

Abstract
BACKGROUND: Aerobic fitness, as measured by peak oxygen uptake (V̇O2 peak), correlates with survival in children and adults with cystic fibrosis (CF). We sought to evaluate the effects of V̇O2 peak on mortality rates in subjects with CF.
METHODS: An online search in PubMed, Embase, LILACS, and SciELO databases was conducted, and cohort studies that assessed mortality rates after oxygen absorption measurements during a maximal exercise test were included. Data were extracted independently by 2 reviewers. The quality analysis of the selected articles was performed using the Newcastle-Ottawa scale. The main outcome evaluated was the mortality of subjects with CF. Whenever possible, and if appropriate, a random effect meta-analysis was performed.
RESULTS: Six cohort studies were included in this systematic review including 551 subjects. Five studies were classified with high methodological quality. Two analyses were carried out to evaluate the influence of V̇O2 peak on mortality. Total difference standardized mean between V̇O2 peak averages in the survival or non-survival groups was −0.606 (95% CI = −0.993 to −0.219, P = .002). In addition, subjects with a lower V̇O2 peak had a significantly higher mortality risk (relative risk 4.896, 95% CI = 1.086 to 22.072, P = .039) in an 8-y follow-up period.
CONCLUSION: Low levels of peak oxygen uptake are associated with an increase of 4.9 in the risk of mortality in subjects with CF. This indicates that V̇O2 could be an important follow-up variable to measure, in addition to FEV1.
Introduction
Cystic fibrosis (CF) is a multisystemic genetic disease characterized by progressive loss of lung function and consequent limitation of aerobic fitness.1 Although morbidity and mortality are still a major concern in the disease management, life expectancy is increasing each year with advancement in the diagnosis and treatment; according to data from the Cystic Fibrosis Foundation, the expected median survival in the year 2015 was 41.7 y.2 Thus, as lung function is better maintained and aging of patients increases, other comorbidities rise and there is a growing importance of factors such as the preservation of aerobic fitness status.3
In general, many factors have been associated with a worse prognosis in individuals with CF, among them sex,4 decline in lung function,4–7 number of exacerbations,6,7 nutritional status,7–9 chronic colonization of the airways,10,11 and peak oxygen consumption (V̇O2 peak).5,11,12 It is known that the reduction of V̇O2 peak is of multifactorial origin, given that the mechanisms that can limit aerobic fitness include respiratory, cardiovascular, and of peripheral muscles.13 Therefore, performance on the cardiopulmonary exercise test (CPET) depends on more than lung function and thus reflects the effects of the disease on other organ systems earlier on,14 although FEV1 has still been cited as the best predictor of mortality in children and adults with CF.4,11,12 Thus, considering only lung function as a disease progression marker may not identify other factors that lead to morbidity and mortality in these subjects. Therefore, aerobic fitness evaluation through CPET seems to be a more comprehensive method.15
CPET is considered the gold standard for evaluating aerobic fitness and has been used not only to follow the evolution of the disease,16 because it evaluates the performance and interaction of the cardiovascular, respiratory, and metabolic systems,17 but also for the prescription of physical exercise.18 In addition, studies have shown high reproducibility of CPET for young19 and adult20 subjects with CF, demonstrating a coefficient of variation of 9.3% and 6.9%, respectively. Moreover, the recent statement on exercise testing in CF recommends performing CPET in individuals aged ≥ 10 y as an important part of the annual review process.15
Exercise intolerance due to hyperinflation and increased respiratory work caused by airway obstruction may be present as the disease advances,21 although it is increasingly common to find some pediatric patients who do not present dynamic hyperinflation during exercise. Aerobic fitness correlates with survival in children12 and adults5,11 with CF. Nixon et al11 was the first to demonstrate that V̇O2 peak (< 45 mL/kg/min) could be a predictor of survival in young individuals. A few years later, this finding was replicated by the study of Pianosi et al,12 which showed that subjects with V̇O2 peak > 82% of predicted had a better rate of survival.
Thus, we hypothesized that a low V̇O2 peak was an independent predictor of mortality in individuals with CF. Therefore, we performed a systematic review and quantitative meta-analysis of all available studies that reported the effects of peak oxygen consumption on mortality rates in individuals with CF.
