

Abstract
BACKGROUND: Spontaneous breathing trials (SBTs) and daily sedation interruptions (DSIs) reduce both the duration of mechanical ventilation and ICU length of stay (LOS). The impact of these practices in patients with ARDS has not previously been reported. We examined whether implementation of SBT/DSI protocols reduce duration of mechanical ventilation and ICU LOS in a retrospective group of subjects with ARDS at a large, urban, level-1 trauma center.
METHODS: All ARDS survivors from 2002 to 2016 (N = 1,053) were partitioned into 2 groups: 397 in the pre-SBT/DSI group (June 2002–December 2007) and 656 in the post-SBT/DSI group (January 2009–April 2016). Patients from 2008, during the protocol implementation period, were excluded. An additional SBT protocol database (2008–2010) was used to assess the efficacy of SBT in transitioning subjects with ARDS to unassisted breathing. Comparisons were assessed by either unpaired t tests or Mann-Whitney tests. Multiple comparisons were made using either one-way analysis of variance or Kruskal-Wallis and Dunn's tests. Linear regression modeling was used to determine variables independently associated with mechanical ventilation duration and ICU LOS; differences were considered statistically significant when P < .05.
RESULTS: Compared to the pre-protocol group, subjects with ARDS managed with SBT/DSI protocols experienced pronounced reductions both in median (IQR) mechanical ventilation duration (14 [6–29] vs 9 [4–17] d, respectively, P < .001) and median ICU LOS (18 [8–33] vs 13 [7–22] d, respectively P < .001). In the final model, only treatment in the SBT/DSI period and higher baseline respiratory system compliance were independently associated with reduced mechanical ventilation duration and ICU LOS. Among subjects with ARDS in the SBT performance database, most achieved unassisted breathing with a median of 2 SBTs.
CONCLUSION: Evidenced-based protocols governing weaning and sedation practices were associated with both reduced mechanical ventilation duration and ICU LOS in subjects with ARDS. However, higher respiratory system compliance in the SBT/DSI cohort also contributed to these improved outcomes.
- acute respiratory distress syndrome
- daily sedation interruption
- mechanical ventilation
- spontaneous breathing trial
Introduction
Throughout the history of critical care medicine, there has been contention over the most effective weaning method from mechanical ventilation for patients with acute respiratory failure. In the 1990s, evidence from large, well-executed, prospective, randomized controlled trials demonstrated that the mode chosen to carry out weaning greatly influenced the duration required to liberate subjects from mechanical ventilation1; protocol-directed approaches to weaning were more efficient compared to physician-directed weaning (regardless of the ventilator mode used),2 and abrupt cessation of mechanical ventilation (ie, spontaneous breathing trials [SBT]) as part of a systematic approach to evaluating patient readiness to resume spontaneous breathing was the most effective and efficient method of discontinuing mechanical ventilation.3,4 In these studies, the duration of weaning was reduced by 1–2 d compared to more traditional methods,3 and the duration of mechanical ventilation was reduced from 6 to 4.5 d.4
In addition, sedation practices have been associated with prolonged duration of mechanical ventilation. The use of sustained sedation to manage anxiety and patient-ventilator asynchrony in critically ill patients has also contributed to increased ICU length of stay (LOS), development of acute delirium, and increased psychological sequelae such as post-traumatic stress disorder and chronic depression.5–9 In 2000, Kress et al10 reported the technique of daily sedation interruption (DSI) to evaluate the intensity of agitation and pain and to assess the impact of DSI on subject recovery. This strategy reduced the median duration of mechanical ventilation by 2.4 d and ICU LOS by a median of 3.5 d. Several years later, Girard et al11 reported that combining SBT with DSI increased mean ventilator-free days by 3.1 d, and reduced ICU LOS by 3.8 d. Moreover, the risk of death was substantially reduced. An alternative strategy of targeted light sedation has been shown to decrease the duration of mechanical ventilation by 1.2–2.6 d and decrease ICU LOS by 1.5–1.8 d.12 On the basis of these results, our institution implemented an SBT protocol in late 2007 and a DSI protocol in early 2008, with the integration of targeted light sedation in 2013.
Patients with ARDS represent a group of the critically ill likely to be problematic in weaning from mechanical ventilation. These patients often require prolonged mechanical ventilation due to severely impaired gas exchange, high ventilatory workloads, and a propensity for developing multi-organ system dysfunction. As a consequence, patients with ARDS are more likely to require high levels of sedation, analgesia, and more frequent need for neuromuscular blockade. In light of these potential barriers to recovery, we studied the impact of SBT/DSI and targeted light-sedation practices on the duration of mechanical ventilation and ICU LOS among subjects with ARDS who survived to hospital discharge. Given the propensity for prolonged mechanical ventilation duration and other factors that likely impede weaning, we also examined the efficacy of the SBT strategy in preparing subjects for a trial of extubation.
QUICK LOOK
Current knowledge
Using spontaneous breathing trials to wean patients from mechanical ventilation and managing sedation with daily sedation interruptions or targeted light sedation generally reduces the duration of mechanical ventilation and shortens the ICU length of stay for critically ill patients.
What this paper contributes to our knowledge
This study suggests that, in subjects with ARDS, these practices may result in even greater reductions in both the duration of mechanical ventilation and the length of stay in the ICU. Moreover, subjects recovering from ARDS do not have particular difficulty in passing a spontaneous breathing trial despite requiring prolonged periods of full ventilatory support.
