

Abstract
BACKGROUND: Recommendations regarding ventilation during cardiopulmonary resuscitation (CPR) are based on a low level of scientific evidence. We hypothesized that practices about ventilation during CPR might be heterogeneous and may differ worldwide. To address this question, we surveyed physicians from several countries on their practices during CPR.
METHODS: We used a Web-based opinion survey. Links to the survey were sent by e-mail newsletters and displayed on the Web sites of medical societies involved in CPR practice from December 2013 to March 2014.
RESULTS: 1,328 surveys were opened, and 548 were completed (41%). Responses came from 54 countries, but 64% came from 6 countries. Responders were mostly physicians (89%). From this group, 97% declared following specific CPR guidelines. Regarding practices, 28% declared always or frequently adopting only continuous chest compressions without additional ventilation. With regard to mechanical chest compression devices, 38% responded that such devices were available to them; when used, 28% declared always or frequently experiencing problems with ventilation such as frequent alarms. During bag-mask ventilation in intubated patients, 18% declared stopping chest compression during insufflation, and 39% applied > 10 breaths/min, which conflicts with international CPR guidelines. When a ventilator was used, the volume controlled mode was the most common strategy cited, but there was heterogeneity regarding ventilator settings for PEEP, trigger, FIO2, and breathing frequency. SpO2 and end-tidal CO2 were the 2 most monitored variables cited.
CONCLUSIONS: Physicians indicated heterogeneous practices that often differ significantly from international CPR guidelines. This may reflect the low level of evidence and a lack of detailed recommendations concerning ventilation during CPR.
- ventilation
- cardiac arrest
- cardiopulmonary resuscitation
- mechanical chest compression
- manual chest compression
- chest compression
- survey
- practices
Introduction
The ventilatory strategy used during cardiopulmonary resuscitation (CPR) could influence the chance of survival because it can interfere with chest compressions. Recommendations regarding ventilation during CPR in CPR guidelines are weak and are based on relatively low levels of evidence.1–4
In the past, ventilation was the first action to be adopted during CPR.5,6 All guidelines published between 1974 and 2005 advocated the famous ABC sequence (A, airway; B, breathing and C, circulation) during the rescue of a victim of cardiac arrest (see the supplementary material at http://www.rcjournal.com). The importance of ventilation decreased progressively in these guidelines over time,7 and the international CPR guidelines published in 2010 changed the former ABC sequence to CAB.1–4
Some authors advocate only performing chest compressions during CPR, without ventilation, with the goal to provide better neurological outcomes. This strategy is advocated for the general public. Once at least 2 health care professionals are involved, airway opening and breathing should be performed according to international CPR guidelines.1–4 Physiological interactions between ventilation and circulation may also differ when chest compression is done manually or with automated devices.
Due to a lack of sufficient evidence in the literature, clinicians are often left with doubts about how ventilation should be performed.9–11 Heterogeneity of ventilation practices during CPR is therefore likely to occur. Because ventilation practices may affect outcomes, we conducted an international survey to assess opinions regarding the practices specifically related to ventilation during CPR in adult victims of a non-traumatic cardiac arrest.
QUICK LOOK
Current knowledge
Assisted ventilation is an important aspect of cardiopulmonary resuscitation (CPR) because it can directly influence survival through positive or negative interactions with chest compression. International guidelines, however, are supported by a low level of evidence and practice heterogeneity is expected.
What this paper contributes to our knowledge
This survey showed that practices regarding the combination of assisted ventilation with chest compressions during CPR were heterogeneous and often differed significantly from CPR guidelines. Difficulties related to ventilation were reported to be high.
