

Abstract
BACKGROUND: Regular monitoring combined with early and appropriate use of airway clearance can reduce unplanned hospital admissions for patients with neuromuscular disease (NMD) and spinal cord injury (SCI). We aimed to describe and compare knowledge of guidelines, monitoring of cough effectiveness, clinician prescription/provision of airway clearance strategies, and service provision constraints in the United Kingdom and Canada.
METHODS: This was a cross-sectional survey of clinicians affiliated with NMD and SCI clinics in Canada, 2016 attendees at the Home Mechanical Ventilation Conference in the United Kingdom, and United Kingdom physiotherapist networks.
RESULTS: We received 155 surveys (92 from Canada; 63 from the United Kingdom). More UK respondents (76%) were aware of airway clearance guidelines than Canadian (56%) respondents (P = .02). Routine assessment of cough effectiveness was reported by more UK respondents (59%) than Canadian (42%) respondents (P = .044). Cough peak flow (CPF) was the most common method used in both countries, although it was more commonly used in the UK (96%) than in Canada (81%, P = .02). Fewer Canadian respondents reported using CPF before initiation of airway clearance (81% vs 94%, P = .046), and fewer Canadian respondents showed results to patients for technique feedback (76% vs 97%, P = .007). Similar participant numbers reported using CPF after initiation to ensure adequate technique (73% vs 72%, P = .92). Mechanical insufflation-exsufflation (MI-E) + lung volume recruitment (LVR) + manually assisted cough when CPF ≤ 270 L/min was most routinely recommended (41% overall). Monotherapy was infrequent (LVR 15%, manually assisted cough 7%, and MI-E 4%). More Canadians identified constraints on service provision, specifically insufficient public funding for equipment (68% vs 39%, P = .002) and inadequate community workers' knowledge (56% vs 34%, P = .002). Funding for community support was a common constraint in both countries (49% vs 42%).
CONCLUSIONS: The somewhat variable cough effectiveness monitoring and airway clearance practices identified in this survey confirm the need for further work on knowledge translation related to guideline recommendations and the need to address common constraints to optimal service delivery.
Introduction
Decreased cough effectiveness is one of the main causes of respiratory complications such as atelectasis and pneumonia, which can result in increased morbidity, mortality, and economic burden for individuals with neuromuscular disorders (NMDs) or high spinal cord injury (SCI).1–4 Cough is an important host defense mechanism for clearing the airway of secretions, including those containing pathogenic organisms.5 Interventions to augment cough effectiveness and promote secretion clearance include airway-clearance techniques such as lung volume recruitment (LVR) (also termed breath-stacking), manually assisted cough, and mechanically assisted cough using a mechanical insufflation-exsufflation (MI-E) device. The increased lung volumes generated via LVR improve elastic recoil and thereby increase cough peak flow (CPF) and promoting sputum expectoration.5 Manually assisted cough further enhances CPF for patients with weak expiratory muscles such as those with NMD or SCI.6 Mechanical insufflation-exsufflation enhances CPF compared with manual techniques.7
Monitoring and improvement of cough effectiveness are important goals in both ongoing management of NMD and SCI rehabilitation.8 For individuals experiencing progressive NMD, regular assessment of pulmonary function including CPF is important for the detection of deterioration of cough effectiveness and the need for airway-clearance interventions.9 Failure to monitor cough effectiveness and implement airway-clearance interventions results in increased emergency department visits, hospital admissions, need for invasive mechanical ventilation, and decreased survival as a result of premature death.10,11 Professional society guidelines from both Canada and the United Kingdom make recommendations related to airway clearance.11–14 However, some data suggest that the use of airway clearance interventions is variable, with anecdotal evidence indicating use is not always based on systematic CPF monitoring.15
Our overall goal was to understand the adoption of guideline recommendations related to monitoring of cough effectiveness and utilization of airway-clearance strategies in Canada and the United Kingdom. These results would inform the need for knowledge-translation strategies. Therefore, we sought to describe and make comparisons of care provider awareness of guideline recommendations and current practice related to monitoring cough effectiveness, and of clinician prescription and recommendation of airway clearance strategies between care providers in the United Kingdom and those in Canada. Secondary objectives were to identify current education for patients and families related to use of airway-clearance techniques, and to understand existing constraints to service provision barriers, particularly in terms of guideline recommendations.