Methods
Since 2002 our institution has maintained a database of all patients meeting the American-European Consensus Conference criteria for acute lung injury and ARDS.13 In light of the new Berlin definition,14 all patients were retrospectively reclassified accordingly. This database consists primarily of information gathered from the day of ARDS onset, including mechanical ventilation and gas exchange data, initial illness severity, and lung injury scores, as well as other demographic data. Outcome data included the duration of mechanical ventilation, ICU LOS, and post-ICU LOS. Both mechanical ventilation duration and ICU LOS accounted for failed extubation and ICU readmissions (ie, the additional days incurred by that subset of subjects were summed with the initial periods of mechanical ventilation and ICU LOS). In addition, during the first 2 years of the SBT protocol, data on the impact of SBT on weaning patients with ARDS also were available. Approval to use our quality assurance data was granted from our institutional review board.
Since September 2000, patients with ARDS and those at high-risk for developing ARDS have been managed with a lung-protective ventilation protocol that incorporated elements from both the ARDSNet ARMA and ALVEOLI trials.15,16 Attending ICU physicians are strongly encouraged to follow the protocol and are at liberty to modify the protocol as deemed necessary.
Beginning in November 2007 in the 14-bed medical ICU, and in April 2008 in the 16-bed trauma-surgical/neurologic ICU, weaning was guided by an SBT protocol similar to that described by the Spanish Lung Failure Collaboration Group.17,18 In brief, patients were screened daily by respiratory therapists for weaning readiness criteria as described in the aforementioned studies.1–3,17,18 SBTs were done with pressure support ventilation set to 7 cm H2O above a PEEP level of 5–8 cm H2O. Extubation was performed at the discretion of the attending physician and was considered after passing a 2-h SBT. Those failing an SBT usually were managed with volume control ventilation at a tidal volume (VT) between 6–8 mL/kg, and less commonly at higher levels of pressure support (eg, ΔP ∼15 cm H2O). The practices of DSI and targeted light sedation were based on the methods described in the aforementioned studies.10,11,19
The primary database was queried for all ARDS survivors, and these data were partitioned into 2 groups: the pre-SBT/DSI group (June 2002–December 2007) consisting of 397 subjects, and the post-SBT/DSI group (January 2009–April 2016) with 656 subjects; 99 patients with ARDS from 2008 (the transition period) were excluded from the analysis. Data included mechanical ventilation duration, ICU LOS, lung injury score,20 Acute Physiology and Chronic Health Evaluation (APACHE II) score,21 Severe Acute Physiology (SAPS II) score,22 age, sex, and race/ethnicity. Pulmonary-specific variables included VT, oxygenation index, the ratio of PaO2 to FIO2, plateau pressure (Pplat), driving pressure (Pplat-PEEP), and compliance of the respiratory system (CRS), all of which were measured both on the day of ARDS onset and on ARDS day 2. The primary outcome was the duration of mechanical ventilation, and the secondary outcome was the ICU LOS between pre-protocol and post-protocol implementation. Each treatment group also was analyzed according to either ARDS severity (ie, Berlin classification of mild, moderate, or severe) or primary ARDS etiology (aspiration, pneumonia, non-pulmonary sepsis, trauma, or other sources).
Specific data on how quickly subjects with ARDS achieved unassisted breathing with an SBT strategy were gleaned from another quality assurance database during the first 2.5 y after implementation of the SBT protocol. This included a subset of 169 subjects with ARDS (108 medical and 61 surgical, trauma, neurotrauma) who required ≥ 48 h of mechanical ventilation, survived long enough to reach weaning readiness criteria, and received at least one SBT. Variables of interest included the duration of mechanical ventilation prior to reaching weaning readiness criteria, the number of SBTs required to pass a 2-h trial, the number of days from first passing an SBT to the first trial of extubation, and the percentage of subjects requiring re-intubation. These subjects had been categorized as either medical or surgical ARDS for quality-assurance purposes.
Statistical analysis was performed using either Stata 9.0 (Stata Corp, College Station, Texas) or Instat (Graphpad Software, La Jolla, California). Data were reported as either mean ± SD or median (IQR). Statistical analysis used 2-sided unpaired t tests for normally distributed data and Mann-Whitney tests for non-normally distributed data. Normality was assessed with the Kolmogorov-Smirnov test. Multiple comparisons were made using either one-way analysis of variance or Kruskal-Wallis and Dunn's multiple comparison tests. Dichotomous data were analyzed with a 2-sided chi-square test. Differences were considered statistically significant when P < .05.
We assessed the magnitude of pre- versus post-protocol differences in mechanical ventilation duration and ICU LOS adjusted for potential confounding variables using linear regression. Our initial model included mechanical ventilation duration and ICU LOS along with demographic information (sex, race/ethnicity), APACHE II, SAPS II, lung injury score, Berlin definition category, primary ARDS etiology, presence of sepsis, and primary managing service. Pulmonary mechanics and oxygenation variables added to the model included VT, Pplat, Pplat-PEEP, CRS, PaO2/FIO2, and oxygenation index. We also included the most abnormal values of pH, base deficit, mean arterial blood pressure, total bilirubin, serum creatinine, and urine output from the day of ARDS onset. Variables with non-normally distributed data were converted to logarithmic scale (eg, VT and oxygenation index). We removed all variables with P > .10 and refit the model. In the final model, we reported the adjusted magnitude of pre- versus post-protocol differences in the primary and secondary outcomes along with all variables in which P < .05.