Methods
Instrument
We used a mixed-methods approach to develop our questionnaire, taking into account the current international CPR guidelines.1–4 The first version of our questionnaire was created after discussion among 3 critical care physicians working in Europe, 1 physician in Brazil, and 2 emergency department physicians in Switzerland. We intentionally sampled participants to represent different practice settings. We developed a draft questionnaire, which we piloted among a focus group of 5 physicians from different regions in France with experience in CPR. A subsequent draft questionnaire underwent a review process by 20 physicians who participated in the acute respiratory failure meeting group or the trauma and emergency medicine meeting group during the 2013 European Society of Intensive Care Medicine Congress in Paris, France. The final version (see the supplementary material at http://www.rcjournal) was hosted on a Web platform (http://www.cardiomobile.ch), and several physicians from different regions in France tested it.
Survey responses were closed, and response options varied, including multiple choice, single choice on a 4-point response scale (never, rarely, frequently, or always), and Yes/No answers. Some questions were only available depending on specific answers related to accessibility or practices.
This survey was voluntary and anonymous, and additional consent was not required according to Swiss regulatory rules.
Subjects
Professionals involved in resuscitation teams, including physicians, nurses, respiratory therapists, and paramedics, were considered as potential responders about the way they manage ventilation and chest compression in adult victims of a non-traumatic cardiac arrest.
Survey Administration
An invitation was sent to members of different national or European societies involved in CPR, and a link to the self-administered survey was available on the Web sites of these societies. The survey could be completed from December 2013 to March 2014. A reminder invitation was sent twice during this period.
Analysis
Only fully completed surveys were analyzed. We elected a priori to include only those respondents who reported being clinically active in performing CPR.
Results
Survey Participation
Of the 1,328 surveys opened, 548 (41%) were completed. Responses came from 54 countries, but most answers (64%) came from 6 countries: France (25%), Japan (14%), Brazil (11%), Belgium (9%), and Canada (5%).
Respondents
The great majority of responders were physicians (490 of 548 respondents, 89%), while nurses (40, 7%), paramedics (11, 2%), and respiratory/physical therapists (7, 1%) represented a small proportion coming from only 3 countries. We thus decided to analyze only physicians' responses (n = 490) for more consistency and representativeness.
In this group, 55% (270 of 490 physician respondents) worked in a university hospital, 35% (170 respondents) declared having a clinical activity in the pre-hospital emergency field, and 54% (265 respondents) said they had some activity in the ICU setting.
Equipment Available for Ventilation and Chest Compression
Almost all physicians (479 of 490 respondents, 98%) affirmed having a bag-mask, which was cited to be the only device available by 19% (94 respondents); 74% (363 respondents) declared having a ventilator, and 7% (33 respondents) said they had a Boussignac CPR tube (Vygon, Ecouen, France) available for CPR.
Concerning chest compression, 38% (186 of 490 respondents) declared having a specific external pump mechanical device; 24% (116 respondents) declared having a piston chest compression (LUCAS-CPR, Physio Control, Lund, Sweden; or Thumper Mechanical CPR device, Michigan Instruments, Michigan); 12% (61 respodents) had an automated load-distributing band (AutoPulse, Zoll, Chelmsford), and 2% (9 respondents) answered that they had a manual mechanical chest compression device available (AMBU CardioPump, AMBU Company, Copenhagen, Denmark). Finally, 7% (32 respondents) said they had > 1 mechanical device available for chest compression. A total of 211 physicians (43%) declared belonging to a center engaged in non-heart-beating organ donation. In this subgroup, the availability of an automatic mechanical chest compression device was higher (97 respondents, 44%) as well as the probability to use it, according to 60% (58 respondents) who preferred using mechanical chest compression device over manual chest compression.
Practices and Organization
General.
Almost all physicians (475 of 490 respondents, 97%) declared following specific CPR guidelines; 73% (11 of 15 respondents) of those who did not follow a CPR guideline belonged to a non-university hospital. The European Resuscitation Council guidelines were the most cited (232 of 475 respondents, 49%), followed by the American Heart Association guidelines (38%) and national guidelines (11%); hospital-specific protocols were scarcely cited (2%).
Basic Life Support.
