

Abstract
BACKGROUND: Although routine physical activity for individuals with COPD is recommended, there are inherent limitations of available oxygen delivery devices that may result in hypoxemia during activity. Changes in Medicare laws have resulted in an increased use of oxygen cylinders and a reduction in the use of liquid oxygen devices. The aim of this survey was to assess the impact of perceived satisfaction with various oxygen delivery devices on perceived mobility and quality of life (QOL) of oxygen-dependent subjects with COPD.
METHODS: A survey was developed to measure perceived satisfaction with current portable oxygen delivery devices, perceived mobility, and perceived QOL. The survey was deployed via a link posted on the COPD Foundation's COPD360SOCIAL social media site for 5 weeks, which resulted in the recruitment of 529 participants, of which 417 were included in the data analysis.
RESULTS: Quantile regression analysis revealed that the median perceived device satisfaction score was significantly higher in the liquid oxygen device group (P < .001) compared with the portable oxygen cylinder and portable oxygen concentrator (POC) groups. The median perceived mobility score was significantly higher in the liquid oxygen device group (P < .001) compared with the portable oxygen cylinder group, but not the POC group. The median QOL score was significantly higher in the liquid oxygen device group (P < .001) compared with the POC and portable oxygen cylinder groups. Moreover, partial least-squares structural equation modeling regression analysis showed that perceived mobility is significantly affected by perceived satisfaction with the long-term oxygen therapy (LTOT) device (adjusted R2 = 0.15, P < .001), and perceived QOL is significantly affected by both perceived satisfaction with the LTOT device and perceived mobility (adjusted R2 = 0.45, P < .001).
CONCLUSIONS: For individuals with COPD requiring LTOT, perceived satisfaction with a portable LTOT device significantly and positively affects perceived mobility and QOL.
Introduction
Chronic lower respiratory diseases, which include primarily COPD, are the third leading cause of death in the United States and are projected to be the fourth leading cause of death worldwide and seventh in morbidity burden by 2030.1,2 COPD is a debilitating illness characterized by remodeling of the airways and lung parenchyma, leading to persistent air-flow limitation that is not fully reversible. Many individuals with COPD experience hypoxemia of varying severity because of the air-flow limitations and the physiologic changes of the lungs. Two seminal studies and a subsequent Cochrane review have contributed to our knowledge regarding the beneficial effects of long-term oxygen therapy (LTOT) in individuals with COPD.3–5 In response to these 2 studies that demonstrated a decrease in the mortality rate of individuals with COPD and severe hypoxemia, LTOT has been established as a standard of care for such individuals. However, a noteworthy criticism of these 2 pivotal studies concerns the failure of the researchers to measure impact of LTOT on the health-related quality of life (HRQOL) in the study participants. Considering that COPD is an incurable disease, improving HRQOL is an important goal in the management of individuals with COPD.
Until the 21st century, instruments used to measure HRQOL relevant to the COPD population were disease-specific and included measures related to respiratory signs and symptoms, such as dyspnea, cough, sputum characteristics, wheezing, and chest tightness.6–8 However, because of the heterogeneity of COPD and the comorbid conditions that are often associated with it, researchers and practitioners have begun to use generic HRQOL measures in conjunction with disease-specific measures to evaluate outcomes of various interventions.9–12 For example, Engström et al13 argued that disease-specific HRQOL measures were not sufficient to examine the effect of COPD on life functions due to comorbidities frequently seen in the COPD population. In a study that assessed the HRQOL in individuals with varying severity of COPD, the researchers found that disease-specific HRQOL indicators correlated well with measures of lung function, but generic HRQOL indicators that measure emotional status and psychosocial function correlated poorly with measures of lung function. The researchers noted that because COPD is associated with multiple comorbid conditions, such as heart disease and diabetes, the comprehensive effects of COPD that are attributable to the pulmonary and non-pulmonary components are best measured with both disease-specific and generic HRQOL instruments.