Results
Impact of SBT/DSI Protocols
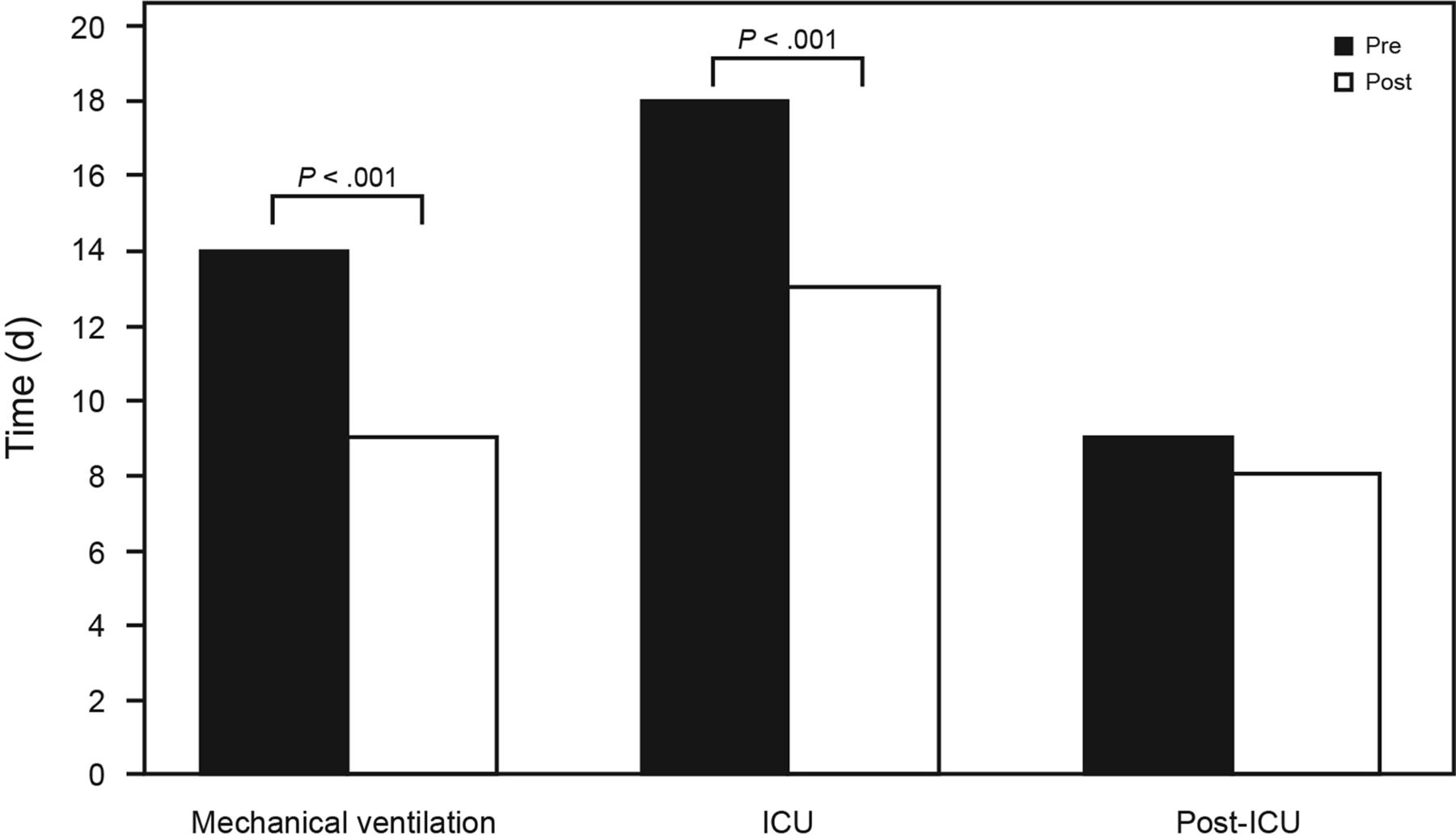
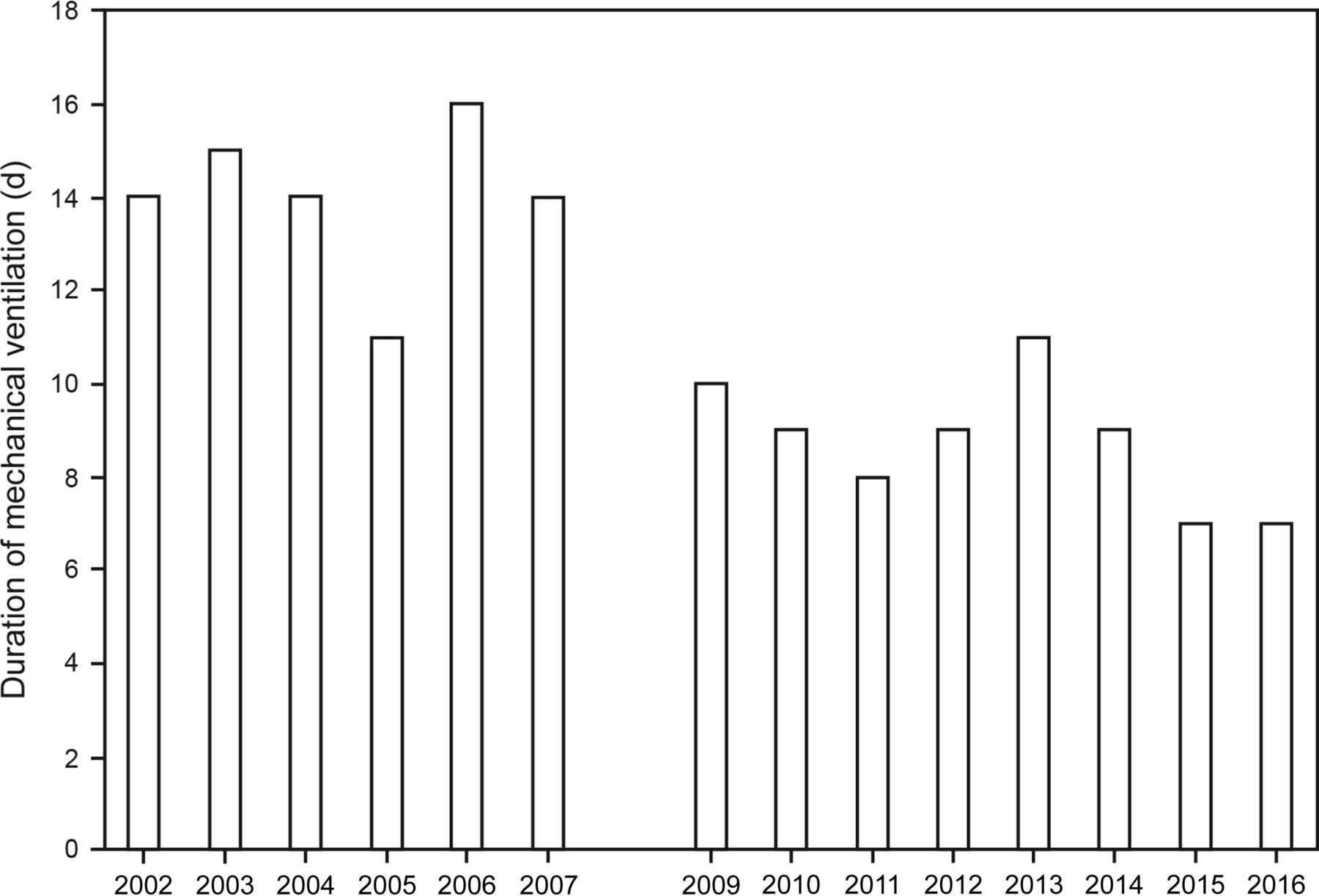
The introduction of SBT and conservative sedation practices was associated with a 5-d median reduction in both mechanical ventilation duration and ICU LOS (P < .001), with no difference in post-ICU LOS (P = .39) (Fig. 1). There was no historical trend toward either reduced mechanical ventilation duration or ICU LOS when pre-SBT/DSI period data were analyzed from 2002 through 2007 (P = .80 and .23, respectively) (Fig. 2, 3). Subjects in the post-SBT/DSI group were significantly older and had higher illness severity, lung injury severity, and oxygenation defects at ARDS onset (Table 1). There were also significant differences in ventilator management between the 2 groups on the day of ARDS onset, because the post-SBT/DSI group received more stringent lung-protective