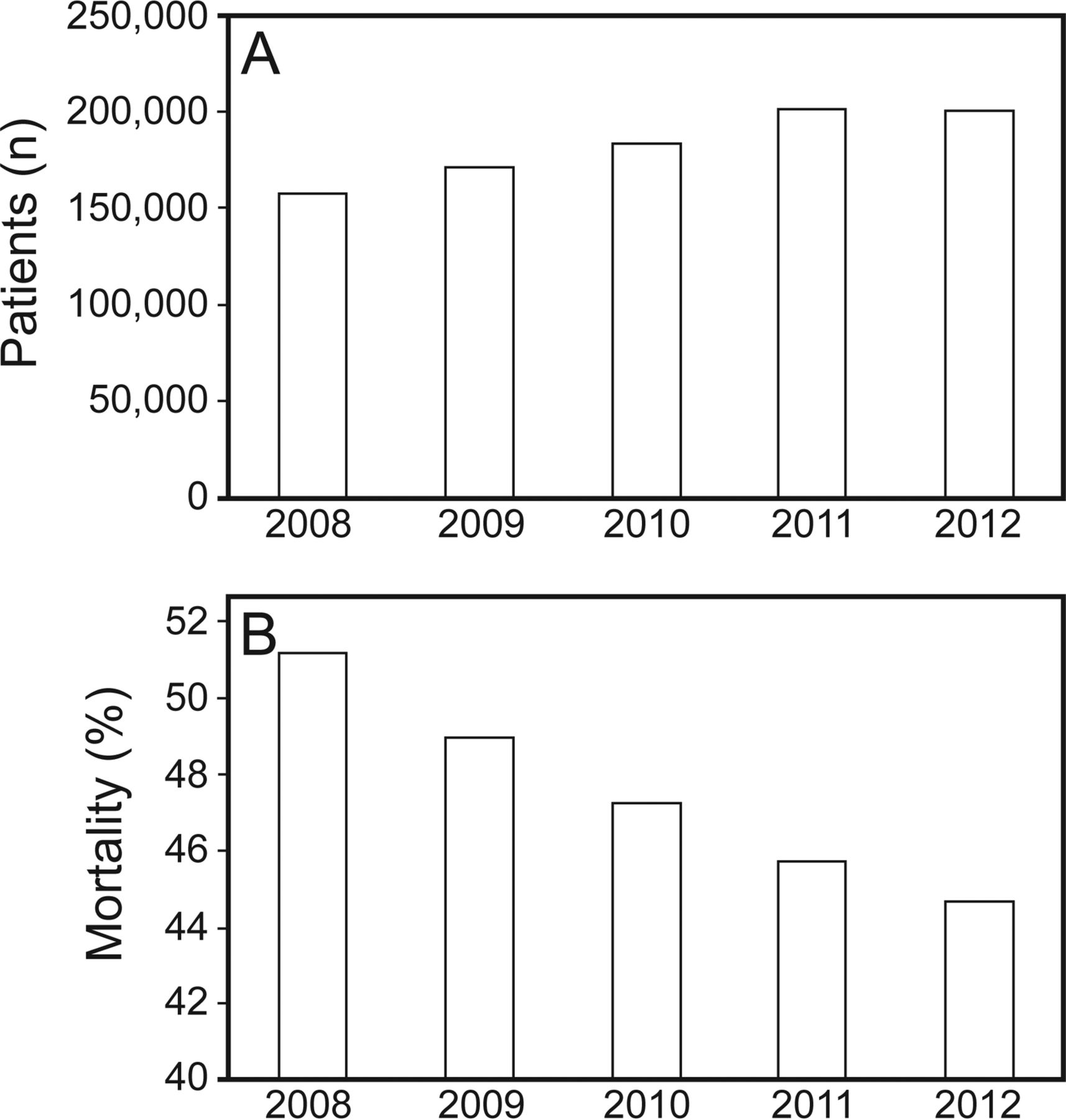
We identified a total of 914,912 subjects who fit our definition of ARDS during the period from 2008 to 2012. Table 2 represents the characteristics of these subjects. In 2008, mortality from ARDS was 51%, and over the next 4 y there was an absolute mortality reduction of 6.5% and a relative reduction of 12.7% (Figure 1, Panel B).
Characteristics of Subjects With ARDS
Overall ARDS prevalence and mortality.
Trends in Use of ECMO for ARDS
In 2008, only about 1 in 1,000 subjects with ARDS underwent ECMO. During the period from 2008 to 2012, there was a 0.19% absolute increase and a 70% relative increase in the use of ECMO as rescue therapy for ARDS. The greatest increase in use of ECMO for ARDS occurred from 2008 to 2009 (0.09% to 0.2%), a 62% relative increase (Table 3).
ECMO Utilization, Mortality and Length of Stay Data
Mortality Trends
In 2008, the mortality rate among subjects with ARDS in whom ECMO was used was 78%. During the 5-y period from 2008 to 2012, there was a 14% absolute reduction and a 19% relative reduction in mortality. There was a sharp decrease in mortality from 2008 to 2010 (78% to 64%). The mortality rate remained stable after 2010 (Table 3).