Methods
This systematic review was performed following the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines,22 and data were described according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.23 The protocol of this review was registered in the international prospective register of systematic reviews and was accepted under the number CRD42016045759.
Search Strategy
Studies were identified from the following databases: PubMed, Embase, LILACS, and SciELO. The terms used were (“exercise test” or “exercise testing” or “cardiopulmonary exercise test” or “cardiopulmonary exercise testing” or “peak oxygen uptake” or “maximal oxygen consumption” or “exercise tolerance” or “exercise capacity”) and (“mortality” or “survival”) and (“cystic fibrosis”). No filters were used. A manual search was performed on the bibliographic references of the selected articles to search for additional publications that were pertinent to the study purpose. The searches were conducted in March 2017.
Study Selection
Two authors (FMV and JSdS) independently evaluated article titles and abstracts, thereby selecting the studies to be included in the review. Cohort studies of subjects with CF that assessed mortality rates after oxygen uptake measurements during a maximal exercise test were included. Articles that did not use variables of the maximal exercise test to predict mortality, articles that assessed the mortality of individuals already on the lung transplant list (because the inclusion of severely ill individuals would potentially bias the analysis), review studies, case studies, experimental models, abstracts, response letters, editorials, and duplicate publications, as well as those that did not meet inclusion criteria, were excluded after the analysis of the abstract or full text. Disagreements over the inclusion criteria of a particular study were discussed and resolved through consensus. A third author (MVFD) evaluated and resolved the discrepancies whenever disagreement or doubts between the 2 authors remained.
Data Extraction
The following data were extracted from each of the selected studies: title, first author's name, year of publication, country of origin, language of publication, type of study, age of subjects, sample size, type of equipment used, type of protocol used, duration of follow-up, V̇O2 peak, breathing reserve, ventilatory equivalent for peak oxygen consumption (V̇E/V̇O2), and ventilatory equivalent for carbon dioxide production (V̇E/V̇CO2). In addition, data from the variables of the cardiopulmonary exercise test and other variables that could predict the mortality of CF patients were collected. Any discrepancies were resolved by consensus among the researchers. Moreover, whenever appropriate, an attempt to contact authors of the included studies was performed in order to request additional information.
Quality Analysis
The quality analysis of the selected articles was performed individually by 2 authors (FMV and JPH-F) using the Newcastle-Ottawa Scale, which assigns a maximum of 9 points to the highest quality studies according to the 3 evaluated parameters: selection (4 points), comparability (2 points), and outcome (3 points).24 The overall quality of the study was defined as poor (score 0–3), reasonable (score 4–6), or high (score 7–9). The findings were discussed together with a third author (MVFD), and the discrepancies or doubts were resolved by consensus.
Synthesis of Data and Statistical Analysis
When possible and appropriate, a randomized meta-analysis of the studies was conducted. The standard difference of the V̇O2 peak averages between the survival and non-survival groups was performed by extracting the average data, sample size, and P value from each study included in that analysis. The association of high or low V̇O2 peak with mortality was calculated between the survival and non-survival groups by extracting the relative risk and the 95% CI and/or the number of events (death) and the total of participants in each group, using the DerSimonian-Laird randomized model.
Forest plots with the point size reflecting study weight were used to graphically represent the results of meta-analysis. The I2 and Q tests were used to quantify the degree of heterogeneity between the studies. It was not possible to evaluate the bias of publication with the Egger's test due to the small number of studies included in each analysis. All analysis were performed in the comprehensive meta-analysis software (Biostat, Englewood, New Jersey).