ventilation (ie, lower VT, Pplat, and Pplat-PEEP). However, when reassessed on ARDS day 2, there were no differences between cohorts in VT, PEEP, PaO2/FIO2, and oxygenation index (see Supplementary Table 1 at http://www.rcjournal.com). Nonetheless, significant differences between cohorts persisted in Pplat, Pplat-PEEP, and CRS, suggesting less impaired chest mechanics in the post-SBT/DSI group.

Differences in median duration of mechanical ventilation, ICU length of stay, and post-ICU length of stay between the pre-protocol group and the post-protocol group whose weaning and sedation were governed by spontaneous breathing trials and daily sedation interruptions.
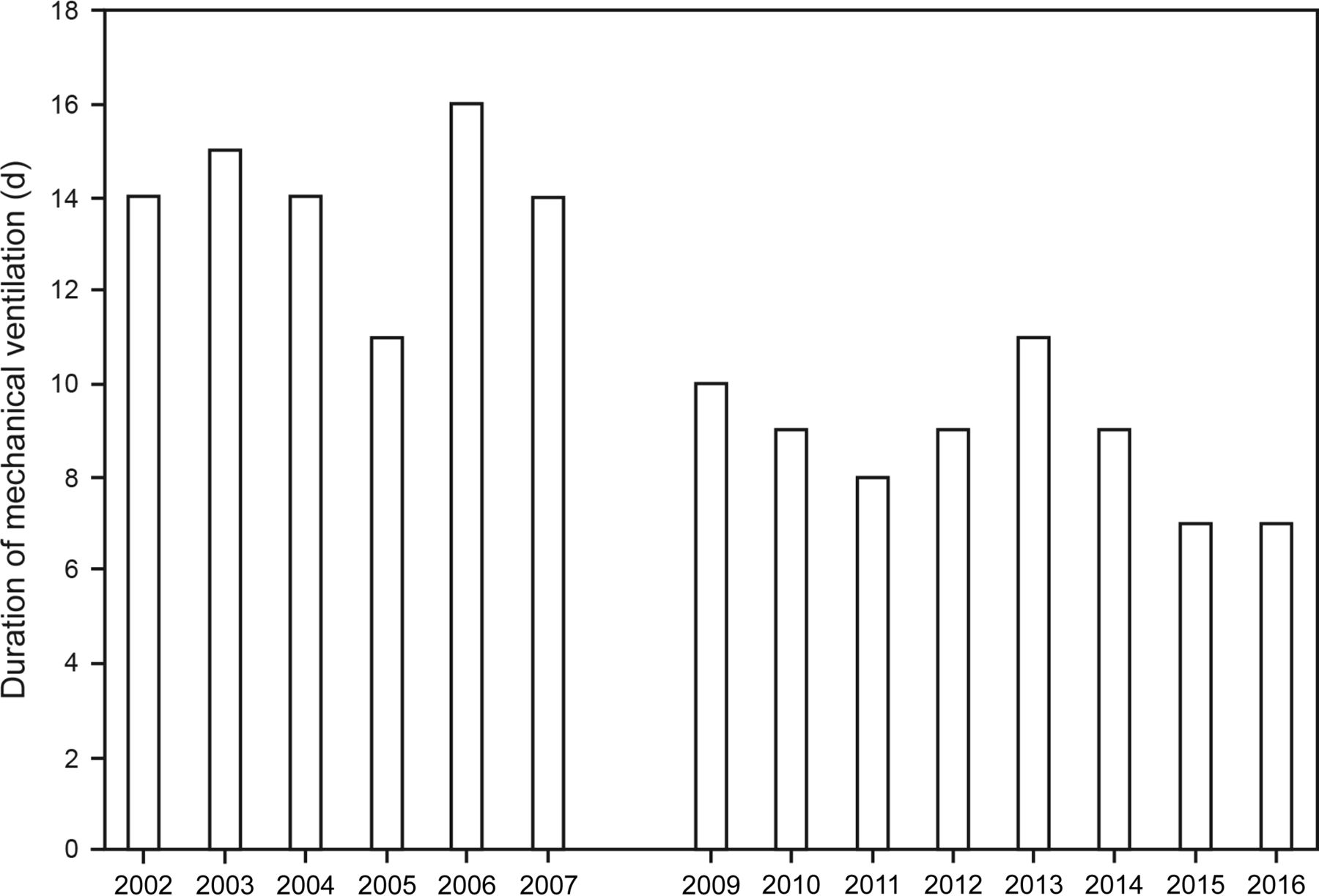
Median, annual duration of mechanical ventilation between the pre-protocol (2002–2007) and post-protocol (2009–2016) groups.

Median, annual ICU length of stay between the pre-protocol (2002–2007) and post-protocol (2009–2016) groups.