QUICK LOOK
Current knowledge
Decreased cough effectiveness causes respiratory complications for individuals with neuromuscular disorders and those with high spinal cord injury. Airway clearance techniques including lung volume recruitment, manually assisted cough, and mechanical insufflation-exsufflation devices augment cough effectiveness and promote secretion clearance. Therefore, monitoring and improvement of cough effectiveness are important goals in both ongoing management of neuromuscular disorders and spinal cord injury rehabilitation. Professional society guidelines from both Canada and the United Kingdom make recommendations related to airway clearance.
What this paper contributes to our knowledge
Knowledge of guideline recommendations was moderate and adoption of practice recommendations related to cough effectiveness monitoring and airway clearance was variable in our survey, indicating the need for further knowledge translation work. Cough peak flow and qualitative assessment were the most common methods of determining cough effectiveness in both countries, yet routine assessment was not consistently practiced. Most commonly, multiple airway clearance strategies were used in combination. Constraints to optimal service delivery were frequent in both countries, with insufficient public funding of equipment and ability to provide support in the community being the most common constraints.
Methods
Study Design and Sample
We conducted a cross-sectional survey of respiratory therapists, physiotherapists, respiratory medical specialists, nurses, physiatrists, and neurologists working with clinics participating in the Canadian Neuromuscular Disease Registry and the Rick Hansen Spinal Cord Injury Registry, members of the Canadian Neuromuscular Disease Network from November 2016 to February 2017, and 119 delegates of the Home Mechanical Ventilation United Kingdom meeting in June 2016, as well as United Kingdom physiotherapist networks including the Specialists in Long-term Ventilation at Home network. The Canadian Neuromuscular Disease Registry and the Rick Hansen Spinal Cord Injury Registry are pan-Canadian registries with sites located at 23 NMD clinics and 31 acute care and rehabilitation facilities treating SCI patients. The Canadian Neuromuscular Disease Network is a national network of > 170 researchers, clinicians, and educators working with patients with NMD.
Survey Development
Our interprofessional investigator team included clinicians and researchers from medicine, nursing, respiratory therapy, and physiotherapy with expertise in airway clearance techniques, NMD, and SCI. The team iteratively generated survey items under the domains of provider knowledge, current practice, patient/family education, and constraints to service provision. We iteratively reduced items based on face and content validity to enable the production of a concise survey without removing domains or questions deemed important to the survey objectives. We obtained relevant Research Ethics Board approvals for the study. Return of survey was considered indicative of informed consent.
Survey Pre-testing
Eleven experts in airway-clearance techniques, home ventilation, and survey methodology reviewed the survey and rated the instrument's clarity, content validity, and comprehensiveness.16 Experts were asked to comment on the relevance of each item, omission of important questions, ease of understanding, and presence of inappropriate or redundant items. The survey instrument was refined and then re-evaluated by the expert panel until no further issues were identified.
Survey Pilot Testing
The survey instrument was tested with 5 international experts not involved in the instrument develop phases as a pilot. These testers provided comments on the overall face and content validity as well as completion time.
Survey Administration
Prior to the survey, administrators of the various networks and membership lists of our sample frame sent an advance notice to foster engagement. Due to privacy laws around membership lists, these same administrators then sent the survey via email containing a link to the online survey hosted on SurveyMonkey. We provided slightly modified versions of the survey for participants known to be working with SCI patients and for United Kingdom participants (see the supplementary materials at http://www.rcjournal.com). Participants were encouraged to forward the link to eligible colleagues. To maximize the response rate, email reminders were sent at 2 weeks and at 1 month after the initial invitation. At the beginning of the survey, respondents were asked to confirm their eligibility, defined as participation in a practice that includes monitoring and management of patients with NMD at risk of respiratory failure or individuals with NMD or SCI currently requiring noninvasive or invasive ventilation in the home.
Data Analysis
We used descriptive statistics, including mean ± SD or median and interquartile range, depending on data distribution for continuous variables and frequencies or proportions for categorical variables. We compared categorical responses between United Kingdom and Canadian respondents using chi-square tests. We carried out analyses using SAS 9.3 (SAS Institute, Cary, North Carolina). All analyses were 2-tailed, with P ≤ .05 considered statistically significant.