Among the physicians who completed the survey, 28% (138 of 490 respondents) answered always or frequently adopting the strategy of only continuous chest compression without any additional form of ventilation, especially at the beginning of resuscitation when the rescuer is alone.
For non-intubated patients, when CPR was performed with an automated chest compression device (LUCAS/AutoPulse), 68% (103 of 152 respondents) declared always or frequently applying the 30:2 option to ventilate the patient with a bag-mask device; when a supraglottic airway was inserted (eg, laryngeal mask airway), only 36% of the physicians (55 of 152 respondents) answered always or frequently applying the 30:2 option to ventilate the patient.
During Intubation Procedure.
During the intubation procedure, 46% of all respondents (225 of 490 respondents) and 43% of physicians (65 of 152 physician respondents) who declared having an automated mechanical chest compression device available confirmed stopping manual or mechanical chest compression, respectively.
Advanced Life Support.
In patients already intubated, 68% of the physicians (326 of 479 respondents) declared never stopping manual chest compression for bag-mask insufflation. Of these 326 respondents, 48% (158) declared adopting a frequency of 8–10 insufflations/min, 5% (16) declared using a frequency < 8 insufflations/min, 37% (121) declared using a frequency > 10 insufflations/min; of the 121 who used a frequency > 10 insufflations/min, 20% (24) used a frequency ≥ 16 insufflations/min.