The American Thoracic Society and the European Respiratory Society have jointly issued a statement regarding research priorities for improving outcomes in COPD. The statement emphasizes the importance of using outcome measures, such as quality of life (QOL), that matter to individuals with COPD (ie, outcomes that are patient-centered) to determine the effectiveness of interventions. This is because surrogate measures, including physiological variables, such as FEV1 and 6-min walk distance, as well as anatomical variables, such as imaging and histological findings, do not correlate well with patient-centered outcomes, such as dyspnea, frequency of hospitalizations, QOL, and mortality.14
There is mounting evidence that lack of physical activity contributes to COPD exacerbation, resulting in increased utilization of health-care resources. A Belgian study found that COPD subjects with a low activity level had more frequent COPD exacerbation episodes and hospitalizations than subjects with a higher activity level as measured via an accelerometer-based activity monitor for 12 h/d. The researchers also found that 6-min walk distance was lower in readmitted COPD subjects 8 d into their hospital stay than in their counterparts who stayed out of the hospital.15 A more recent study at a Veterans Affairs health-care system in the United States, in which subjects were matched on percent-of-predicted FEV1 and previous exacerbation, found that the risk for exacerbations and COPD-related hospitalizations was significantly higher for individuals with COPD who had a low activity level as compared with individuals who were more active.16 Findings from a subsequent retrospective cohort study of 6,042 subjects by Nguyen et al17 demonstrated that self-reported moderate or vigorous physical activity of 150 min/week, as recommended, was associated with a 34% lower risk of 30-d readmission compared with inactive subjects (relative risk 0.66, 95% CI 0.51–0.87).
Besides the fact that physical activity is an intervention that is currently recommended in evidence-based guidelines for individuals with COPD, the ability to engage in physical activity is an outcome measure that matters to many individuals because it is a personal goal that affects perceived QOL. However, due to inherent limitations of available oxygen delivery devices, engaging in regular physical activity may be a challenge for individuals with COPD who require LTOT to mitigate the deleterious effects of hypoxemia. A complicating issue in the United States is that changes in Medicare regulations have resulted in the replacement of liquid oxygen delivery devices with portable oxygen cylinders. The aim of this survey was to assess the impact of perceived satisfaction with various portable oxygen delivery devices on the mobility and QOL of oxygen-dependent COPD subjects.
QUICK LOOK
Current knowledge
Oxygen therapy is a well-established standard of care for individuals with COPD and severe hypoxemia. More recently, routine physical activity has been added to the repertoire of evidence-based COPD interventions. Long-term oxygen therapy (LTOT) devices that are not portable may adversely impact the ability of oxygen-dependent individuals with COPD to engage in recommended routine physical activity and, ultimately, their quality of life. The current evidence regarding the impact of portable, lightweight LTOT devices on routine physical activity of these individuals is inconclusive.
What this paper contributes to our knowledge
A validated survey was used to assess the impact of perceived satisfaction with 3 types of LTOT devices on the perceived mobility and perceived quality of life of oxygen-dependent individuals with COPD. Analysis of survey results revealed that in oxygen-dependent individuals with COPD, perceived satisfaction with an LTOT device affects perceived mobility. Perceived satisfaction with an LTOT device and perceived mobility were also found to affect perceived quality of life.
Methods
Study Design and Participants
This cross-sectional study utilized a survey instrument that was developed to measure survey participants' satisfaction with their oxygen delivery device(s) and perceived mobility using the maximal life space component of the UAB Study of Aging Life-Space Assessment (with permission) in conjunction with self-reported walk distance (ranging from one quarter of a mile to ≥1 mile) and walk frequency (ranging from none to every day of the week) to measure participant mobility. The inclusion of this well-validated and reliable scale helped to create a survey that uniquely addressed the goals of the study.18,19 The survey instrument also included a QOL scale. The survey's Likert-type QOL scale was informed by several validated QOL instruments, including the World Health Organization Physical QOL survey. The survey instrument was subsequently converted to a web-based format and hosted on REDCap, a secure, web-based application designed exclusively to support data capture for research studies. A link to the survey was distributed to potential participants by posting to a social media site. The survey feature of REDCap was configured to preserve the anonymity of survey participants such that no personal identifiers, including IP addresses, were obtained. Demographic data regarding age, sex, length of COPD diagnosis, COPD severity, oxygen device use, and Medicare recipient status was collected. Study approval was obtained from our institutional review board.