Baseline Characteristics on the Day of ARDS Onset
Each treatment group was analyzed further according to ARDS severity (ie, Berlin classification of mild, moderate, or severe),14 primary ARDS etiology (aspiration, pneumonia, non-pulmonary sepsis, trauma, or other causes), and re-intubation rate. Regardless of ARDS severity, subjects in the post-SBT/DSI group experienced significant reductions in duration of mechanical ventilation and ICU LOS; the only exception was ICU LOS for subjects with moderate ARDS (P = .062) (see Supplementary Table 2 at http://www.rcjournal.com).
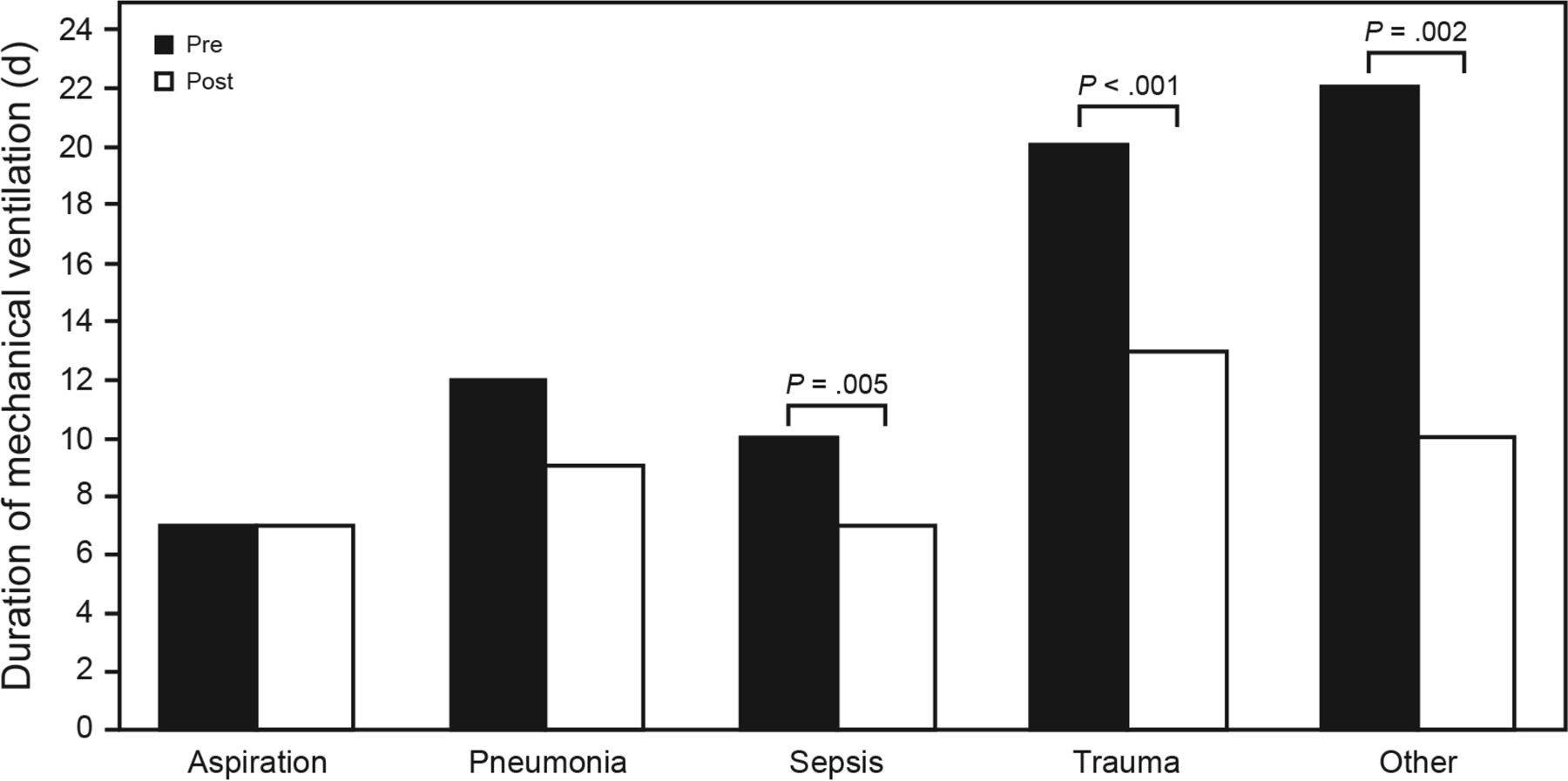
When analyzed according to ARDS etiology, both mechanical ventilation duration and ICU LOS decreased consistently in the post-SBT/DSI group, the only exception being subjects with aspiration. However, the decrements in duration achieved