During manual chest compression in patients already intubated, 87% (428 of 490 respondents) and 46% (223 of 490 respondents) declared always or frequently using a bag-mask and a ventilator, respectively. Continuous flow insufflation with the Boussignac tube specific to CPR was cited by only 4% (18 of 490 respondents).
Ventilator Settings and Monitoring.
When a ventilator was applied during CPR, the volume controlled mode was the most commonly cited mode (260 of 363 respondents, 72%), followed by pressure controlled mode (85 of 363, 23%), and CPAP (18 of 363, 5%).
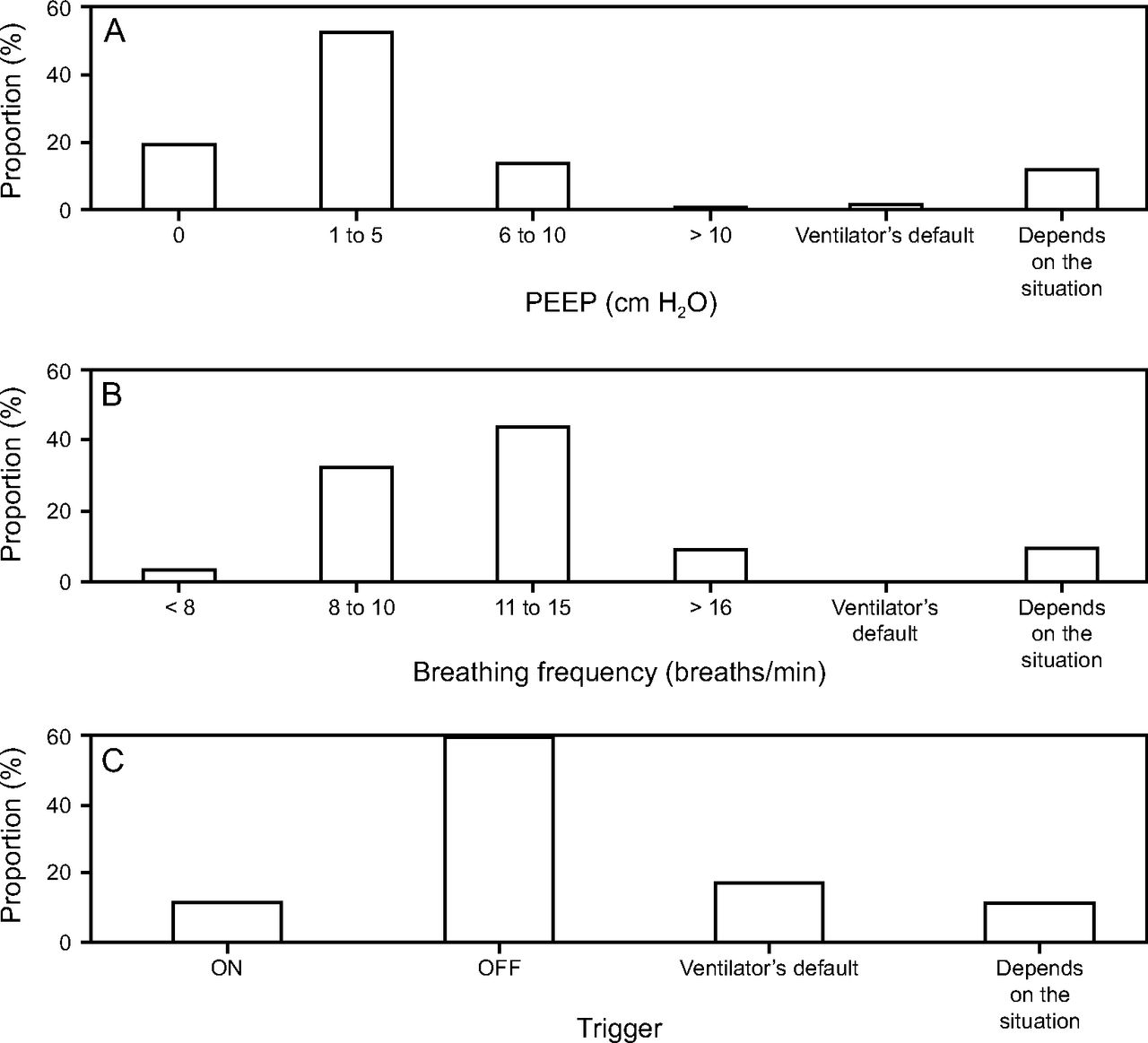
There was a marked heterogeneity regarding the ventilator settings of PEEP values (Fig. 1A), breathing frequency (Fig. 1B), and trigger (Fig. 1C). Among responders who had a ventilator available, 42% (153 of 363 respondents) declared setting FIO2 according to pulse oximetry (SpO2), with heterogeneous SpO2 targets (Fig. 2A). Among those who declared setting FIO2 independently of SpO2, almost all cited an FIO2 of 1.0 (Fig. 2B). Monitoring practices were also heterogeneous, with SpO2 and end-tidal CO2 being the 2 most frequently cited variables (Fig. 3).

Ventilator settings during cardiopulmonary resuscitation.
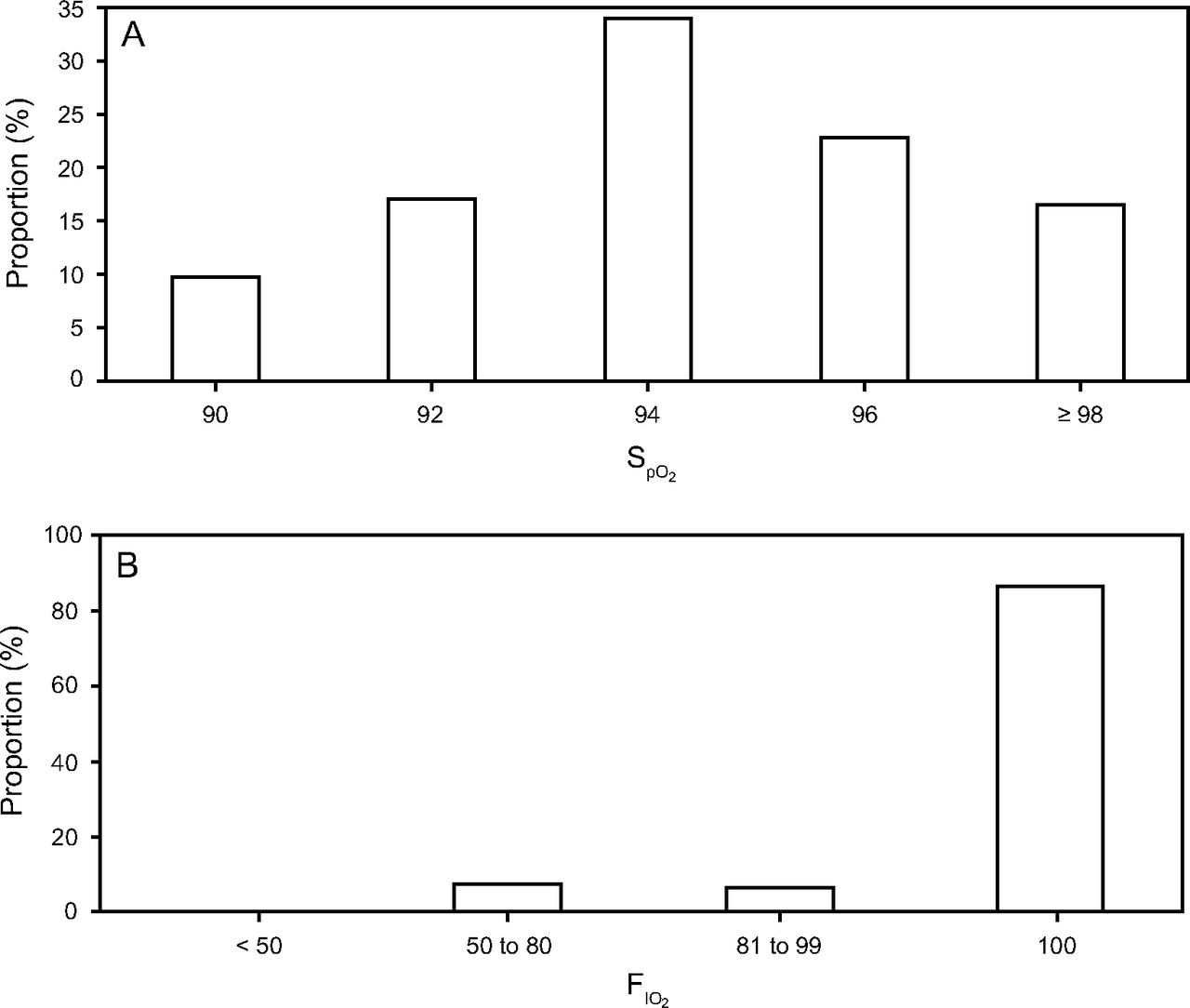
FIO2 during cardiopulmonary resuscitation. (A) According to SpO2 target. (B) Independent of SpO2 value.

Monitoring of ventilation-related variables during cardiopulmonary resuscitation. PETCO2 = end-tidal carbon dioxide pressure.
Specific Settings for Automatic Chest Compression Devices.
During automatic mechanical chest compression in intubated patients, 18% (28 of 152) of the physicians declared always or frequently applying the 30:2 option; 62% (94 of 152) and 57% (86 of 152) of the physicians declared always or frequently using a bag-mask and a ventilator, respectively; 12% (18 of 152) of the participants who had an automatic mechanical chest compression device available changed their ventilation monitoring options when using these devices instead of manual chest compression. In addition, 32% (48 of 152 physicians) cited always or frequently changing their ventilation practice when using an automated chest compression device: 72% (35 of 48) of them declared adjusting ventilator settings, 36% (18 of 48) switched from manual to mechanical ventilation, and 21% (10 of 48) switched from mechanical to manual ventilation (more than one answer was possible).
Finally, only 27% (41 of 152 physicians) declared never experiencing major problems (Fig. 4A) concerning ventilation when automated chest compression devices were used. Different strategies were proposed to face major problems (Fig. 4B).

Ventilation during cardiopulmonary resuscitation done with an automated chest compression device. (A) Major problems experienced. (B) Different strategies proposed to face major problems.