Data Collection
The COPD Foundation enabled the collection of data by publishing the survey link on their COPD360SOCIAL social media site for 5 weeks. The target population consisted of oxygen-dependent subjects with COPD, the majority of whom use Medicare to pay for their oxygen supplies.
Statistical Analysis
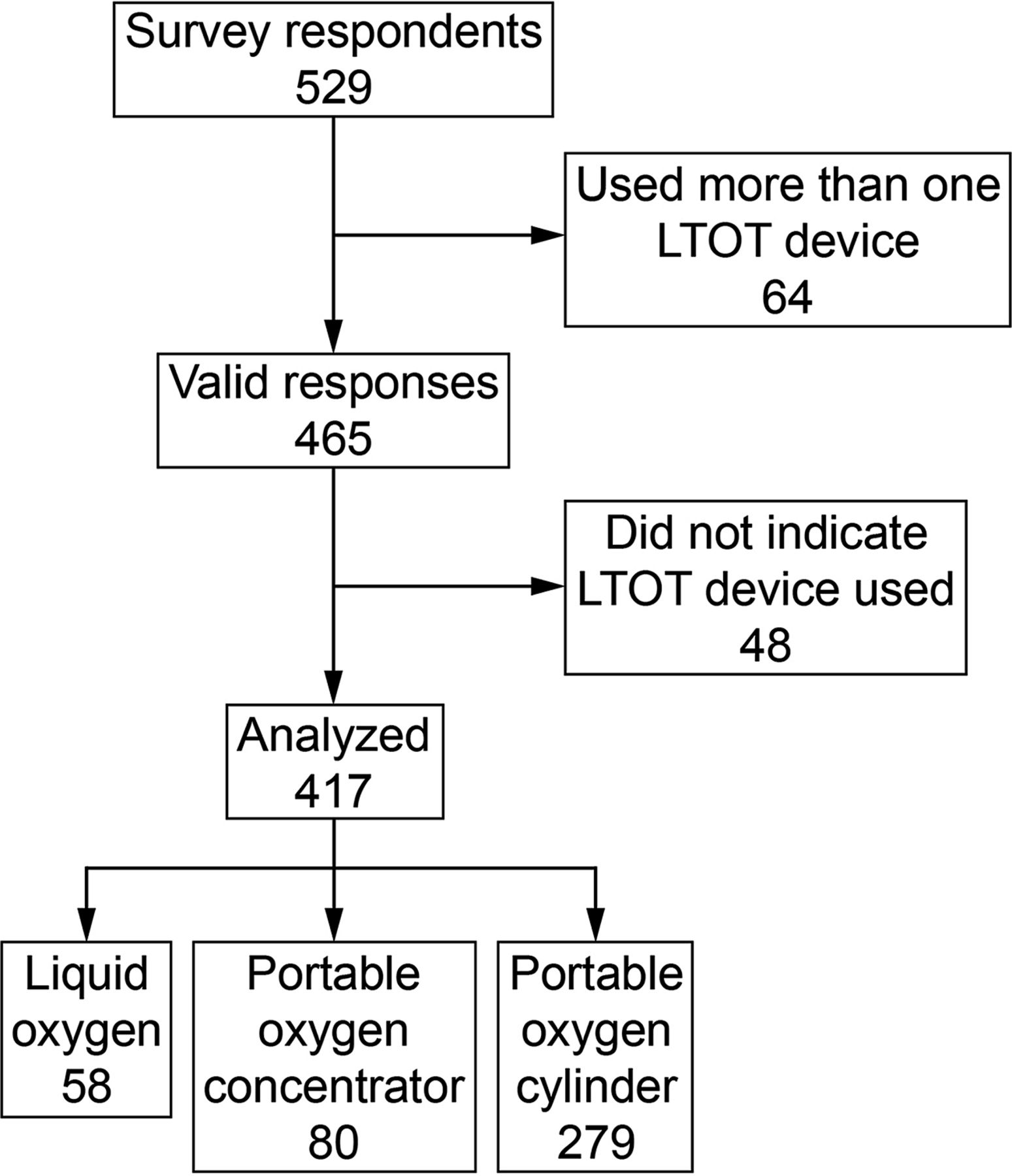
Among 529 survey respondents, to avoid any mixture, we focused only on subjects with one single LTOT device (n = 465). We subsequently excluded subjects with any missing values (n = 48). Although 10% of the data are missing, there is no statistically significant difference in characteristics between subjects with and without missing data (not shown). Given that missing completely at random assumption may hold (i.e., missing data is independent of bias in the research process), we proceeded with the analysis using complete cases.