Hospital Stay
For subjects with ARDS in whom ECMO was used, the mean hospital stay among survivors decreased from 65 d in 2009 to 41 d in 2012. Among nonsurvivors, hospital stay remained relatively stable at between 19 to 23 d.
Use of ECMO for ARDS by Age, Sex, Race, and Socioeconomic Status
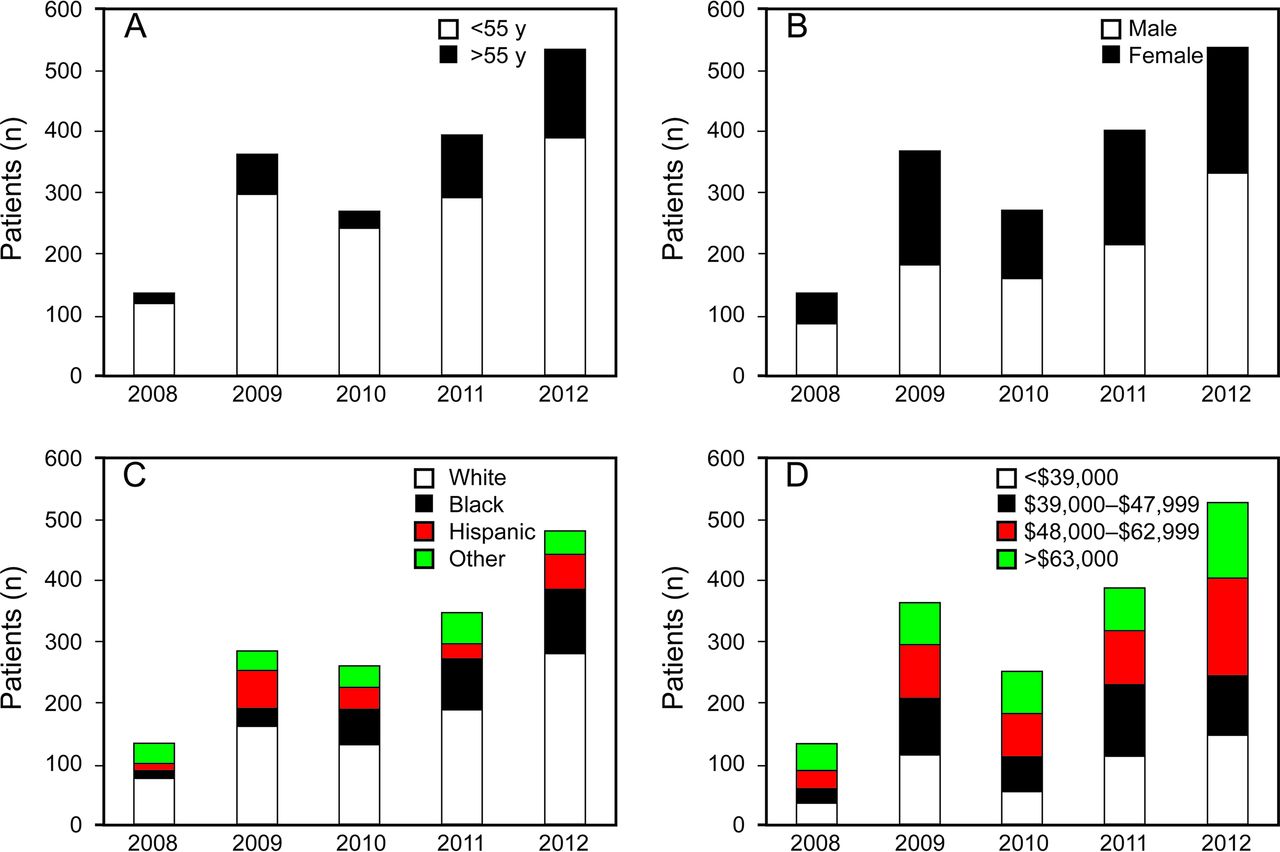
Overall, subjects with ARDS younger than 55 y of age were more likely to be treated using ECMO in the context of ARDS than older subjects were (1,349/242,518 vs 353/656,566) (P < .001). There were no differences in ECMO utilization by sex (male 973/487,905 vs female 731/427,135) or by race (White 827/532,543 vs Black 300/140,569, vs Hispanic 188/86,321). Similarly, there were no differences in the proportion of subjects with ARDS treated with ECMO by socioeconomic status (first quartile 456/272,035 vs second quartile 383/218,128 vs third quartile 436/155,705 vs fourth quartile 374/185,270). Figure 2 depicts yearly totals of use of ECMO for ARDS by age group, sex, race, and socioeconomic status.
ECMO Utilization based on age, gender, ethnicity and socioeconomic status.
Discussion
Main Findings
In this study, we used the largest all-payer in-patient healthcare database in the United States and showed a trend toward increasing use of ECMO for subjects with ARDS from 2008 to 2012. We also found that among patients with ARDS in whom ECMO was used, there was a trend toward decreasing hospital mortality. The hospital stay among survivors decreased during the same period. We did not find any differences in the use of ECMO for ARDS by sex, race, or socioeconomic status.