statistical significance only for mechanical ventilation days in subjects with non-pulmonary sepsis, trauma, and other less common ARDS etiologies (Fig. 4), and for ICU LOS only in subjects with trauma and other etiologies (Fig. 5). There was no difference in re-intubation rates between the pre-SBT/DSI and post-SBT/DSI treatment groups (14% vs 13.7%, respectively; risk ratio 1.02 [0.80–1.31], P = .98), nor were there differences in ICU readmission rates (10.6 vs 9.8%; risk ratio 1.09 [0.73–1.65], P = .75).

Differences in mechanical ventilation duration between the pre-protocol and post-protocol groups analyzed according to ARDS etiology. Note that sepsis is non-pulmonary sepsis.
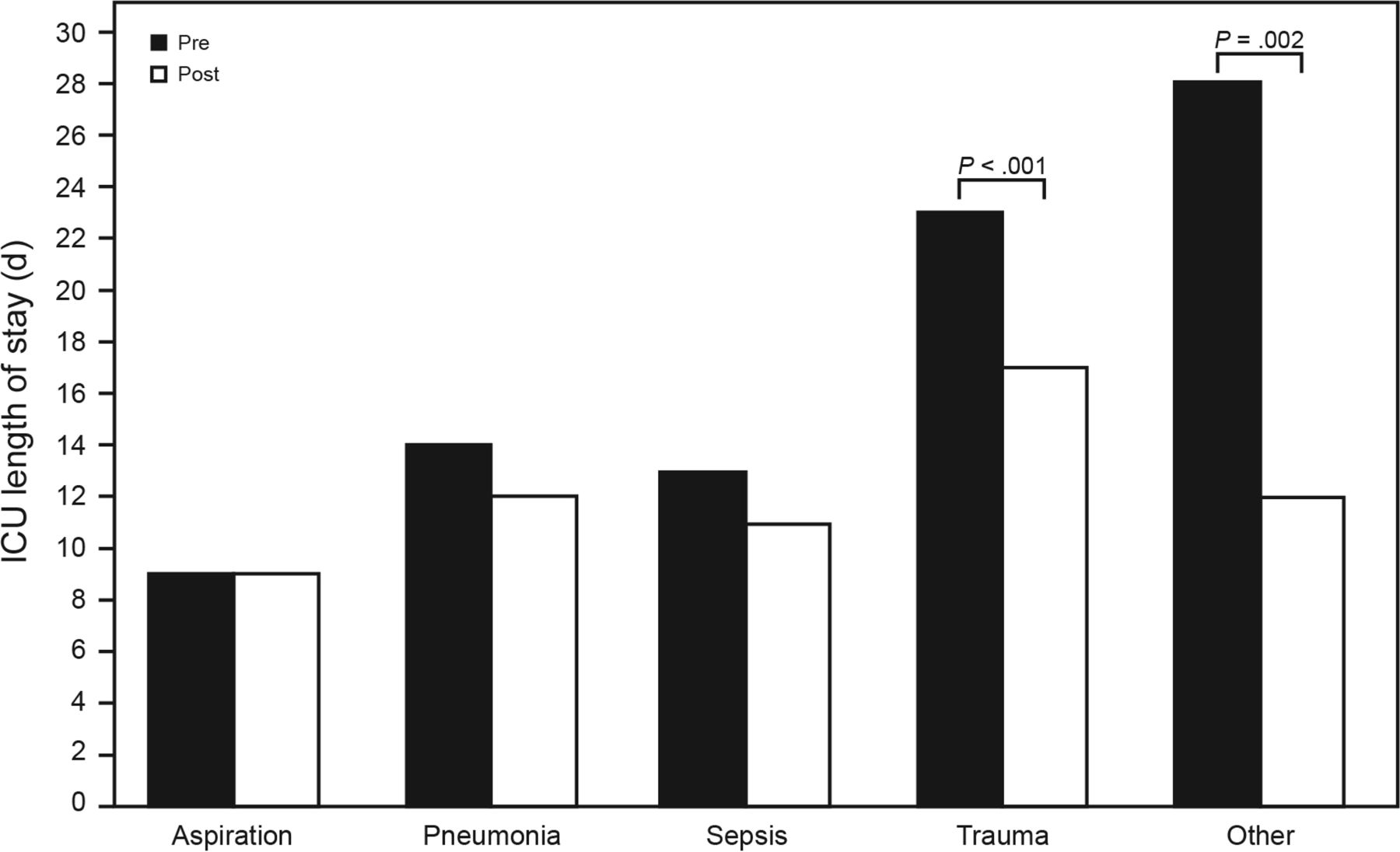
Differences in ICU length of stay between the pre-protocol and post-protocol groups analyzed according to ARDS etiology. Note that sepsis is non-pulmonary sepsis.