We evaluated the reliability and discriminant validity of the mobility, QOL, and device satisfaction scales using Cronbach's α and Fornell–Larcker criterion, respectively. Convergent validity was assessed by computing the average variance extracted for all of the items used to measure each construct.20,21 Convergent validity demonstrates the strength of the relationship between the different indicators used to measure the same construct and explains the average amount of variance that a construct explains in its indicator variables relative to the overall variance of its indicators.21 An average variance extracted of 0.5 or greater is considered acceptable as it indicates that the construct explains >50% of its indicators' variance.20,21 The composite score of each scale (mobility, QOL, and device satisfaction) of the survey instrument consists of only verified items. The composite scores for the QOL and device satisfaction scales were obtained by averaging each participant's responses to the multiple verified items on the survey instrument that measure QOL and device satisfaction, respectively. Composite scores for the mobility scale were calculated using a specific computational algorithm based on each participant's responses to the multiple verified items that measure mobility. The results of these assessments presented in Tables 1 and 2 demonstrate acceptable psychometric properties of the survey instrument.
Survey Reliability and Validity Assessment Summary
Fornell–Larcker Criteria for Discriminant Validity
The sample was summarized across device groups by using the frequency with the percentage for categorical variables and the median with the interquartile range for continuous variables. We assessed the distributional difference across device groups for each variable by using the chi-square test for categorical variables and the Kruskal–Wallis test for continuous variables due to skewness of distributions. Moreover, we fitted quantile regressions on median scores to investigate the effect of the device on each concept (namely mobility, device satisfaction, and life satisfaction). The associations between concepts were also explored in a similar way. Each model adjusted for sex (female vs male), age group (≤64 vs >64), COPD severity (mild/moderate vs severe), and Medicare indicator. These statistical analyses were conducted using SAS 9.3 (SAS Institute, Cary, North Carolina). Two-sided P values < .05 were considered as statistically significant. We used partial least-squares structural equation modeling using Addinsoft's XLSTAT 2016 statistical software, a data analysis add-on for Excel (Microsoft, Redmond, Washington), to evaluate the relationship between device satisfaction and mobility as well as between QOL and both mobility and device satisfaction.
Results
Of the 529 survey respondents, 417 were included in the final data analysis, because 64 indicated that they used one LTOT device and 48 did not indicate the LTOT device used (Fig. 1). Table 3 shows the demographics of our analyzed sample for 417 subjects. The sample consisted of more females (81%), Medicare users (73%), subjects with severe COPD (80%), and subjects who were >64 y old (52%). Across device groups, the distributions were not statistically different for sex (P = .28) and COPD severity (P = .96), but were statistically different for age (P = .043) and Medicare (P < .001), since subjects in the liquid oxygen group tended to be older Medicare users than subjects in the other 2 device groups. Oxygen usage is summarized in Table 4. For our primary outcomes of interest, including perceived device satisfaction, mobility, and QOL, the trend in Table 5 was consistent, since there was a statistically significant difference in distribution across groups, and the liquid oxygen group showed higher scores than the portable oxygen concentrator (POC) and portable oxygen cylinder groups. All 3 outcomes showed statistical distributional difference in terms of P values (P < .001).