Results
Participants and Service Volume
We received 155 surveys, with 92 from Canada and 63 from the United Kingdom. Due to an unknown denominator because of our multiple and snowballing survey distribution, we were unable to calculate an overall survey response rate. Canadian respondents comprised 30 (34%) respiratory therapists, 24 (27%) physiotherapists, 9 (10%) nurses, 14 (16%) respiratory medical specialists, 6 (7%) neurologists, and 6 (7%) other (4 physiatrists, 1 intensivist, 1 pediatrician). United Kingdom respondents comprised 31 (49%) respiratory physiotherapists, 18 (29%) nurses, 10 (16%) respiratory medical specialists, and 4 (6%) other (2 intensivists, 1 occupational therapist, and 1 respiratory physiologist). Most Canadian (n = 50, 54%) respondents had > 10 y of experience working with the patient population of interest, whereas most respondents from the UK (n = 44, 70%) respondents had > 5 y of experience. In both countries, respondents represented most regions (Table 1).
Regional Representation
There was variation in both Canada and the United Kingdom in terms of clinic or program size represented by the respondents, the number of patients commenced on MI-E, and the number commenced on noninvasive ventilation on an annual basis (Table 2).
Reported Service Volume
Knowledge of Guidelines
More respondents from the UK (76%) than from Canada (56%) were aware of any published guidelines with recommendations for monitoring cough effectiveness and commencement of airway clearance interventions (P = .02). Of the UK participants aware of guidelines, 98% identified that CPF was recommended for monitoring cough effectiveness, whereas 90% of Canadian participants aware of guidelines identified CPF as the test recommended.
Current Practice
More UK respondents (59%) than Canadian respondents (42%) (P = .044) reported routine assessment of cough strength adequacy as their current practice. The most frequent method to assess cough effectiveness in both countries was CPF, though this was used more commonly in the UK (96%) than in Canada (81%, P = .02). Other common methods (UK vs Canada) were qualitative assessment of cough effectiveness (44% vs 44%) and maximum inspiratory pressure/maximum expiratory pressure (31% vs 44%) with no between-country differences for use of these 2 methods (Table 3).
Methods Used to Assess Cough Effectiveness
More respondents from the UK (94%) than Canadian respondents (81%) reported measuring CPF before initiation of airway clearance (P = .046), and showed the results to patients to enable feedback on their airway clearance technique (97% vs 76% vs, P = .007). Thirteen (19%) Canadian respondents indicated CPF was never measured. Reasons included no access to CPF equipment (7/13, 69%), using other measures (4/13, 31%), unfamiliar with CPF measurement (3/13, 23%), and not perceiving CPF to be useful to guide treatment (4/13, 31%). Prescription of airway-clearance strategies was based primarily on CPF results in the UK, whereas worsening symptoms (50%) was the most common reason for commencing therapy in Canada. Similar proportions of respondents in both countries measured CPF after initiation to ensure technique adequacy (73% vs 72%, P = .92).
A combination including all 3 airway-clearance techniques (ie, LVR + manually assisted cough + MI-E when the CPF ≤270 L/min was the airway clearance strategy most routinely recommended on initiation (41% overall, 54% in the UK and 32% in Canada). Single therapy was infrequent (LVR 15%, manually assisted cough 7%, and MI-E 4% in both countries). The most commonly prescribed minimum frequency of airway clearance in both countries was 2–3 times each day. More UK respondents indicated the presence of a standardized plan or guideline for monitoring cough strength and initiation of airway clearance techniques in their clinic or program (60% vs 38%, P = .02).
Of the UK respondents, 82% indicated their practice included always recommending or prescribing airway-clearance techniques when considered appropriate, whereas only 55% of Canadian respondents described such a practice; 15% of UK respondents and 29% of Canadian respondents indicated that they only sometimes recommended airway-clearance techniques, with the main reasons being anticipated non-adherence, inability to provide ongoing support or education, inability to access equipment for all patients, insufficient evidence of effectiveness for some patient groups, and impaired bulbar function. Referral to another clinic or specialist was the reason given by 10 respondents (2 from the UK and 8 from Canada) never recommended airway-clearance strategies.
Education for Patient and Families
All of the respondents indicated that initial teaching on airway-clearance techniques was provided either all of the time (UK 91%, Canada 26%) or some of the time (UK 9%, Canada 74%) in their clinic or program, most commonly by physiotherapists (UK) and respiratory therapists (Canada). Of the UK respondents, 59% reported initial teaching was provided in the home in addition to clinic teaching; ongoing support and troubleshooting at home was provided by 69%. The ability to conduct initial teaching (29%) and deliver ongoing support (39%) in the home was less frequent among Canadian respondents.