Strengths and Limitations of This Study
There are several notable limitations to our analysis. First, we inferred the diagnosis of ARDS based on a combination of ICD-9 codes obtained from a nationwide database that reports diagnoses and procedures for in-patient discharges. Therefore, it is possible that we misclassified some subjects with this method of defining ARDS. However, in such types of large-scale claims data, use of ICD-9 codes for case identification is common. Others have used the HCUP-NIS database and similar claims databases to identify patients with ARDS.18,19 The use of ICD-9 procedure codes to identify patients who underwent ECMO is less problematic. However, we could still misclassify subjects who underwent ECMO for reasons other than ARDS. An alternative approach would be to use a prospective database, such as the Extracorporeal Life Support Organization (ELSO) database, to identify patients with ARDS who underwent ECMO.20,21 However, the ELSO database contains data from 160 United States and 120 international centers that voluntarily supply information and therefore may not be a true representation of yearly national trends in ECMO use for ARDS. A nationwide United States-based database like HCUP-NIS, albeit imperfect, gives a good approximation of national trends. Another drawback of using such a database is that severity of illness and the clinical circumstances of patients placed on ECMO cannot be ascertained. A point of novelty for our analysis is the exploration for possible differences in use of ECMO for ARDS by age, race, sex, or socioeconomic status.
Interpretation of Findings in Relation to Previously Published Work
The yearly total numbers of ECMO use in ARDS from our analysis were similar to those observed in the ELSO database, as reported by Schmidt and colleagues21,22 indicating that our algorithm for identifying cases of ECMO in ARDS from the HCUP-NIS database probably performed well. In the ELSO database, the number of ECMO procedures for acute respiratory failure per year was stable at about 100 per year from 2000 to 2008.22 In 2009, there was a marked increase to about 350 per year. We observed the same uptick between 2008 and 2009. A likely reason for this sharp increase in use of ECMO for ARDS from 2008 to 2009 was the 2009 H1N1 influenza pandemic. Numerous reports are available that describe experiences of ECMO use for H1N1-associated ARDS.23,24 There are many possible reasons for the continuous increase in use of ECMO for ARDS since 2009. First, many intensive care units developed expertise in the use of ECMO for ARDS following the experience from the 2009 H1N1 influenza pandemic. Second, improvements have been made in technology and in protocols for the use of ECMO in patients with ARDS. Additionally, strategies for patient selection have improved in recent years23–26 Even though the use of ECMO for management of ARDS increased from 2008 to 2012; it is used in fewer than 3 per 1,000 cases of ARDS. If recent trends are an indication, then the use of ECMO for ARDS is expected to continue to rise in the coming years, despite the limited data regarding its efficacy and effectiveness.26,27 It is notable that there is a large multicenter phase-3 trial underway to study the efficacy (60-d mortality) of ECMO in early ARDS versus conventional therapy.28
Our findings are also in agreement with those of Schmidt et al22 who showed that the trend in mortality among subjects with ARDS who underwent ECMO decreased slightly between 2008 and 2012. According to their analysis of the ELSO database, the survival rate among subjects with ARDS who underwent ECMO therapy was about 50% in 2008 and improved to about 60% in 2009, followed by a plateau. It is unclear whether this decrease in mortality is due to ECMO therapy or is part of the overall trend of declining ARDS mortality, or both. Alternatively, such a reduction in mortality may be due to administration of ECMO to patients with less severe ARDS who would have a low expected mortality. Ideally, a severity-adjusted analysis may need to be performed to determine the relative contribution of each factor to the observed trend in decreasing mortality.
Implications for Future Research, Policy, and Practice
The increasing use of ECMO for ARDS brings attention to the need for more evidence of efficacy and effectiveness of this treatment modality that is quite expensive and resource intensive. Ongoing prospective randomized control trials will provide evidence of efficacy, and detailed economic analyses of prospective databases like the ELSO database will give insight into the effectiveness of ECMO for ARDS. These findings also bring attention to the subject of training of current and future critical care physicians in the use of this modality. As more surgical and nonsurgical specialists adopt ECMO for ARDS, rigorous training of physicians along with nursing staff, perfusionists, pharmacists, and other support staff is paramount. With limited resources and staff, innovative multidisciplinary training will need to be developed. Some institutions now offer fellowship training in extracorporeal life support and others have developed local educational programs to train medical care teams.
Conclusions
We report that in 2009, a sharp increase occurred in the use of ECMO for ARDS and since then, there has been a steady increase. This coincided with a slight increase in survival among subjects with ARDS in whom ECMO was used during the same period. Despite the absence of compelling evidence for its efficacy and effectiveness in ARDS, ECMO is emerging as an important tool for management of severe ARDS with refractory hypoxemia.
Footnotes
- Correspondence: Bhupinder Natt MD, University of Arizona Health Sciences, Division of Pulmonary, Allergy, Critical Care and Sleep, 1501 North Campbell Ave, Tucson, AZ 85724. E-mail: bnatt{at}deptofmed.arizona.edu.
See the Related Editorial on Page 1425
- Copyright © 2016 by Daedalus Enterprises





{kind=link}
{kind=link}