Discussion
This is the first international survey evaluating opinions and declared practices regarding ventilation during CPR. The results suggest a wide heterogeneity in practices exist. Based on the results of our survey, we can distinguish 2 major findings. First, regarding ventilation, there is a gap between declared practices and CPR recommendations in international guidelines. These observations are consistent with results of an observational study analyzing the quality of multiple parameters of CPR12 and showing that practices often do not align with published recommendations. Second, although nearly all of the respondents stated that they follow international guidelines, responses from the physicians who completed the survey were heterogeneous. Both findings could reflect the low level of evidence and the lack of specificity in the recommendations for ventilation during CPR.
Available Equipment for CPR
For ventilation, a bag-mask was the most common device available, while less than half of responders answered having a mechanical device dedicated to chest compression. A systemic review comparing manual and mechanical chest compression concluded that mechanical chest compression was not associated with harm or benefit.13 In situations such as during transportation, in the catheterization laboratory, and as a bridge to more invasive support, mechanical chest compression seems to be an interesting option, as well as when high-quality manual chest compression cannot be delivered.14 We hypothesize that automatic chest compression may render ventilation more difficult and thus interfere with clinical practices; there are few studies regarding the best ventilation strategy associated with mechanical chest compression devices, and our survey showed that the occurrence of ventilation problems is not negligible when this method of chest compression is used.
Ventilation and Chest Compression
Interestingly, more than a quarter of respondents declared adopting only continuous chest compression, highlighting the prioritization of chest compression over assisted ventilation.15–17 Some authors advocate that ventilation is not necessary during the early phase18 or when the rescuer is alone because providing assisted ventilation may decrease the effectiveness of CPR by increasing the time without chest compression.19
Nichol et al20 published a trial in 2015 in which adults receiving CPR were treated with continuous chest compression with asynchronous ventilations delivered at a rate of 10 ventilations/min (intervention group) or with interrupted chest compression for ventilation at a ratio of 30:2, respectively (control group). The rate of survival to hospital discharge and favorable neurologic function at discharge were similar in both groups. Interestingly, the chest-compression fraction, which is an important marker of interruptions of chest compression, were high in both groups (0.77 in intervention group and 0.83 in control group) and above international recommendations. The mechanics driving blood flow during CPR are complex and positive-pressure ventilation may play a key role in promoting better blood flow along with chest compressions if the interaction between ventilation and chest compression is well adjusted.21
We observed that almost half of the providers declared stopping chest compression for endotracheal intubation. The optimal timing of an advanced airway placement is not well defined in the literature. Some studies demonstrated positive results when subjects were intubated22 in the first 13 min,23 while other studies showed better results when endotracheal intubation was avoided24 or delayed in favor of minimally interrupted chest compression.25 Recommendations regarding the relationship between chest compression and ventilation were not strictly followed by almost 20% of the providers, regardless of whether the patient was intubated.
Ventilation Practice
More than 80% of the responders declared having more than one option to support ventilation during CPR, which implies that understanding the different features of each device is important. Despite the various risks in relation to the use of a bag-mask,26,27 this device remains the most widely used to deliver assisted ventilation during CPR. Hyperventilation can be common during CPR. In the porcine CPR model, a higher ventilation rate promotes a lower coronary perfusion pressure and survival rate.28 International guidelines recommend 8–10 breaths/min when the patient is already intubated, but we observed that almost 40% of the rescuers adopted a ventilation rate > 10 breaths/min when using a bag-mask device.
Our results indicated a large heterogeneity in setting ventilator parameters during CPR, possibly reflecting the absence of detailed recommendations in guidelines. Furthermore, a controversy exists regarding the use of positive-pressure ventilation,29,30 which could explain the different PEEP practices observed in this survey. Regarding oxygenation, the current literature is equivocal; some studies have demonstrated that hyperoxemia is associated with higher mortality,31,32 whereas a large retrospective study did not find any relationship.33 In our survey, almost all of the providers established an FIO2 of 1.0 during CPR, and 35% declared adopting SpO2 > 96% when using pulse oximetry as a target. This high oxygenation target may carry specific risks, but further studies are needed to define the appropriate level of oxygenation during CPR.