Constraints to Service Provision
More Canadians identified constraints to service provision, specifically insufficient public funding for equipment (68% vs 39%, P = .002) and inadequate knowledge of community workers (56% vs 34%, P = .02). Funding for support and troubleshooting in the home was a common constraint in both countries (49% vs 42%) (Fig. 1).
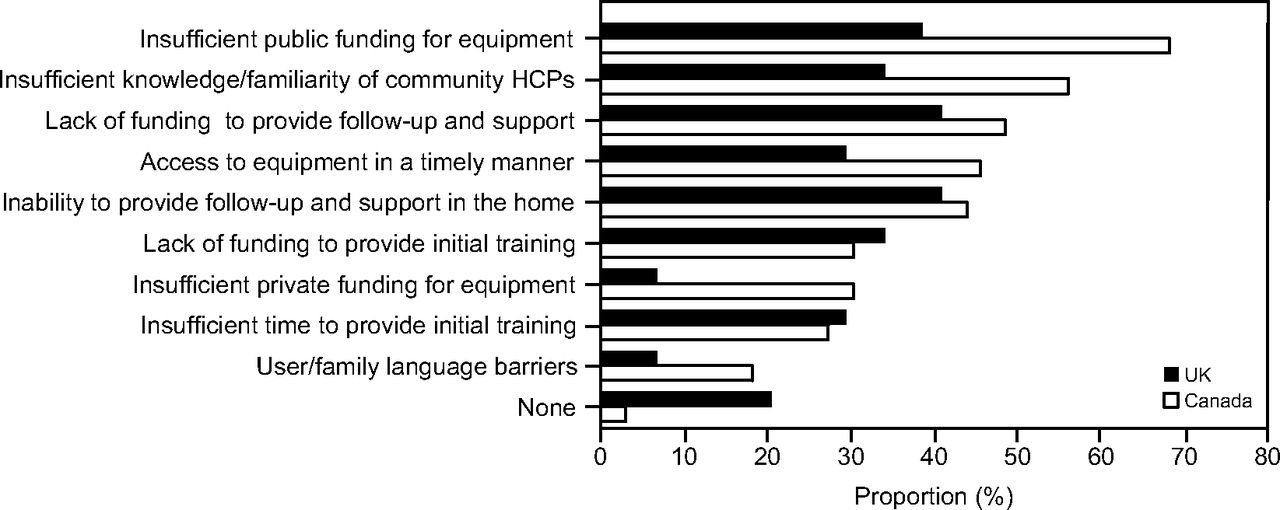
Constraints to service provision. HCP = health care provider.
Discussion
In this self-report survey of clinicians representing the range of professions involved in respiratory management of NMD and SCI, we found awareness of professional society guideline recommendations related to airway clearance was more common among United Kingdom clinicians than among Canadian clinicians. Routine assessment of cough strength and use of CPF to guide initiation of airway clearance, as recommended in guidelines, was also more common among UK clinicians. Frequently cited reasons for not using CPF by Canadian respondents related to a lack of access to necessary equipment and the use of other measures to guide therapy. Multiple airway-clearance techniques, used 2–3 times per day, was the most common airway-clearance prescription in both countries. More Canadian respondents reported constraints in service delivery, particularly insufficient public funding for equipment and insufficient knowledge of airway-clearance techniques on the part of community health care providers. Interestingly, despite 69% of UK respondents indicating that they provided ongoing support and troubleshooting in the home, lack of funding and inability to provide this type of support were the most frequently reported service constraints by UK respondents.
We found moderate awareness of guideline recommendations for monitoring of cough effectiveness and commencement of airway-clearance interventions. Lack of awareness of guideline recommendations is an obvious barrier to their adoption and application.17 Pertinent guidelines were published > 5 y before our survey, which arguably should be sufficient time for widespread dissemination.12,14 As members of the Canadian Thoracic Society Home Ventilation guidelines are on this research team, we are aware that dissemination was primarily passive, ie, via professional society endorsement, conference presentation, and peer-reviewed publication. We cannot comment on the processes used to disseminate the UK guidelines. Differences in the routine measurement of cough strength adequacy and the use of CPF to guide initiation of airway-clearance strategies in the UK and Canada may be attributable to differences in guideline awareness. Additional reasons may be the constraints reported by Canadian respondents to the use of CPF such as limited access to required equipment, although we cannot confirm if this refers to lack of access to portable peak flow meters or to more sophisticated pulmonary function testing, and the perception that CPF was not useful in guiding treatment decisions. Alternatively, differences between countries may be attributable to differences in our survey sample frame, as attendees of the United Kingdom Home Ventilation conference may be more invested in the delivery of airway-clearance interventions.