Flow chart. LTOT = long-term oxygen therapy.
Characteristics of Study Participants, Grouped by Long-Term Oxygen Therapy Device
Portable Oxygen Usage by 417 Study Subjects
Distribution of Scores for Perceived Satisfaction With Long-Term Oxygen Therapy Device, Perceived Mobility, and Perceived Quality of Life Across Type of Device Used by 417 Study Subjects
Results of the quantile regression analysis revealed that the median perceived device satisfaction score was significantly higher in the liquid oxygen device group (P < .001) compared with the portable oxygen cylinder and POC groups. The median perceived mobility score was significantly higher in the liquid oxygen device group (P = .02) compared with the portable oxygen cylinder group, but not the POC group. The median QOL score was significantly higher in the liquid oxygen device group (P < .001) compared with the POC and portable oxygen cylinder groups.
Mobility's Impact on and Contribution to Device Satisfaction, and Mobility and Device Satisfaction's Impact on and Contribution to Life Satisfaction
Results of the partial least-squares structural equation modeling regression analysis (summarized in Table 6) revealed that perceived satisfaction with an LTOT device has a significant effect on perceived mobility (adjusted R2 = 0.15, 99% CI 0.04–0.34, P < .001) (Fig. 2). This finding indicates that perceived satisfaction with an LTOT device moderately (f2 = 0.17) explains 15% of the variance in perceived mobility. COPD subjects' perceived QOL was also found to be affected by both perceived satisfaction with an LTOT device and perceived mobility (adjusted R2 = 0.45, 99% CI 0.29–0.68, P <. 001). This finding indicates that 45% of the variance in participants' perceived QOL is strongly (f2 = 0.37) explained by perceived satisfaction with an LTOT device and moderately (f2 = 0.13) explained by perceived mobility.

Impact and contribution of device satisfaction and mobility to the variance (R2) in perceived quality of life based on the values of the path coefficients (partial least-squares weights), which represent the hypothesized relationships linking device satisfaction and perceived mobility to perceived quality of life in the partial least-squares structural equation model.
Effect of Predictor Variables on Perceived Quality of Life
Discussion
Our study findings indicate that perceived satisfaction with an LTOT device affects perceived mobility in oxygen-dependent individuals with COPD. Additionally, we found that both perceived satisfaction with an LTOT device and perceived mobility affect perceived QOL in these individuals. Although various aspects of long-term oxygen therapy have been studied extensively, very few studies have focused on the impact of oxygen delivery devices on mobility and QOL. Moreover, the few studies that address this issue have been conducted in Europe and may not be reflective of the COPD population in the United States. The scarcity of research in this area may be attributed to the reality that Medicare reimbursement for LTOT is modality-neutral,22 which means that physicians are required to prescribe an oxygen flow but not the LTOT device. Additionally, it has been noted that LTOT is usually prescribed before the patient is discharged from the hospital by acute care physicians who may not have the requisite knowledge about LTOT devices to specify the most appropriate device for the patient in the prescription. Consequently, the selection of LTOT devices has been mostly left up to the suppliers of durable medical equipment.22
In this study of oxygen-dependent individuals with COPD, liquid oxygen system use significantly and positively affected mobility and QOL, whereas cylinder use significantly and negatively affected mobility and perceived QOL. Because mobility is a key determinant of satisfaction, it is understandable why oxygen devices that are perceived to increase mobility would result in a higher perceived QOL. COPD outcomes largely depend on adherence to the prescribed treatment regimen (including quitting smoking, if applicable), remaining physically active, and improving mental health.7,8 Some of the psychological hallmarks of COPD are feelings of isolation, depression, and anxiety.23 Many of these feelings may be directly related to lack of mobility due to the prescribed oxygen delivery device. If the device is too heavy, too conspicuous, too cumbersome, or too limiting and/or makes the user feel self-conscious, the patient may become withdrawn and less physically active. This in turn increases the likelihood of poor COPD symptom control and increased emergency room visits and hospitalizations. A meta-analysis of COPD health-care behavior self-management interventions24 found that physical activity improved HRQOL. The researchers postulated that physical activity contributes to less dyspnea and fatigue, with concomitant improvement in mental health and social engagement, resulting in improved HRQOL.