Results
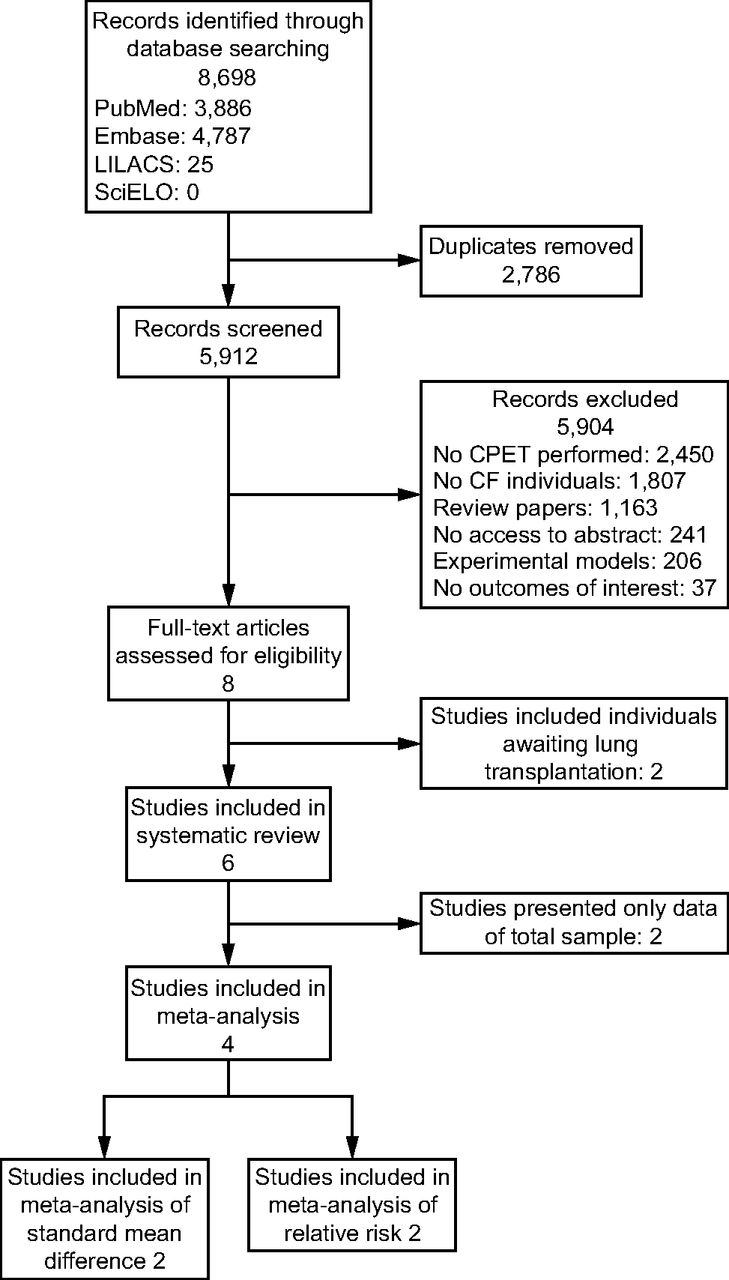
A total of 8,698 articles were found (3,886 in PubMed, 4,787 in EMBASE, and 25 in LILACS). Of these, 2,786 studies were excluded because they were repeated in the database searches, and 5,904 studies were excluded because they did not meet the eligibility criteria of our study. Eight studies were assessed for eligibility, and after analysis of the full text, 2 studies were excluded for including individuals already on a transplant list.25,26 Therefore, 6 studies were included in this review, and 4 studies were included in the meta-analysis. Figure 1 shows the flow chart of the articles found and the reasons for the exclusion of studies.

Flow chart. CPET = cardiopulmonary exercise testing; CF = cystic fibrosis.
The selected articles included a total of 551 subjects, and the sample size of each study varied between 28 and 149 subjects, with ages ranging from 10 to 30.2 y and follow-up time between 2.8 and 8 y (Table 1). Only 2 studies presented CFTR genotype classification, although no separate analyses were performed.9,10 All studies used the cycle ergometer to perform CPET. However, when evaluating the type of protocol, 3 studies used the Godfrey protocol,9–11 2 performed a ramp protocol,5,27 and 1 study12 used a step increment. The V̇O2 peak, breathing reserve, V̇E/V̇O2, and V̇E/V̇CO2 data from each article are presented in Table 2.
Main Methodological Characteristics of the Studies
Main Results of Cardiopulmonary Exercise Test Variables of the Studies Included in the Systematic Review
Regarding the overall methodological quality, 5 of the included studies5,9,11,12,27 were classified as high quality, and two5,11 of these received the maximum score (9 points). On the other hand, only 1 article10 was classified as reasonable quality and was assigned 6 points. Table 3 presents the parameters evaluated in the Newcastle-Ottawa Scale.