Among Canadian respondents, the most common constraint to ideal service provision was public funding of equipment. In Canada, a country comprising 10 provinces and 3 territories and a population of 35 milllion,18 most health care is funded through general taxation; however, public funding of assistive devices such as MI-E is highly variable and province-specific. For example, in Ontario, the most populous province, the provincial government funded the provision of MI-E starting in April 2014 (personal communication, Regina Pizzuti, Ventilator Equipment Pool). In British Columbia, publicly funded equipment for LVR is available through the Provincial Respiratory Outreach Program; access to MI-E for adults is limited and provided on a priority basis. In Alberta, there is no public funding of MI-E devices. In the United Kingdom, specialist centers may be contracted by their Clinical Commissioning Group, a clinically-led statutory National Health Service body responsible for commissioning of health care services for their local area, to provide equipment for airway clearance.19 Other providers may apply for public funding of equipment for an individual based on assessed need with a written application to their Clinical Commissioning Group, which may or may not be approved. We included the UK and Canada in this study due to relative similarities in terms of publicly funded universal health care and the publication of professional society guidelines with clear guidance on airway clearance. We did not include participants from the United States due to substantial differences in the provision of health care. However, our findings related to common practices in relation to assessment of cough strength and use of cough augmentation strategies may be similar in the United States and warrants investigation.
Other common constraints to ideal service provision were the knowledge possessed by community health care providers regarding airway-clearance techniques and the ability to provide support and follow up in the home. Again, in both the UK and Canada these aspects of care delivery are highly variable based on proximity to a specialist center and regional variation in service delivery models.20 In our previous national Canadian study of 152 home ventilation providers (113 local community, 38 institutional), 58% indicated they were able to provide some form of follow-up in the home, whereas only 41% indicated they provided training to community health care providers external to their institution.15 Although not specific to airway clearance, data from a qualitative interview study of 33 individuals receiving home ventilation and their family caregivers also identified a need for home outreach and increased training of community health care providers as potential facilitators to transition to home mechanical ventilation.21
Study Strengths and Limitations
Strengths of our study include the rigorous survey development process and data reflecting practices across 2 geographical regions. As with any self-report survey, our findings may reflect social desirability bias and are subject to selection bias. However, a strength of our data is that those who provide direct patient care (ie, respiratory therapists and physiotherapists) were well represented among survey participants. Differences in the sampling frame in the 2 countries may have resulted in the identified differences in guideline awareness and clinical practices. Furthermore, our findings may not be generalizable to clinicians managing patients outside of specialist NMD, SCI, or home mechanical ventilation clinics or centers who were likely not accessed through our sampling strategies.
Conclusion
In this self-report survey of clinicians in Canada and the United Kingdom providing care to patients requiring assistance with airway clearance, we found moderate awareness of guideline recommendations related to cough effectiveness monitoring. Awareness and practice adherence to guideline recommendations were more common among respondents from the UK, but this may be reflective of the sample frame. Although CPF was the most common test assessed in both countries, a wide range of other tests were used, including qualitative assessment, which may not be the optimal method to guide therapy. More Canadians reported constraints in service delivery, although insufficient public funding for equipment and the inability to provide support in the home were common constraints in both countries. The somewhat variable cough effectiveness monitoring and airway-clearance practices for NMD and SCI patients identified in this survey confirms the need for further knowledge translation work related to guideline recommendations and the need to address common constraints to optimal service delivery.
Acknowledgments
We acknowledge Gemma Howell, Rachel Moses, Victoria Hodgkinson, Lawrence Korngut, and Tova Plashkes for their assistance with the distribution of the survey and reminders.
Footnotes
- Correspondence: Louise Rose RN PhD, Sunnybrook Health Sciences Centre, 2075 Bayview Ave, Toronto, ON, Canada, M4N 3M5. E-mail: louise.rose{at}utoronto.ca
The authors disclose a relationship with Muscular Dystrophy Canada.
Supplementary material related to this paper is available at http://www.rcjournal.com.
Dr Rose presented a version of this paper at the International Conference of Home Mechanical Ventilation, held March 15-17, 2018, in Lyon, France.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}