Based on comments from survey participants, size E cylinders are considered heavy, conspicuous, cumbersome, and limiting for many of these individuals. The following quotes from 4 of the survey participants highlight their perceived limitations to mobility imposed by portable LTOT devices:
Absolutely hate the E tanks that represent my portable unit. They are heavy, ugly and run out of O2 within 2 ½ h. My normal setting is 5 for activity. In the past, I was using a POC and then had to convert to D tanks using [a] home fill system to fill extra tanks for all trips away from home. I always encouraged COPD patients to stay active. Now, I find that I am the one that has slowed down almost to a stop.
I would be more mobile and better able to be independent if I had a more efficient portable O2 system. The tanks are heavy and take extra oxygen to even carry them. I've always maintained that if you can carry those heavy tanks you don't need O2.
The previous cylinders hinders us due to the weight. If you can't breathe, adding additional weight and [a] cumbersome device hinders a person's life that is already hindered.
The tank and shoulder bag I carry weigh 5 pounds. For some people that is not a lot, but I am a small woman who has lost a lot of strength over my years with COPD. It is bulky and hard to manage while cleaning house, working in the yard, taking care of a pet or children, etc.
It is clear from the results of this survey that this type of LTOT device may negatively affect the mobility and perceived QOL for oxygen-dependent persons with COPD. It must be noted that our survey sample consisted primarily of individuals who reported that they have severe (80%) and moderate COPD (17%).
Our survey results corroborate the findings of a previous Swedish study, which found that a liquid oxygen system as compared with a concentrator enhanced QOL in subjects with chronic hypoxemia as measured by the Sickness Impact Profile and the EuroQol instruments.25 The results of this study and our survey are not consistent with the findings of a study by Casaburi et al,26 in which COPD subjects with severe hypoxemia were randomized to use either E oxygen cylinders or lightweight cylinders (M-6 cylinders) weighing only 3.6 pounds. The researchers found that ambulatory oxygen use declined from baseline in COPD subjects who were given the lightweight oxygen cylinders. At the end of the study, there was no significant difference in the use of ambulatory oxygen between the 2 groups of subjects, indicating that lightweight LTOT devices did not improve mobility in those subjects.26 A significant limitation of the study by Casaburi et al26 is that it was underpowered; the authors noted that the sample size needed to detect an increase in daily oxygen use of 3 h in the lightweight LTOT device group was 100 participants, but only 17 participants completed the study. Additionally, the lightweight oxygen cylinder (M-6) that was used may not have been optimal for ambulation in this patient population due to fear of oxygen depletion. The authors stated that the lightweight device was set to deliver a pulse dose between 2 and 5 L/min, but this may not have been sufficient for these subjects during ambulation. Indeed, several studies have found that whereas oxygen-conserving devices meet the oxygen needs of subjects at rest, they may fail to do so during periods of activity due to various patient- and device-related factors.27–29
The results of our survey also conflict with the findings of a recent multi-center parallel group, randomized clinical trial30 of LTOT versus no LTOT in 738 subjects with COPD and moderate resting or exercise-induced desaturation. The results of this clinical trial indicate that ambulatory oxygen does not improve the QOL, as measured with the Quality of Well-Being scale in subjects with moderate or exercise-induced desaturation.30 However, this study had several significant limitations, including the use of different LTOT devices across participants in the various study centers. Moreover, the portable oxygen device used for ambulation was not specified. Additionally, 75% of the participants were male, which is not representative of the COPD population in the United States, where the COPD rate among women is higher than in men.1 The authors also reported significant bias in self-reported adherence to prescribed LTOT; consequently, the results of this clinical trial demonstrating no mortality benefit of LTOT should be interpreted with caution, given the complexity of COPD and the multiple factors that influence which individuals may benefit from oxygen supplementation.