Analyzing subjects according to the primary care service revealed strong trends toward reduced mechanical ventilation duration in the post-SBT/DSI period among subjects in the medicine and neurosurgery/neurology cohorts, whereas highly significant reductions were observed in the surgery/trauma cohorts (see Supplementary Table 3 at http://www.rcjournal.com). ICU LOS was significantly lower during the post-SBT/DSI periods among subjects in both the surgery/trauma and neurosurgery/neurology cohorts.
In the final model, both the post-SBT/DSI implementation period and increasing CRS were independently and significantly associated with reduced duration of mechanical ventilation, whereas increasing Pplat and base deficit were independently associated with increasing duration of mechanical ventilation (Table 2). In addition, other factors such as ARDS etiology and subject classification by primary care service were associated with increased mechanical ventilation duration. First, relative to aspiration as the primary etiology, ARDS associated with either pneumonia or trauma was associated with increased mechanical ventilation duration. Second, classifying subjects by primary care service as trauma/surgical, neurosurgical/neurology, and other services also was independently associated with increased mechanical ventilation duration compared to those classified as medical.
Adjusted Regression Coefficients of Factors Determining Mechanical Ventilation Duration
There were similar findings in the adjusted analysis of variables associated with ICU LOS. The only differences were that CRS was excluded from the final model, whereas the category of other ARDS etiology and a co-diagnosis of sepsis were found to be independently associated with increased ICU LOS (Table 3). Only management in the SBT/DSI cohort was significantly associated with decreased ICU LOS.
Adjusted Regression Coefficients of Factors Determining ICU Length of Stay
Efficacy of SBT in Achieving Unassisted Breathing
In analyzing the efficiency of SBT to facilitate the resumption of unassisted breathing, subjects with ARDS achieved unassisted breathing at a median of 1 d after initiation of SBT, or 2 trials. By the third SBT, the cumulative pass rate was 69% and 82% for medical and surgical ARDS subjects, respectively. In surgical ARDS, this was attained despite subjects having been ventilator-dependent for a median of 9 d (Table 4). Re-intubation rates were not different between medical and surgical ARDS subjects (14% vs 12%, respectively; risk ratio 0.84 [0.42–1.70], P = .81).
Weaning Characteristics in a Subset of Subjects Based on Surgical vs Medical ARDS
We also analyzed the efficacy of weaning by SBT on a subset of subjects with medical and surgical ARDS who required at least 2 weeks of full ventilatory support prior to meeting weaning readiness criteria. Only 3 subjects with medical ARDS required 14–37 d of mechanical ventilation prior to meeting weaning readiness criteria. Of these 3 subjects, the 2 who required continuous mechanical ventilation for 34 d and 37 d passed their initial SBT. Among the 20 subjects with surgical ARDS who required 14–47 d of mechanical ventilation, 9 (45%) were able to pass their first SBT, and an additional 4 (20%) subjects passed an SBT on the second day.
Discussion
Subjects with ARDS managed with current, evidenced-based practices for weaning by SBT and sedation managed by DSI and/or targeted light sedation required substantially less time receiving mechanical ventilation and fewer days of care in the ICU compared to physician-directed, usual-care practices in place prior to 2008. While our results corroborate the findings from prior studies, we found a greater reduction in both mechanical ventilation duration and ICU LOS among subjects with ARDS than that previously reported for the general ICU population. Moreover, despite requiring extended durations of full ventilatory support, the majority of our subjects with ARDS experienced relatively little difficulty in resuming unassisted breathing when weaned with an SBT protocol.
To our knowledge, we are the first to have examined specifically the impact of adopting SBT/DSI and targeted light sedation practices on the duration of mechanical ventilation and ICU LOS in subjects with ARDS, a segment of critically ill subjects who often are perceived as being relatively difficult to wean. In our study, the magnitude of impact that these protocols had on duration of mechanical ventilation and ICU LOS was unexpected. However, this may in part reflect our own history of managing subjects with ARDS (particularly surgical-trauma ARDS) with generous amounts of analgesics and sedatives both during the pre- and early post- lung-protective ventilation eras.23,24
When we examined data by primary ARDS etiology, it appeared that the predominant impact of SBT/DSI in reducing mechanical ventilation duration occurred in those with sepsis, trauma, and other less common etiologies. Therefore, we suggest that subjects with ARDS who are more likely to have complicated courses (eg, those with multi-organ failure or multi-organ traumatic injury) may benefit the most from management with SBT/DSI strategies. This interpretation is also supported by the results of the linear regression analysis, in which several variables were independently associated with increased duration of mechanical ventilation and ICU LOS. In particular, subjects with trauma-associated ARDS, subjects with increasing base deficit at ARDS onset, and subjects whose condition required management in the trauma, surgical, and neurocritical care settings all were independently associated with increased mechanical ventilation duration and ICU LOS (as was a co-diagnosis of sepsis with ICU LOS).