Monitoring
In this study, the most frequently monitored parameter was SpO2. End-tidal CO2 was the second most cited parameter to be monitored, despite numerous limitations that render its use in routine practice complex.34 Nevertheless, end-tidal CO2 is usually considered as a physiological parameter that correlates with cardiac output and reflects the quality of chest compression during CPR.7,35 The European Resuscitation Council's 2015 guidelines highlighted the importance of end-tidal CO2 but limited its use to specific purposes.36
Manual Versus Automatic Mechanical Chest Compression and Ventilation
Ventilatory and monitoring practices were different when using an automatic mechanical chest compression device in comparison to manual chest compression. When using automatic mechanical chest compression devices, both the bag and a ventilator were frequently used. The occurrence of ventilatory problems with automatic chest compression devices appears to be frequent because most of responders declared experiencing majors issues requiring adjustment of ventilator settings.
Ventilation Practices During CPR
González et al,36 in a survey with questions similar to our survey, tried to describe ventilatory practice during CPR in children. They observed, as in our adult survey, considerable variation in the management of ventilation for children in cardiac arrest, and international recommendations were not being followed in a high percentage of cases. The results of our survey, similar to those by González et al,37 suggest that further studies of the role of ventilation during cardiac arrest are required to better understand and adjust ventilation for patients in cardiac arrest.
Limitations
We received answers from participants working in 54 countries, but 64% came from 6 countries and half of the responders were from 3 countries, which limits the worldwide representation from our survey. This survey documented opinions about practices rather than practices themselves.
The study was performed before the most recent international CPR guidelines published by the American Heart Association38,39 and by the European Resuscitation Council.36,40 As a result, we cannot draw conclusions on the impact of the most recent recommendations, although they were very similar to the guidelines published in 2010 with regard to ventilator practices. The American Heart Association1,2,38,39 and the European Resuscitation Council 3,4,36,40 CPR guidelines are similar regarding aspects of ventilation during CPR.
Conclusions
This international survey showed that opinions and declared practices regarding the management of ventilation with chest compression differ significantly from international recommendations, even though the majority of responders stated that they follow CPR guidelines. The low level of scientific evidence and the lack of specificity in current recommendations regarding ventilation may have led to these findings. The multiplicity of available medical devices dedicated to either automated chest compression or ventilation reported in this survey may also contribute to differences in the interpretation of guidelines.
Acknowledgments
The authors are grateful to the European Society of Intensive Care Medicine, the French Society of Emergency Medicine (Société Française de Médecine d'Urgence), the Brazilian Association of Intensive Care Medicine (Associação Brasileira de Medicina Intensiva), the French Language Society of Intensive Care (Société de Réanimation de Langue Française), the Japanese Society of Intensive Care Medicine, the Belgian Society of Intensive Care Medicine (Société Belge d'Anesthésie et de Réanimation), the European Artificial Ventilation Research Network, the International PanArab Critical Care Medicine Society, the European Resuscitation Council, and the European Critical Care Research Network-European Society of Intensive Care Medicine, who endorsed the survey. It was the survey of the month for the European Society of Intensive Care Medicine in December 2013. We thank Nathalie Rey, Marc Niquille, and Evangelia Akoumianaki for their important contributions to the survey formulation.
Footnotes
- Correspondence: Ricardo Luiz Cordioli MD PhD, Hospital Israelita Albert Einstein, Av Albert Einstein, 627 - Morumbi 05652-900, Sao Paulo, Brazil. E-mail: rlcordioli{at}gmail.com.
Dr Richard has disclosed relationships with Air Liquide Medical Systems, Vygon, Dräger, and Covidien. Dr Brochard has disclosed relationships with Maquet, Covidien, Dräger, Philips Respironics, Air Liquide, and General Electric. Dr Khoury has disclosed a relationship with the European Commission.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}