Newcastle-Ottawa Scale: Methodological Quality of Cohort Studies Included in the Systematic Review
Table 4 shows the data of significant variables to predict mortality in CF subjects. V̇O2 peak was significant in 5 studies,5,9–12 and breathing reserve was significant in 1 study.9 In the study by Nguyen et al,27 only the arterial-alveolar oxygen gradient was significant. With regard to other variables, FEV1 was significant in 5 studies,5,9,11,12,27 body mass index (BMI) was significant in 2 studies,9,27 and Pseudomonas cepacia colonization was significant in 1 study.11 To determine the influence of CPET variables on the mortality of subjects with CF, 3 studies9,11,12 used Cox proportional hazards, whereas the other 3 studies used log rank tests,10 multivariate logistic regression,27 and chi-square tests.5
Variables Used as Mortality Predictors in Patients with Cystic Fibrosis
Meta-analysis
Two different analyses were carried out to evaluate the influence of V̇O2 peak on mortality in subjects with CF, and 2 studies were included in each analysis. Figure 2A shows data from articles reporting differences between averages of V̇O2 peak in the survival and non-survival groups. The I2 analysis did not show heterogeneity between studies (I2 = 0%, P = .84). The total difference standardized mean was −0.606 (CI 95% = −0.993 to −0.219, P = .002), indicating that subjects in the non-survival group had a lower V̇O2 peak compared to survivors.

Meta-analysis of studies that reported mean difference in V̇O2 peak between survival or non-survival groups (A) and the association (relative risk, 95% CI) of V̇O2 peak (high vs. low–moderate) with mortality (B). Low V̇O2 peak was considered when < 45 mL/kg/min or 82% of predicted.
Subjects with a lower V̇O2 peak (< 45 mL/kg/min or < 82% of predicted) were associated with a significantly higher risk for mortality (relative risk 4.896, 95% CI = 1.086 to 22.072, P = .039). There was a small but not significant heterogeneity in the studies (I2 = 31.56%, P = .23) included in this analysis (Fig. 2B). It was not possible to generate funnel charts in the analysis because of the small number of studies included.
Discussion
Low aerobic fitness has been reported in individuals with CF and is associated with several factors, including impairment of lung function,28 poor nutritional status,29 low muscle power,28 cardiac dysfunction,30 high level of inflammation,10 and physical deconditioning.28 V̇O2 peak, defined as the peak amount of oxygen that can be transferred and utilized during exercise, is the main parameter in the evaluation of aerobic capacity.18 Our systematic review and meta-analyses demonstrate that subjects with lower V̇O2 peak rates (ie, values < 82% of predicted or 45 mL/kg/min) demonstrated a 4.9-fold increased risk for a fatal outcome, indicating that measurement of aerobic fitness could be a tool for prognosis in patients with CF. Furthermore, the difference between means indicated that subjects in the non-survival group had a lower V̇O2 peak compared to the survivors. This association of oxygen consumption with mortality has also been described for individuals with COPD31,32 and chronic heart failure.33,34 To our knowledge, this is the first meta-analysis to evaluate the association of V̇O2 peak with mortality in subjects with CF.
Nguyen et al27 was the only study included that found no relationship between V̇O2 peak and mortality. They demonstrated only that alveolar-arterial gradient for oxygen at peak exercise was significantly associated with mortality. On the other hand, the remaining articles demonstrated an association between V̇O2 peak and mortality. However, other variables, including FEV1 and BMI, were also significant in predicting mortality. A higher BMI has been associated with an increased likelihood of survival in subjects with CF,7–9,35 corroborating the results from Nguyen et al27 and Hulzebos et al.9 Furthermore, FEV1 has been considered the best predictor of mortality in subjects with CF,4,11,12 including those on lung transplant lists.36 According to Kerem et al4 individuals with FEV1 < 30% of predicted should be referred for lung transplantation. Moorcroft et al5 showed that, despite the correlation of V̇O2 peak with survival, FEV1 is still the best indicator of prognosis. On the other hand, Rosenthal37 described that lung function between 8 y and 12 y was a poor indicator of the risk of dying or being transplanted. Moreover, Pianosi et al12 demonstrated that the change in V̇O2 peak over time is more useful as a prognostic marker than the commonly used longitudinal decline in FEV1. In addition, abnormalities in aerobic fitness in early disease in stable subjects may reflect changes that are not detected with spirometry, given that Dodd et al38 have demonstrated that the correlation between thoracic computed tomography abnormalities and exercise limitation is stronger than the correlation between spirometry and BMI with exercise limitation. Thus, it is possible that V̇O2 peak is a better prognostic marker early in life than FEV1, considering that CPET is dependent on more than lung function and thus reflects the effects of the disease on other organ systems earlier on; however, further studies are needed to directly address this question.