Likewise, when examined according to the Berlin definition of ARDS, the post-implementation group experienced significantly fewer mechanical ventilation days across all categories, as well as significantly less time in the ICU for those with mild and severe ARDS. It is unclear why the reduction in ICU LOS in moderate ARDS was not statistically significant. However, the Berlin definition categories are predicated solely upon cut-off values of PaO2/FIO2; this is perhaps too crude a measure to account for the numerous factors that determine ICU LOS, many of which are non-pulmonary.
The interpretation of our results must also take into consideration that our post-SBT/DSI subjects had higher CRS during the first few days of ARDS. As a consequence, they also had lower Pplat and lower driving pressure (Pplat-PEEP). This has been associated with reduced risk for developing ventilator-induced lung injury that, in turn, may have contributed to their reduced mechanical ventilation duration, as has been demonstrated by others during lung-protective ventilation.25
The impact of SBT/DSI protocols can be appreciated by reviewing the standard of care in the early 1990s. Particularly striking is the duration of mechanical ventilation prior to meeting weaning readiness criteria. Two of the seminal weaning studies required relief from sedation or no further need for sedation as a criterion to begin weaning1,3 This may partly explain why subjects in various treatment arms required mechanical ventilation that ranged from 6.5 ± 4.5 to 17 ± 31 d prior to weaning, with most exceeding a mean of 10 d. Moreover, an examination of the duration of several gradual weaning strategies, which represented the prevailing methodology from the mid-1970s to the 1990s, revealed that gradual weaning strategies (regardless of the specific methodology) increased the duration of mechanical ventilation by an average of 5.7 ± 3.7 d with pressure support and 9.3 ± 8.2 d with T-piece trials and intermittent mandatory ventilation.1
Thus it appears that two of the greatest impediments to successful ventilator liberation toward the end of last century were overly liberal sedation combined with overly conservative weaning practices. Our judgment that the approach to weaning during that period was excessively conservative was underscored by Esteban et al,3 who attempted to study the effects of various weaning techniques in subjects deemed to be difficult. These subjects had been managed with continuous mechanical ventilation for 7.5 ± 6.1 d prior to study enrollment. To be randomized to receive a specific weaning strategy, subjects had to fail a screening SBT. However, 76% of enrolled subjects passed their initial SBT screening trial and could not be randomized. These findings, along with our own data, support the notion that use of full ventilatory support modes (eg, time-cycled, volume, pressure, or dual-control continuous mechanical ventilation) during the acute phase of critical illness does not, in and of itself, impede the process of liberating patients from mechanical ventilation.
The primary limitation of our study is the retrospective nature based on data collected for quality-assurance purposes at a single hospital. As such, it possesses neither the same rigor nor scope of data collection to account for protocol execution and control of confounding variables. For example, we lacked the resources to capture and analyze continuous electronic data. Therefore, all data were transcribed by hand, which greatly limited the amount and detail of information that could be accessed. This also impaired our ability to rigorously ascertain how faithfully protocols were followed throughout the study period.
Therefore, generalizing our findings to patients with ARDS in other settings is potentially limited. However, it should be noted that, as a major urban public hospital and level-1 trauma center, our ARDS population was diverse. Etiologies for ARDS in our subject group included pneumonia (33%), trauma (25%), non-pulmonary sepsis (17%), and aspiration (14%), as well as 11% from other sources (most often pancreatitis, transfusion-related acute lung injury, and inhalation injury). Despite the above enumerated limitations, the size and duration of data and consistent results suggests that evidenced-based practice changes initiated outside of a clinical research setting positively affects patient-centered outcomes in subjects with ARDS.
Conclusions
In summary, adoption of evidenced-based protocols for weaning and sedation practices in those with ARDS was associated with large reductions in mechanical ventilation duration and ICU LOS. These observations hold true regardless of ARDS severity and were particularly effective in subjects with etiologies associated with non-pulmonary sepsis and trauma, as well as less common sources of acute lung injury. Moreover, irrespective of mechanical ventilation duration, the majority of subjects with ARDS experienced little difficulty in achieving unassisted breathing when an SBT was used as the weaning method. Furthermore, our study suggests that, despite the inherent difficulty of maintaining strict adherence to protocols in clinical practice, considerable improvements in patient-centered outcomes can be achieved and may have the greatest impact for the sickest patients.
Finally, during the first 2 d of ARDS, the post-SBT/DSI group was observed to have high CRS and both lower Pplat and driving pressure, which are variables associated with reduced risk for ventilator-induced lung injury. That higher CRS was independently associated with reduced mechanical ventilation days in our post-SBT/DSI subjects underscores the importance of minimizing the risk of stretch-related injury during ARDS.
Acknowledgments
We wish to thank the respiratory therapists, critical care nurses, and physicians whose cooperation, teamwork, and diligence in implementing these protocols produced these results. Without their collective multidisciplinary efforts, this study would not have been possible.
Footnotes
- Correspondence: Richard H Kallet MSc RRT FAARC, Department of Anesthesia and Perioperative Care, Zuckerberg San Francisco General Hospital and Trauma Center, Bld 5: GA-2, 1001 Potrero Ave, San Francisco, CA 94110. E-mail: rich.kallet{at}ucsf.edu
Supplementary material related to this paper is available at http://www.rcjournal.com.
A version of this paper was presented by Ms Yip as an Editors' Choice abstract at the AARC Congress 2016, held October 15–18, 2016, in San Antonio, Texas.
The authors have disclosed no conflicts of interest.
See the Related Editorial on page 119
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}