Participant recruitment for our survey was achieved via an Internet-based method and is consistent with the growing trend among researchers of tapping into a more diverse population from the Internet.31 There is mounting evidence that results from research in which participants are recruited using Internet-based methods are as valid and reliable as results from research in which traditional means of participant recruitment are used. Casler et al31 compared results of a behavioral study from 3 different groups of participants who were recruited using the traditional method of recruiting undergraduate psychology students and using 2 Internet-based methods, namely crowd-sourcing and social media. The 3 different groups of participants were asked to complete a behavioral task, which was adapted to fit an online context for the online participants. The participants who were traditional undergraduate recruits completed the task one-on-one with an experimenter in a university lab test room,31 whereas the online participants were allowed to complete the task at their leisure. The study findings demonstrated that there was no difference between the 3 groups with regard to the expected behavioral outcome. It was also noted that the online participants were more diverse than the participants recruited via the traditional method and were more representative of the general population. The researchers concluded that participants recruited online can provide valid data. Health care-related studies, including clinical trials, are also increasingly relying on online recruitment to obtain more diverse participants, decrease recruitment costs, and increase the number of participants who enroll in a study, especially for studies of rare diseases and risky health behaviors in which participant recruitment by traditional methods is challenging.32–34
Since our study relied on self-reported data, the validity of results may be compromised due to limitations inherent in this study design, such as recall bias, respondents' ability to understand the survey questions, response bias, and differences in how respondents interpret the rating scales used in the survey. The variances in mobility and device satisfaction can also be attributed to differences in personal perceptions of satisfaction among individual survey participants. Although the survey asked participants to rank levels of satisfaction with their oxygen device, QOL, and mobility, it is difficult to truly assess personal preferences. Moreover, the degree of mobility that is considered acceptable to one individual may be perceived as severely limiting to another. Additionally, because study subjects were not selected at random, there may very well be selection bias in that the portable device that was in use at the time of the study may have been influenced by the subject's mobility at baseline. Finally, because 80% of study subjects were female with severe COPD and the ability to use the Internet, the study cannot be generalized to the entire COPD population.
Conclusions
The goal of our survey was to assess the impact of perceived satisfaction with LTOT devices on the perceived mobility and QOL of oxygen-dependent individuals with COPD. This study found that satisfaction with a portable LTOT device significantly and positively affects perceived mobility. Additionally, perceived QOL is significantly and positively affected by both perceived mobility and satisfaction with a portable LTOT device. Our findings have important implications relevant to the gap between the current evidence-based recommendation for COPD subjects to engage in routine physical activity and actual compliance, which may be attributable to the prescribed LTOT device. Future research is needed to investigate the association between various LTOT devices and physical activity, QOL, number of exacerbations, and survival in oxygen-dependent individuals with COPD.
Acknowledgments
We thank Dr Patricia Sawyer (University of Alabama at Birmingham [UAB] Comprehensive Center for Healthy Aging) for allowing us access to the UAB Study of Aging Life-Space Assessment and Bill Clark for facilitating posting of the survey on the COPD360SOCIAL social media site.
Footnotes
- Correspondence: Constance C Mussa PhD RRT-NPS, Rush University, AAC 765A, 600 S Paulina Street, Chicago, IL 60612. E-mail: Constance_Mussa{at}rush.edu.
The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant UL1TR002003. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Dr Mussa, Ms Tonyan, and Mr Vines presented a version of this report at AARC Congress 2016, held October 15–18, 2016, in San Antonio, TX.
Mr Vines has disclosed relationships with Aerogen, Bayer Healthcare, Boehringer Ingelheim, Carefusion, Covidien-Medtronic, Halyard, Salter Labs, and Teleflex. The other authors have disclosed no conflicts of interest.
See the Related Editorial on page 121
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}