Information obtained through CPET plays an important role in the care and follow-up of patients with CF because of its contribution to prognosis and functional information.18 Thus, an annual follow-up of V̇O2 peak is relevant to identify individuals at risk for a worsening prognosis,15 as well as those who may benefit from more intense therapy,39 considering that aerobic fitness correlates with survival in children12 and adults5,11 with CF. In addition, it is well-established that exercise increases V̇O2 peak, indicating its importance as a therapeutic tool that could influence prognosis.40
The studies included in this systematic review and meta-analysis showed variation in follow-up time, ranging from 2.8 y to 8 y. Considering that these are studies to evaluate mortality, a short follow-up time may be considered as a limitation because it could influence this outcome. In addition, it is already known that the evolution of CF is characterized by a decline in lung function and exercise limitation,1 highlighting the role of long-term follow-up periods in the evaluation of mortality rates.
As for the reported variables of CPET, the included studies showed a large variability, which prevented us from including some articles in certain analyses and to evaluate the influence of other variables such as ventilatory reserve data, V̇E/V̇O2, and V̇E/V̇CO2. A high breathing reserve index at the lactate threshold represents a reduction of pulmonary mechanical reserve and was already reported as a predictor of mortality in individuals with CF waiting for lung transplantation.25 In addition, V̇E/V̇O2 measurement has also been shown to be important in predicting mortality.5,9 Despite the relevance of the analyzed variables, it is important to recognize that CPET is not widely available in CF centers and requires specific equipment and expert personnel to perform and interpret the test. On the other hand, increasing life expectancy and new therapeutic options are changing the clinical presentation of CF, and markers such as lung function are better maintained over time, highlighting the importance of other factors such as aerobic fitness. Thus, studies designed to evaluate the prognostic value of CPET as compared to nutritional status, lung function, and other exercise tests are needed to further understand the role of aerobic fitness as a disease progression marker in CF.
Regarding the methodological quality of the studies included, in general, a high quality was found because only 1 study10 presented a reasonable classification according to the Newcastle-Ottawa Scale, which strengthens our systematic review and meta-analysis. In addition, the I2 test in the analysis of the difference between means did not show heterogeneity, and the relative risk analysis showed a low heterogeneity among the included studies, which may confirm the power of the analysis presented, despite the small number of articles.
One of the main limitations of this study is the small number of articles included in each analysis and the variability of the parameters evaluated. Due to the different presentations of data, only 2 articles were included in each of the analyses. Therefore, it was not possible to perform a funnel chart to evaluate publication bias of the studies. A short follow-up period, especially for a population of young children and adolescents, may also be considered a limitation in the evaluation of mortality. Two studies9,10 included subjects from the same CF center and with similar characteristics, which may include some shared members of a cohort. In addition, the lack of response when we tried to contact the authors of some of the studies9–12 to request additional V̇O2 peak information distinguished between survivors and non-survivors may be considered a limitation of present study.
Conclusions
This systematic review and meta-analysis showed that a low level of peak oxygen uptake is associated with higher mortality in CF, as subjects with reduced V̇O2 peak had a 4.9-fold increased risk for a fatal outcome. This indicates that V̇O2 peak may be an important follow-up variable to measure in addition to FEV1, although data from our analyses should be interpreted with caution due to the small number of studies included. Moreover, comparisons between aerobic capacity variables, FEV1, and BMI as mortality predictors in CF need to be further explored in future studies.
Footnotes
- Correspondence: Márcio Donadio, Laboratory of Pediatric Physical Activity, Centro Infant, Institute of Biomedical Research, Av. Ipiranga, 6690, 2° andar, Porto Alegre, Rio Grande do Sul, CEP 90610-000, Brazil. E-mail: mdonadio{at}pucrs.br
The authors have disclosed no conflicts of interest.
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}